One hesitates to elevate obviously bad arguments, even to point out how bad they are. This is a conundrum that comes up a lot these days, as members of the media measure the utility of reporting on bad faith, disingenuous or simply bizarre claims.
If someone were to insist, for example, that they were not going to get the coronavirus vaccine solely to spite the political left, should that claim be elevated? Can we simply point out how deranged it is to refuse a vaccine that will almost certainly end an international pandemic simply because people with whom you disagree think that maybe this is a good route to end that pandemic? If someone were to write such a thing at some attention-thirsty website, we certainly wouldn’t want to link to it, leaving our own readers having to figure out where it might be found should they choose to do so.
In this case, it’s worth elevating this argument (which, to be clear, is actually floating out there) to point out one of the myriad ways in which the effort to vaccinate as many adults as possible has become interlaced with partisan politics. As the weeks pass and demand for the vaccine has tapered off, the gap between Democratic and Republican interest in being vaccinated seems to be widening — meaning that the end to the pandemic is likely to move that much further into the future.
Consider, for example, the rate of completed vaccinations by county, according to data compiled by CovidActNow. You can see a slight correlation between how a county voted in 2020 — the horizontal axis — and the density of completed vaccinations, shown on the vertical. There’s a greater density of completed vaccinations on the left side of the graph than on the right.
If we shift to the percentage of the population that’s received even one dose of the vaccine, the effect is much more obvious.
This is a relatively recent development. At the beginning of the month, the density of the population that had received only one dose resulted in a graph that looked much like the current density of completed doses.
If we animate those two graphs, the effect is obvious. In the past few weeks, the density of first doses has increased much faster in more-Democratic counties.
If we group the results of the 2020 presidential contest into 20-point buckets, the pattern is again obvious.
It’s not a new observation that Republicans are less willing to get the vaccine; we’ve reported on it repeatedly. What’s relatively new is how that hesitance is showing up in the actual vaccination data.
A Post-ABC News poll released on Monday showed that this response to the vaccine holds even when considering age groups. We’ve known for a while that older Americans, who are more at risk from the virus, have been more likely to seek the vaccine. But even among seniors, Republicans are significantly more hesitant to receive the vaccine than are Democrats.
This is a particularly dangerous example of partisanship. People 65 or older have made up 14 percent of coronavirus infections, according to federal data, but 81 percent of deaths. That’s among those for whom ages are known, a subset (though a large majority) of overall cases. While about 1.8 percent of that overall group has died, the figure for those aged 65 and over is above 10 percent.
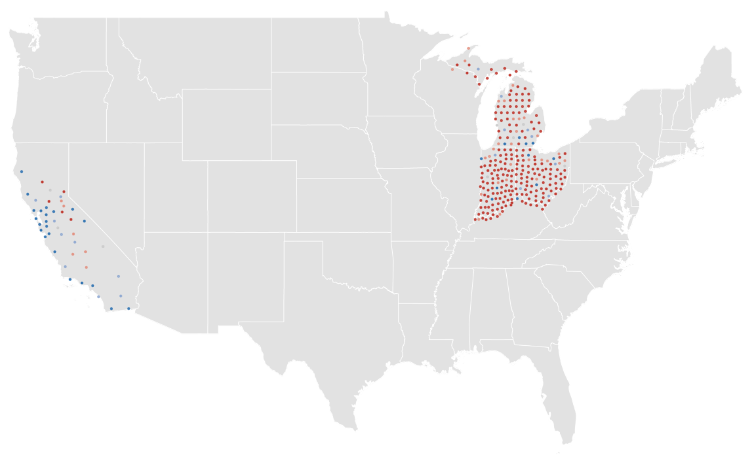
As vaccines have been rolled out across the country, you can see how more-heavily-blue counties have a higher density of vaccinations in many states.
This is not a universal truth, of course. Some heavily Republican counties have above-average vaccination rates. (About 40 percent of counties that preferred former president Donald Trump last year are above the average in the CovidActNow data. The rate among Democratic counties is closer to 80 percent.) But it is the case that there is a correlation between how a county voted and how many of its residents have been vaccinated. It is also the case that the gap between red and blue counties is widening.
Given all of that, it probably makes sense to point out that an argument against vaccines based on nothing more than “lol libs will hate this” is an embarrassing argument to make.
Europe seems poised to set the global standard for vaccine passports, now that European Commission President Ursula von der Leyen has signaled that vaccinated Americans will be allowed to travel to the continent this summer.
Why it matters: Opening up travel to vaccinated Americans will bring new urgency to creating some kind of trusted means for people to prove they’ve been vaccinated, Axios’ Felix Salmon reports.
The big picture: There will probably never be a single credential that most people use to prove they’ve been vaccinated, for every purpose.
But the EU’s system will help set a standard for a proof of vaccination that’s both easily accessible and difficult to forge.
The U.S. is being closely consulted on the European passport, so any future American system will likely use similar protocols.
Details: Informal mechanisms like simply asking someone whether they’re had a shot can suffice in many situations. A system for international travel will likely be far more stringent. And there’s a wide middle, too.
Other activities that don’t need the same rigorous standards as international travel could rely on the CDC’s vaccination cards; options like a printed QR code, similar to what’s been proposed by PathCheck; or a digital QR code, like the ones created by CommonPass or the Vaccine Credential Initiative.
The bottom line:The world of vaccine passports is almost certainly going to end up as a mishmash of different credentials for different activities, rather than a single credential used by everybody for everything.
Cambridge-based Massachusetts Institute of Technology professors Martin Bazant and John Bush, PhD, developed a model to calculate indoor exposure risk to COVID-19 by factoring in the amount of time spent inside, air filtration and circulation, immunization, variant strains, mask use, and respiratory activity such as breathing, eating or talking.
“We argue there really isn’t much of a benefit to the six-foot rule, especially when people are wearing masks,” Mr. Bazant told CNBC. “It really has no physical basis because the air a person is breathing while wearing a mask tends to rise and comes down elsewhere in the room so you’re more exposed to the average background than you are to a person at a distance.”
As with smoking, even people wearing masks can be affected by secondhand smoke that makes its way around the enclosed area and lingers. The same logic applies to airborne droplets of the virus, according to the study. However, the study did note that mask use by both infected and susceptible people reduces “respiratory plumes” and thus increases the amount of time people may safely spend together indoors.
When crafting guidelines, the CDC and World Health Organization have overlooked the amount of time spent indoors, Mr. Bazant claims.
“What our analysis continues to show is that many spaces that have been shut down in fact don’t need to be,” Mr. Bazant said. “Oftentimes, the space is large enough, the ventilation is good enough, the amount of time people spend together is such that those spaces can be safely operated even at full capacity, and the scientific support for reduced capacity in those spaces is really not very good.”
Opening windows or installing new fans to keep air moving may be just as effective or more effective than purchasing a new filtration system, Mr. Bazant said.
The CDC currently recommends staying at least 6 feet away from other people and wearing a mask to slow the spread of COVID-19, citing the fact that the virus spreads mainly among people who are in close contact for a prolonged period.
“The distancing isn’t helping you that much and it’s also giving you a false sense of security, because you’re as safe at six feet as you are at 60 feet if you’re indoors. Everyone in that space is at roughly the same risk, actually,” Mr. Bazant said.
After three rounds of peer review, Mr. Bazant says he hopes the study will influence social distancing policies.
There’s a lot of anxiety about the AstraZeneca vaccine thanks to recent reports of incomplete data, as well as reports on blood clot risks. Let’s take a look at both issues in context, understanding the efficacy data before and after numbers were updated, and understanding blood clot risk in relation to other common situations where blood clots are a potential concern.
For some time, we’ve been focused on the efforts of Walmart to launch and grow a care delivery business, especially as it has piloted an expanded primary care clinic offering in a handful of states. We’ve long thought that access to basic care at the scale that Walmart brings could be transformative, given that more than half of Americans visit a Walmart store every week. Along those same lines, we’ve always wondered why Dollar General and Dollar Tree—each with around four times as many retail locations as Walmart—haven’t gotten into the retail clinic or pharmacy businesses.
(Part of the answer is ultra-lean staffing—this piece gives a good sense of the basic, and troubling, economics of dollar stores.) Now, as the federal government ramps up its efforts to widely distribute the COVID vaccines, it turns out that the CDC is actively discussing a partnership with Dollar General to administer the shots.
A fascinating new paper (still in preprint) from researchers at Yale shows why this could be a true gamechanger. The Biden administration, through its partnership with national and independent pharmacy providers, aims to have a vaccination site within five miles of 90 percent of the US population by next week. Compared to those pharmacy partners, researchers found,Dollar General stores are disproportionately located in areas of high “social vulnerability”, with lower income residents and high concentrations of disadvantaged groups. Particularly in the Southeast, a partnership with Dollar General would vastly increase access for low-income Black and Latino residents, allowing vaccine access within one mile for many, many more people. And the partnership could form the basis for future expansions of basic healthcare services to vulnerable and rural communities, particularly if some of the $7.5B in funding for COVID vaccine distribution went to helping dollar store locations bolster staffing and equipment to deliver basic health services. We’ll be watching with interest to see if the potential Dollar General partnership comes to fruition.
As states rush to fully reopen businesses, and Americans leave their masks at home in greater numbers, it appears that the feared “fourth surge” of COVID is now underway in many parts of the country.Coronavirus cases are up in half of all states, and up nationally by 9 percent compared to last week. While the latest wave appears to be much less deadly—largely targeting younger people who haven’t yet been vaccinated—it adds urgency to the effort to get shots in arms as quickly as possible.
The good news: that’s happening. Today the US surpassed the milestone of 200M vaccinations given, with nearly a quarter of the population now fully vaccinated (including nearly two-thirds of those over age 65). The progress on vaccines comes as the Johnson & Johnson COVID jab is sidelined, over safety concerns stemming from a small number of rare blood-clotting cases in younger women that caused the Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC) to urge states to pause the use of the shot. Wednesday’s inconclusive meeting of the FDA’s Advisory Committee on Immunization Practices meant an additional 7 to 10 days of limbo for the J&J vaccine, drawing criticism from experts who warned that the negative publicity could undermine confidence in vaccines among the general population, both in the US and around the world.
Count us among those skeptical of the decision to pull back on the J&J vaccine, which plays a pivotal role in the campaign against COVID, given that it’s a single-dose vaccine that can be stored at normal refrigerator temperatures, making it more easily distributed than the two-dose mRNA vaccines. While the blood clotting cases are serious, and merit investigation, the odds of suffering a vaccine-related blood clot are far outweighed by an individual’s risk of death or severe complications from COVID itself, let alone the chances of getting a blood clot from other medications (such as oral contraceptives).
It was a big week for innumeracy, unfortunately: headlinesabounded about the CDC’s discovery of 5,800 “breakthrough” COVID cases, in which fully vaccinated people still contracted the disease. Unsurprisingly, the numerator got the headlines, not the denominator—the 80M people who’ve been fully vaccinated. Your chances of hitting a hole-in-one as an amateur golfer are better than the chances of getting COVID after being fully vaccinated. Furthermore, of those 5,800 people infected after being fully vaccinated, only 7 percent were hospitalized, and 74 died. Each a tragedy, to be sure—but we’ll take those odds any day.
We’re a year into the coronavirus pandemic, so the math that undergirds its risks should by now be familiar. We all should know, for example, that the ability of the virus to spread depends on it being able to find a host, someone who is not protected against infection. If you have a group of 10 people, one of whom is infected and nine of whom are immune to the virus, it’s not going to be able to spread anywhere.
That calculus is well known, but there is still some uncertainty at play. To achieve herd immunity — the state where the population of immune people is dense enough to stamp out new infections — how many people need to be protected against the virus? And how good is natural immunity, resistance to infection built through exposure to the virus and contracting covid-19, the disease it causes?
The safe way to increase the number of immune people, thereby probably protecting everyone by limiting the ability of the virus to spread, is through vaccination. More vaccinated people means fewer new infections and fewer infections needed to get close to herd immunity. The closer we get to herd immunity, the safer people are who can’t get vaccinated, such as young children (at least for now).
The challenge the world faces is that the rollout of vaccines has been slow, relatively speaking. The coronavirus vaccines were developed at a lightning pace, but many parts of the world are still waiting for supplies sufficient to broadly immunize their populations. In the United States, the challenge is different: About a quarter of adult Americans say they aren’t planning on getting vaccinated against the virus, according to Economist-YouGov polling released last week.
That’s problematic in part because it means we’re less likely to get to herd immunity without millions more Americans becoming infected. Again, it’s not clear how effective natural immunity will be over the long term as new variants of the virus emerge. So we might continue to see tens of thousands of new infections each day, keeping the population at risk broadly by delaying herd immunity and continuing to add to the pandemic’s death toll in this country.
But we also see from the Economist-YouGov poll the same thing we saw in Gallup polling earlier this month: The people who are least interested in being vaccinated are also the people who are least likely to be concerned about the virus and to take other steps aimed at preventing it from spreading.
In the Economist-YouGov poll, nearly three-quarters of those who say they don’t plan on being vaccinated when they’re eligible also say they’re not too or not at all worried about the virus.
That makes some perverse sense: If you don’t see the virus as a risk, you won’t see the need to get vaccinated. Unfortunately, it also means you’re going to be less likely to do things like wear a mask in public.
Or you might be more likely to view as unnecessary precautions such as avoiding close-quarter contact with friends and family or traveling out of state.
About a quarter of adults hold the view that they won’t be vaccinated when eligible. That’s equivalent to about 64 million Americans.
Who are they? As prior polls have shown, they’re disproportionately political conservatives. At the outset of the pandemic, there was concern that vaccine skepticism would heavily be centered in non-White populations. At the moment, though, the rate of skepticism among those who say they voted for Donald Trump in 2020 and among Republicans is substantially higher than skepticism overall.
That shows up in another way in the Economist poll. Respondents were asked whose medical advice they trusted. Among those who say they don’t plan to get the vaccine, half say they trust Trump’s advice a lot or somewhat — far more than the advice of the Centers for Disease Control and Prevention or the country’s top infectious-disease expert Anthony S. Fauci.
If we look only at Republican skeptics, the difference is much larger: Half of Republican skeptics say they have a lot of trust in Trump’s medical advice.
The irony, of course, is that Trump sees the vaccine as his positive legacy on the pandemic. He’s eager to seize credit for vaccine development and has — sporadically — advocated for Americans to get the vaccine. (He got it himself while still president, without advertising that fact.) It’s his supporters, though, who are most hostile to the idea.
Trump bears most of the responsibility for that, too. Over the course of 2020, worried about reelection, he undercut containment efforts and downplayed the danger of the virus. He undermined experts such as Fauci largely out of concern that continuing to limit economic activity would erode his main argument for his reelection. Over and over, he insisted that the virus was going away without the vaccine, that it was not terribly dangerous and that America should just go about its business as usual — and his supporters heard that message.
They’re still listening to it, as the Economist poll shows. One result may be that the United States doesn’t reach herd immunity through vaccinations and, instead, some large chunk of those tens of millions of skeptics end up being exposed to the virus. Some of them will die. Some may risk repeat infections from new variants against which a vaccine offers better protection. Some of those unable to get vaccinated may also become sick from the virus because we haven’t achieved herd immunity, suffering long-term complications from covid-19.
Trump wants his legacy to be the rollout of the vaccine. His legacy will also probably include fostering skepticism about the vaccine that limits its utility in containing the pandemic.