Last Friday, the Centers for Medicare and Medicaid Services (CMS) announced that it will begin phasing in major Medicare Advantage (MA) risk-adjustment changes over a three-year period, slower than previously anticipated. Thanks to this delay in full implementation, MA plans will see an average 3.3 percent payment increase in 2024, up from the one percent projected in the earlier draft notice.
CMS also finalized regulations this week that aim to limit MA prior authorizations and denials by requiring that coverage decisions align with traditional Medicare.
The Gist: After CMS began proposing changes to MA payment formulas last year, aimed at reining in pervasive abuses and fraud,
the insurance industry responded with a $13M marketing blitz to oppose the changes.
The ads, one of which aired during the Super Bowl, tied Medicare Advantage “cuts” to the time-tested “Hands Off My Medicare” messaging directed at seniors.
With MA enrollment projected to overtake traditional Medicare this year,the federal government finds itself walking a tightrope in clamping down on overpayments to MA plans, given that any reductions will impact a growing number of seniors.
On Wednesday, UnitedHealth Group (UHG) announced that it will reduce its prior authorization claims volume by 20 percent for its commercial, Medicare Advantage, and Medicaid businesses later this year. Next year, it will launch a “gold card” program for qualifying providers that will further streamline care approvals. Cigna also shared that it has removed nearly 500 services from prior authorization review since 2020, relying on an electronic process for faster response times. These changes come in the wake of a Centers for Medicare and Medicaid Services (CMS) proposed rule, set to be finalized in April, that aims to streamline prior authorization by requiring certain payers to establish a method for electronic transmission, shorten response time for physician requests, and provide a reason for denials.
The Gist: These changes address two of providers’ primary complaints around prior authorizations: there are too many of them, and payers take too long to process them. However, technology options aiming to solve this problem through automation are by no means a foolproof solution.
As ProPublica recently reported, algorithm-based electronic claims processing solutions that improve response times can create other challenges, including improper automatic denials, and can expand prior authorization to lower-cost services, for which it was previously determined to be inefficient to rely on human review. Quicker responses must still be accurate and fair, necessitating that insurance companies closely monitor, audit, and hone technology solutions.
This week, the Centers for Medicare and Medicaid Services (CMS) finalized a 2018 proposed rule that will impose aggressive audits on Medicare Advantage (MA) insurers. By extrapolating the audits to insurers’ entire contracts, CMS expects to claw back almost $500M annually in overpayments since 2018, but has opted not to extrapolate the audits for 2011 to 2017. While MA insurers threaten to sue over the rule’s exclusion of a “fee-for-service adjustor” that would have reduced the degree of overpayments, CMS officials note that the estimated repayments under the final rule constitute less than 0.2 percent of total MA spending.
The Gist: This MA overpayment audit is overdue, especially given how well-documented MA overbilling has become. This week the Biden administration also announced a proposed change to MA risk adjustment that would reduce MA spending by $11B annually.
Though nearly half of all US seniors are now enrolled in MA plans, the program has yet to achieve its original purpose of saving the government money by encouraging competition around delivering care more efficiently.
MA cannot continue to cost more per enrollee than traditional Medicare in perpetuity, and an eventual reduction in per-member per-year payments is inevitable.
On Tuesday, the Centers for Medicare and Medicaid Services (CMS) announced a proposed rule that aims to streamline the prior authorization process by requiring certain payers to establish a method for electronic transmission, shorten response time for physician requests, and provide a reason for denials. This rule replaces one proposed in December 2020 that was never finalized.
In addition to applying to Medicaid and Affordable Care Act exchange plans, the new rule would also apply to Medicare Advantage plans, which the previous rule did not. If finalized, it will take effect in 2026.
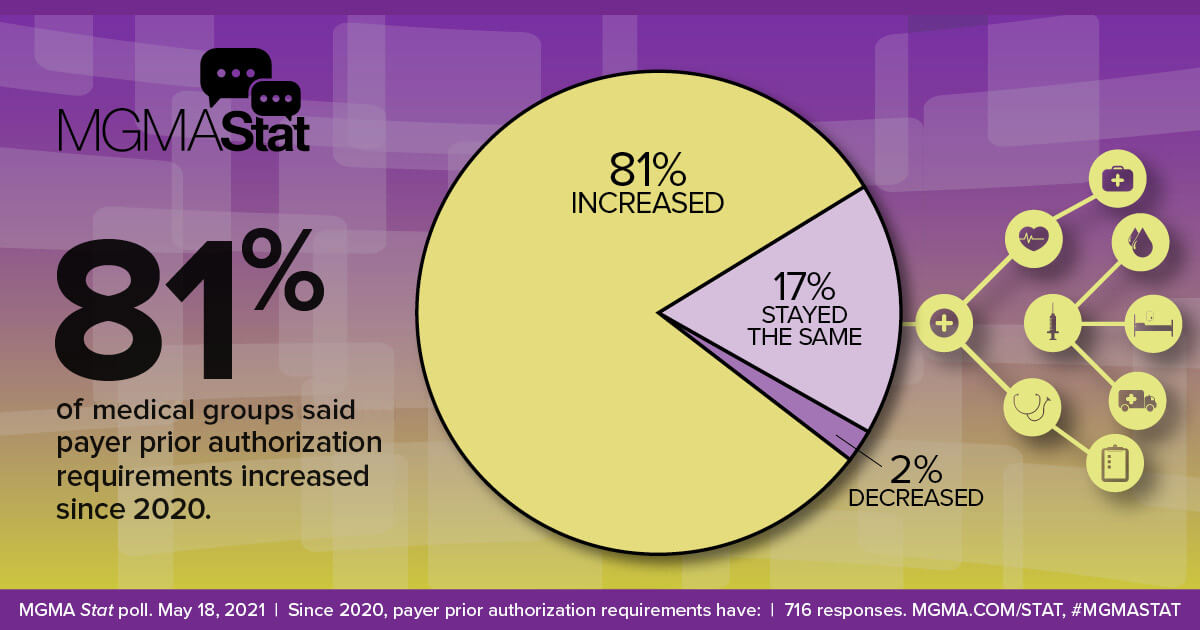
The Gist: Managing prior authorization requests is one of providers’ greatest sources of frustration, with over 80 percent of physicians rating it as “very or extremely burdensome” in a recent Medical Group Management Association survey.
Not only would patients would benefit from faster turnarounds, but even major payers agree that the status quo is suboptimal, and payer advocacy organization AHIP has signaled support for transmitting prior authorization requests electronically.
The challenge for regulators will be to strike a balance that satisfies the competing interests of payers and providers—turnaround time is likely to be a sticking point—but the one good thing about a system that no one likes is that there’s plenty of room for improvement.
Nearly 3.4 million people have signed up for 2023 Affordable Care Act insurance coverage since the start of open enrollment on Nov. 1, a record-setting pace that is a 17% boost over last year, new federal data shows.
The signup data released Tuesday by the Centers for Medicare and Medicaid Services shows a major hike in new signups on HealthCare.gov.
“We are off to a strong start — and we will not rest until we can connect everyone possible to healthcare coverage this enrollment season,” Department of Health and Human Services Secretary Xavier Becerra said in a statement Tuesday.
The nearly 3.4 million in signups represents activity through Nov. 19 on HealthCare.gov, which is used by residents in 33 states to pick an ACA plan, and through Nov. 12 for the 16 states and District of Columbia that run their own marketplaces.
There are 655,000 people who are new to the exchanges that picked a plan already, making up 19% of the total plan signups so far. CMS added that 2.7 million people who already have 2022 coverage renewed or selected a new plan for 2023.
“These plan selection numbers represent a 17% increase in total plan selections over last year,” CMS said in a release.
There is especially major growth on HealthCare.gov, which has seen 493,216 new enrollees compared to 354,137 for the same time period last year.
“Providing quality, affordable health care options remains a top priority,” said CMS Administrator Chiquita Brooks-LaSure in a statement. “The numbers prove that our focus is in the right place.”
The new signups come as the Biden administration made new investments in expansions for marketing and outreach, including record-setting funding for the ACA navigator program. Administration officials are hoping for another robust period of signups thanks to enhanced subsidies to lower insurance costs.
“Four out of five people will be able to find a plan for $10 or less after tax credits,” CMS said.
The boosted tax credits were supposed to expire after this year but have been extended into 2025 by the Inflation Reduction Act.
The 2022 coverage year saw a record 14.5 million signups. The latest open enrollment for HealthCare.gov for 2023 coverage will run through Jan. 15.
In their latest article scrutinizing the MA program, New York Times reporters Reed Abelson and Margot Sanger-Katz highlight MA marketing practices brought to light in a recent report from the Senate Finance Committee. Complaints to the Centers for Medicare and Medicaid Services (CMS) about MA marketing more than doubled from 2020 to 2021, as agents and brokers took advantage of oversight rules relaxed during the Trump administration. Some of the most egregious alleged abuses include agents switching seniors into new plans without their consent and exploiting individuals with cognitive impairments.
The Gist: Media interest is finally catching up to the building legislative and regulatory pressure on Medicare Advantage. While earlier reporting has highlighted how plans can inflate payments from Medicare, this new story shows how the process of selecting a plan can be fraught for the seniors enrolled.
Plan design is confusing even for industry insiders, so it is no surprise that seniors might find themselves ‘choosing’ plans that omit key providers, or even drug coverage they already rely on, particularly after being badgered or misled by agents and brokers.
Many of the regulatory fixes highlighted in the report can be implemented directly by CMS, but insurers, who remember the managed care backlash of the 90s, shouldn’t wait to tighten the reins on questionable marketing practices, lest they risk losing public support for one of their most lucrative business lines.
Physicians are set to see a 4.5 percent decrease in Medicare payment next year, in part due to the expiration of a temporary payment boost that was passed by Congress in December 2021 to avert scheduled sequester cuts. Physician groups are expected to lobby lawmakers heavily in the final months of the year, hoping to secure a reprieve, especially as inflation and labor costs continue to rise.
Other changes in the 2023 rules include advance payments to new participants in the Medicare Shared Savings Program, intended to boost participation of providers in rural and underserved areas. Some pandemic-era telehealth flexibilities that are set to expire with the end of the federal COVID public health emergency were also extended.
The Gist: We do not expect the full Medicare physician reimbursement cut to physicians to go into effect, as a bipartisan group of Senators has already asked leadership to address it in the upcoming lame-duck session. However, the cut serves the important purpose ofrebasing negotiations between physician lobbies and Congress, such that keeping rates flat or obtaining a small boost would feel like a win for both groups—even if it falls far short of the rate increases needed to meet the rising cost of running a practice.
If Congress continues to intervene to push off or mitigate Medicare’s sequestration payment reductions, we could find ourselves back in a Sustainable Growth Rate (SGR)-type situation where a payment cut constantly looms, physicians continually lobby for yet another reprieve, and the delayed cuts balloon in size.
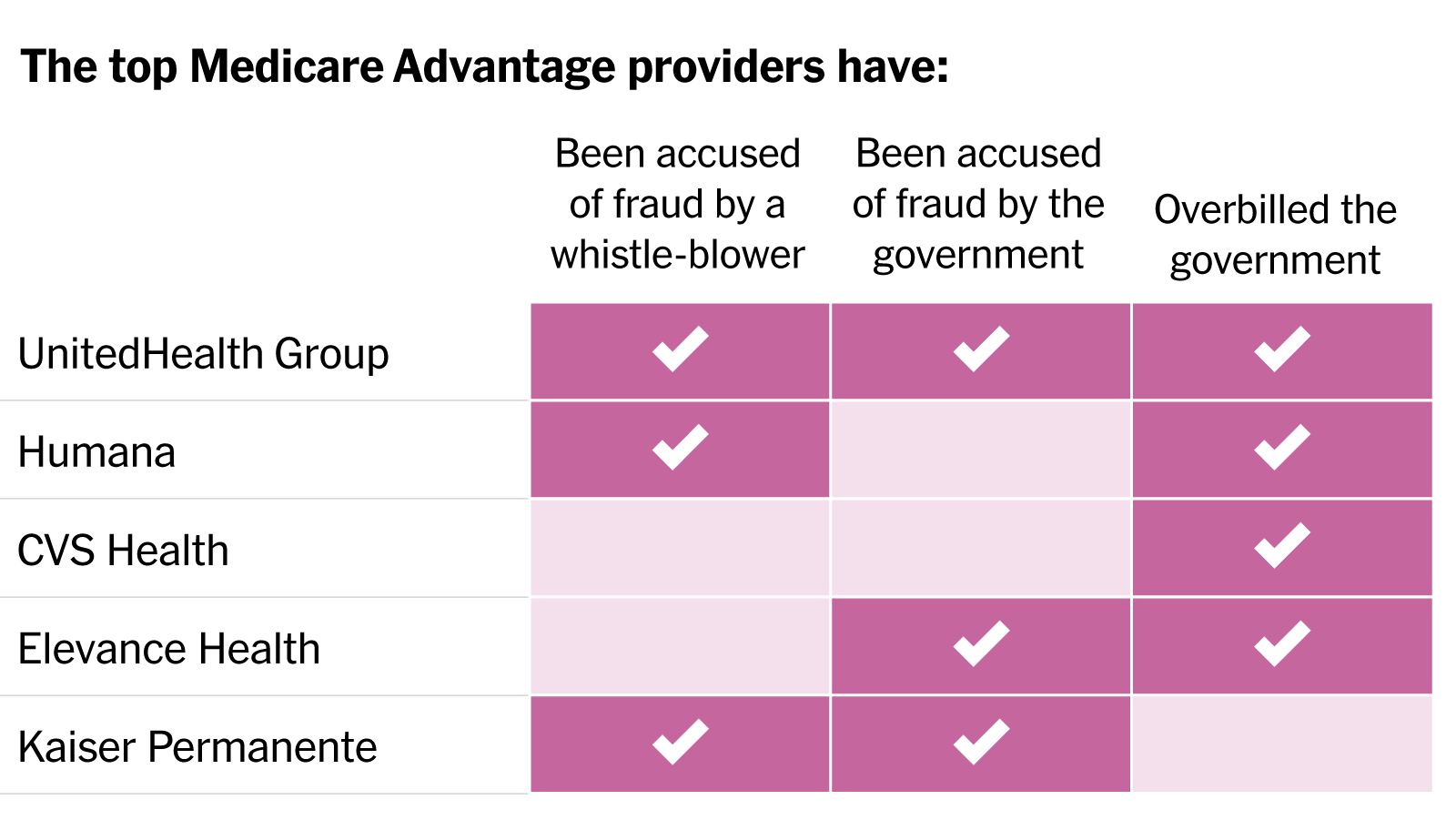
In a blistering article published in the New York Times, reporters Reed Abelson and Margot Sanger-Katz detail widespread fraud allegations involving the nation’s largest MA insurers. Nine of the ten largest plans have been accused by the government of fraud or overbilling, generally for upcoding practices that exaggerate the disease burden among their beneficiaries, without providing them more care. Insurers have disputed most allegations, and regulators have been slow to punish known infractions. As a growing steam of seniors continue the enter the program, aggressive risk adjustment has significantly increased the government’s costs. The Centers for Medicare and Medicaid Services has yet to reduce payments in response to overbilling, despite having the power to do so.
The Gist: While these practices were well known to many in the healthcare industry, MA’s growth—set to overtake traditional Medicare enrollment next year—has added a spotlight worthy of national attention. While many beneficiaries report being satisfied with their MA benefits, the program was also intended to improve the cost efficiency of senior care.
With payers gaming the system to garner record profits, the government has seen higher per-enrollee spending in MA compared to traditional Medicare. There are some signs that the strings are starting to tighten for insurers, as many of the largest are losing Medicare star bonuses in 2023, impacting both plan revenue and ability to market throughout the year. However, reduced quality bonuses change nothing about the underlying MA payment structure, and could even drive insurers to more profit-seeking behavior.
The court ruling comes after the Supreme Court struck down a nearly 30 percent cut to 340B hospital payments from 2018.
October 04, 2022 – A federal judge has ordered HHS to immediately end the almost 30 percent cut in Medicare drug reimbursement to 340B hospitals.
The decision published last week by judge Rudolph Contreras with the US District Court for the District of Columbia rejected HHS’ plan to restore full payment to hospitals participating in the 340B Drug Pricing Program in 2023.
“HHS should not be allowed to continue its unlawful 340B reimbursements for the remainder of the year just because it promises to fix the problem later,” wrote Contreras.
Hospitals participating in the 340B Drug Pricing Program receive outpatient prescription drugs at a discounted price of up to 50 percent since they treat a disproportionate amount of low-income and vulnerable patients. The 340B Program is designed to enable the safety-net providers to stretch their financial resources. Medicare must also reimburse hospitals for administering covered outpatient drugs.
HHS reduced the Medicare drug reimbursement rates for 340B hospitals though in 2018, cutting payments by 28.5 percent in an effort to generate about $1.6 billion in savings. Federal officials reasoned that reimbursing 340B hospitals at the same rate as other hospitals creates an incentive for the hospitals to overprescribe the drugs or prescribe more expensive drugs since they receive covered outpatient drugs at a discounted price.
HHS also argued that 340B hospital reimbursement cuts would lower co-payments for Medicare beneficiaries since the amounts are tied to hospital reimbursement rates.
Hospitals and hospital groups, including the American Hospital Association (AHA) Association of American Medical Colleges (AAMC), and American’s Essential Hospitals, sued the federal government over the reduced reimbursement rates.
The case made it all the way to the Supreme Court where, in a major win for hospitals, judges unanimously ruled that HHS should not have reduced payments to certain hospitals in 2018 and 2019 without surveying hospitals to determine average acquisition costs for drugs. HHS had relied on the average price of the drugs to set lower rates.
However, the Supreme Court did not make judgments on 340B hospital reimbursement cuts for 2020 and later years. Following the Supreme Court’s ruling, HHS announced it would reimburse hospitals for administering 340B-covered drugs the same as non-340B drugs starting Jan. 1, 2023.
Hospital groups again challenged HHS policy, asking the courts to immediately halt the unlawful cuts in 2022.
“The AHA appreciates Judge Contreras’ ruling that the Department of Health and Human Services must immediately stop unlawful reimbursement cuts for 2022 for hospitals participating in the 340B drug pricing program. Halting these cuts will help 340B hospitals provide comprehensive health services to their patients and communities,” said Melinda Hatton, AHA’s general counsel and secretary, regarding the most recent court ruling.
“We continue to urge the Administration to promptly reimburse all the hospitals that were affected by these unlawful cuts in previous years and to ensure the remainder of the hospital field is not penalized for their prior unlawful policy, especially as hospitals and health systems continue to deal with rising costs for supplies, equipment, drugs and labor,” Hatton continued in the public statement.
340B Health’s president and CEO Maureen Testoni also called the court ruling “an important victory for 340B hospitals that have been fighting these unlawful cuts for nearly six years.” 340B health advocates safety-net hospitals participating in the drug pricing program.
“The Centers for Medicare & Medicaid Services (CMS) has the clear responsibility to restore the appropriate payments for 340B drugs immediately, and now a federal court has ordered it to do so without delay,” Testoni said.
HHS has not announced a repayment plan for 340B hospitals. Notably, the court ruling also did not cover the AHA’s motion to include reimbursement cuts from 2020 through 2022 in the case, nor AHA’s motion to repay hospitals for the cuts since 2018 without penalizing other hospitals.
A Kaiser Health News analysis of federal data published Sept. 9 highlights an increasing trend among hospitals — establishing independent, nonprofit health center “look-alikes” for primary care patients to improve their financial picture.
Federally qualified health center look-alikes, as designated by the federal government, deliver primary care services to underserved communities. They receive federally qualified health center prospective payment system reimbursement through CMS — a higher rate than if the sites were owned by the hospitals — as well as help with the recruitment and retention of primary care providers via HHS’ National Health Service Corps.
However, they don’t receive health center program funding from HHS to cover operational expenses.
Some hospitals increasingly view look-alikes as a strategy to help with their financial picture, since they can divert primary care patients without urgent needs to look-alike clinics from expensive emergency rooms, according to Kaiser Health News.
The Kaiser Health News analysis published Sept. 9 found that at least eight hospitals and health systems have converted or built new clinics designated as look-alikes from 2019 through 2022. This includes Mount Carmel, Ill.-based Wabash General Hospital, Beverly Hospital in Montebello, Calif., and Parrish Medical Center in Titusville, Fla., among others.
To read the full Kaiser Health News report, click here.