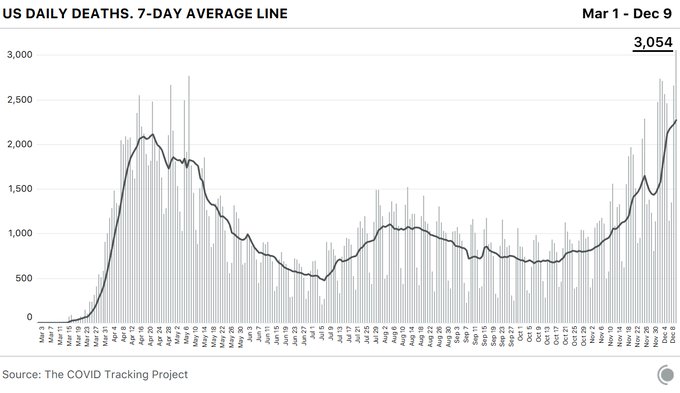
The coronavirus pandemic pushed the U.S. past another dire milestone Wednesday, the highest daily death toll to date, even while the mortality rate has decreased as health experts learn more about the disease.
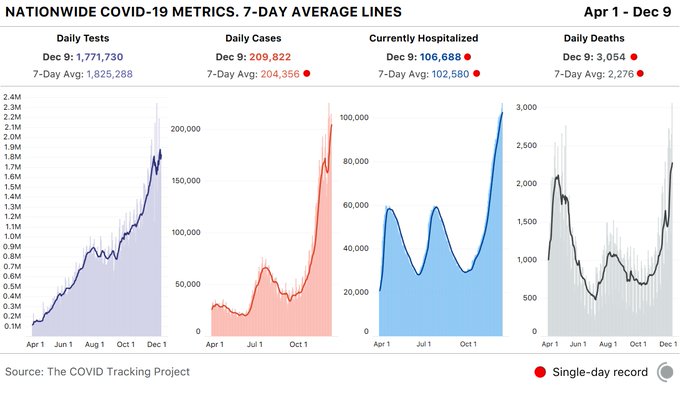
The Covid Tracking Project, which tracks state-level coronavirus data, reported 3,054 COVID-19 related deaths — a significant jump from the previous single-day record of 2,769 on May 7.
The spread of the disease has shattered another record with 106,688 COVID-19 patients in U.S. hospitals. And overall, states reported 1.8 million tests and 210,000 cases. According to the group, the spike represents more than a 10% increase in cases over the last 7 days.
Additionally, California nearly topped its single-day case record at 30,851. It is the second highest case count since December 6, the organization reported.
The staggering spike in fatalities and infections has overwhelmed hospitals and intensive care units across the nation, an increase attributed by many experts to people relaxing their precautions at Thanksgiving.
Dean Baquet, The Times’s executive editor, believes that 2020 will go down as a signature year in history, alongside years like 1968, 1945 and 1865. “It will long be remembered and studied as a time when more than 1.5 million people globally died during a pandemic, racial unrest gripped the world, and democracy itself faced extraordinary tests,” he writes.
Those words come from Dean’s introduction to The Times’s annual Year in Pictures feature. Here, my colleagues on The Morning and I have chosen a dozen of those pictures that we think best summarize 2020. But we obviously have room here for only a fraction of the year’s photographs — so I encourage you to check out the full selection.
As you do, ask yourself which pictures you would have selected if you had to pick only 12 to sum up 2020.
Early in the year, the virus hit Western Europe harder than any other place in the world. In March, a coronavirus patient was examined at his home in Cenate Sotto, Italy.The pandemic forced people to find new ways to socialize. Circles painted on the grass at Domino Park in Brooklyn helped people spend time safely outdoors in May.Donald Trump became only the fourth elected president in the last century not to win re-election, joining Herbert Hoover, Jimmy Carter and George H.W. Bush. Trump departed Air Force One in August after returning from a campaign rally.Joe Biden struggled badly early in the Democratic primaries, only to rally to win the nomination and the presidency. He prayed at the Corinthian Baptist Church in Des Moines in January.Climate change wrought destruction on the planet in multiple ways during 2020. In Azusa, Calif., a wildfire burned more than 4,200 acres during the most active wildfire year on record for the West Coast.The killing of George Floyd in May inspired mass demonstrations against police brutality across the country. In Minneapolis, officers confronted protesters on May 31.Protesters marched in New York in June as anger spread across the country.Around the world, people spent far more time at home this year than usual. In São Paulo, Brazil, residents gathered at their windows in March to protest the government’s pandemic response.The pandemic led to a sharp economic downturn in much of the world. In May, people lined up for food distribution at a church in Brooklyn.More than 1.5 million people around the world have died from Covid complications. Mourners gathered in April at a cemetery in Brazil where workers were busy digging lines of open graves.Amid illness, death and separation in 2020, people also experienced great joys — even if they sometimes required adaptation. In April, Precious Anderson, a Covid-19 patient, was shown her newborn baby for the first time with the help of a live video feed at a hospital in Brooklyn.
When Ashley Antonio contracted covid-19 in late March, the Canadian criminal lawyer fought against the common symptoms that come with most cases: fever, body aches, fatigue, headaches.
She would manage her symptoms at home and eventually overcome them, she assured herself. After all, she was a healthy 35-year-old with no underlying conditions who boxed and did strength training four times a week.
Except the symptoms never really went away — they intensified.
Now, 259 days later, Antonio is still suffering the repercussions of a virus that has upended almost every aspect of her life.
She has been in and out of the hospital four times in almost nine months. Her doctors have diagnosed Antonio with arthritis and a condition that causes her heartbeat to dramatically increase when she stands up. Both are long-term effects of the virus, they told her. They also don’t know if, and when, those symptoms will go away.
“Everyone is just told you either recover or you die,” Antonio told The Washington Post on Tuesday. “There’s never talk of all the people that are trapped somewhere in the middle with all of these long-term effects. We’re not recovered. We’re just not covid-positive anymore.”
Antonio is not alone. Doctors still aren’t sure why “long-haulers” continue to suffer the consequences of the disease months later or whether the symptoms will stay with them for the rest of their lives. But public health experts say it’s increasingly clear that many thousands of patients face long-term effects from the virus.
Long-haulers “are in every country, in every language,” Igor J. Koralnik, who started a program for covid-19 neurocognitive problems at Northwestern Memorial Hospital in Chicago, told The Post in October. “It’s going to be a big problem. It’s not going to go away.”
So far, clinicians have learned the long-term effects can impact both the old and the young, regardless of whether the case was mild or required hospitalization. Many long-haulers have turned to social media groups to share their experiences and advice.
Antonio, who lives in Edmonton and whose story was first reported by the CBC, said she had been taking precautions and working from home for a month before she got sick. Her best guess is that she caught the virus on a run to the grocery store. She began feeling symptoms around March 25.
But because she did not have a cough, which doctors and health experts then said was one of covid-19′s main symptoms, Antonio thought she only had a stomach flu.
She stayed home and started to feel like herself again days later. But every time she thought she was recovering, symptoms would return. In the next three months, old symptoms and new, graver ones left Antonio tied to her couch. The fatigue was so bad she could shower only a couple of times a week. Her blood oxygen levels would drop dangerously low whenever she took short steps. One day, her brain was so foggy that she could not remember how to hold a glass.
It wasn’t until mid-May when she was taken to the emergency room for the first time. Alone in her bedroom and fighting a high fever, Antonio began hallucinating. Then, she could not feel half of her body or her face. The hospital tested her for the coronavirus, but her results came back negative so she was sent home. About a week later, she was back. She would return two more times in the following months.
“I had every test you could imagine,” she said. But her doctors could still not figure out what exactly was wrong with her. An emergency room doctor suggested she might have long-term covid-19 effects and referred her to a special clinic.
In June, she tested positive for coronavirus antibodies. In July, doctors at a clinic for coronavirus survivors diagnosed her with arthritis and a condition that causes her heartbeat to raise significantly when standing. “But doctors couldn’t explain why my oxygen was still dropping every time I walked or any other symptoms,” she said.
Antonio turned to other long-haulers for more information, joining a Facebook group where she learned, for example, that she wasn’t alone in smelling cigarettes when no one was smoking near her. Other people experienced random smells too, they told her.
“I had a lot of questions and the doctors didn’t have a lot of answers. It was all so new to everyone,” Antonio said. “I just wanted to see if what I was experiencing was ‘normal.’ It was very comforting to know that I wasn’t alone.”
Although her symptoms persisted, in August, Antonio voluntarily returned to the law firm where she works as a criminal lawyer. Some days, she feels okay. But the increased heart rate, shortness of breath, joint pain and headaches are usually daily ailments. She also still suffers from blurry vision and gets skin rashes. Her doctors have now told her it’s possible that her long-term symptoms will come and go for the rest of her life. For now, Antonio said she is taking it one day at a time.
“I’m definitely worried it will be permanent,” she said. “It’s very overwhelming if I think that this is how the rest of my life is going to be.”
Antonio added: “When I have a good day, I no longer think that it will be over. I know I’ll have bad days again. It makes you feel hopeless.”
But there is still one dark cloud hanging over the vaccines that many people don’t yet understand.
The vaccines will be much less effective at preventing death and illness in 2021 if they are introduced into a population where the coronavirus is raging — as is now the case in the U.S. That’s the central argument of a new paper in the journal Health Affairs. (One of the authors is Dr. Rochelle Walensky of Massachusetts General Hospital, whom President-elect Joe Biden has chosen to run the Centers for Disease Control and Prevention.)
An analogy may be helpful here. A vaccine is like a fire hose. A vaccine that’s 95 percent effective, as Moderna’s and Pfizer’s versions appear to be, is a powerful fire hose. But the size of a fire is still a bigger determinant of how much destruction occurs.
I asked the authors of the Health Affairs study to put their findings into terms that we nonscientists could understand, and they were kind enough to do so. The estimates are fairly stunning:
At the current level of infection in the U.S. (about 200,000 confirmed new infections per day), a vaccine that is 95 percent effective — distributed at the expected pace — would still leave a terrible toll in the six months after it was introduced. Almost 10 million or so Americans would contract the virus, and more than 160,000 would die.
This is far worse than the toll in an alternate universe in which the vaccine was only 50 percent effective but the U.S. had reduced the infection rate to its level in early September (about 35,000 new daily cases). In that scenario, the death toll in the next six months would be kept to about 60,000.
It’s worth pausing for a moment on this comparison, because it’s deeply counterintuitive. If the U.S. had maintained its infection rate from September and Moderna and Pfizer had announced this fall that their vaccines were only 50 percent effective, a lot of people would have freaked out.
But the reality we have is actually worse.
How could this be? No vaccine can eliminate a pandemic immediately, just as no fire hose can put out a forest fire.While the vaccine is being distributed, the virus continues to do damage. “Bluntly stated, we’ll get out of this pandemic faster if we give the vaccine less work to do,” A. David Paltiel, one of the Health Affairs authors and a professor at the Yale School of Public Health, told me.
There is one positive way to look at this:Measures that reduce the virus’s spread — like mask-wearing, social distancing and rapid-result testing — can still have profound consequences. They can save more than 100,000 lives in coming months.
In the past seven days, 15,813 people in the U.S. died from the virus, breaking a record that had stood since mid-April.
Americans have made no secret of their skepticism of COVID-19 vaccines this year, with fears of political interference and a “warp speed” timeline blunting confidence in the shots. As recently as September, nearly half of U.S. adults said they didn’t intend to be inoculated.
But with two promising vaccines primed for release, likely within weeks, experts in ethics and immunization behavior say they expect attitudes to shift quickly from widespread hesitancy to urgent, even heated demand.
“People talk about the anti-vaccine people being able to kind of squelch uptake. I don’t see that happening,” Dr. Paul Offit, a vaccinologist with Children’s Hospital of Philadelphia, told viewers of a recent JAMA Network webinar. “This, to me, is more like the Beanie Baby phenomenon. The attractiveness of a limited edition.”
Reports that vaccines produced by drugmakers Pfizer and BioNTech and Moderna appear to be safe and effective, along with the deliberate emphasis on science-based guidance from the incoming Biden administration, are likely to reverse uncertainty in a big way, said Arthur Caplan, director of the division of medical ethics at New York University School of Medicine.
“I think that’s going to flip the trust issue,” he said.
The shift is already apparent. A new poll by the Pew Research Center found that by the end of November 60% of Americans said they would get a vaccine for the coronavirus. This month, even as a federal advisory group met to hash out guidelines for vaccine distribution, a long list of advocacy groups — from those representing home-based health workers and community health centers to patients with kidney disease — were lobbying state and federal officials in hopes their constituents would be prioritized for the first scarce doses.
“As we get closer to the vaccine being a reality, there’s a lot of jockeying, to be sure,” said Katie Smith Sloan, chief executive of LeadingAge, a nonprofit organization pushing for staff and patients at long-term care centers to be included in the highest-priority category.
Certainly, some consumers remain wary, said Rupali Limaye, a social and behavioral health scientist at the Johns Hopkins Bloomberg School of Public Health. Fears that drugmakers and regulators might cut corners to speed a vaccine linger, even as details of the trials become public and the review process is made more transparent. Some health care workers, who are at the front of the line for the shots, are not eager to go first.
“There will be people who will say, ‘I will wait a little bit more for safety data,” Limaye said.
But those doubts likely will recede once the vaccines are approved for use and begin to circulate broadly, said Offit, who sits on the FDA advisory panel set to review the requests for emergency authorization Pfizer and Moderna have submitted.
He predicted demand for the COVID vaccines could rival the clamor that occurred in 2004, when production problems caused a severe shortage of flu shots just as influenza season began. That led to long lines, rationed doses and ethical debates over distribution.
“That was a highly desired vaccine,” Offit said. “I think in many ways that might happen here.”
Initially, vaccine supplies will be tight, with federal officials planning to ship 6.4 million doses within 24 hours of FDA authorization and up to 40 million doses by the end of the year. The CDC panel recommended that the first shots go to the 21 million health care workers in the U.S. and 3 million nursing home staff and residents, before being rolled out to other groups based on a hierarchy of risk factors.
Even before any vaccine is available, some people are trying to boost their chances of access, said Dr. Allison Kempe, a professor of pediatrics at the University of Colorado School of Medicine and expert in vaccine dissemination. “People have called me and said, ‘How can I get the vaccine?’” she said. “I think that not everyone will be happy to wait, that’s for sure. I don’t think there will be rioting in the streets, but there may be pressure brought to bear.”
That likely will include emotional debates over how, when and to whom next doses should be distributed, said Caplan. Under the CDC recommendations, vulnerable groups next in line include 87 million workers whose jobs are deemed “essential” — a broad and ill-defined category — as well as 53 million adults age 65 and older.
“We’re going to have some fights about high-risk groups,” said Caplan of NYU.
The conversations will be complicated. Should prisoners, who have little control over their COVID exposure, get vaccine priority? How about professional sports teams, whose performance could bolster society’s overall morale? And what about residents of facilities providing care for people with intellectual and developmental disabilities, who are three times more likely to die from COVID-19 than the general population?
Control over vaccination allocation rests with the states, so that’s where the biggest conflicts will occur, Caplan said. “It’s a short fight, I hope, in the sense in which it gets done in a few months, but I think it will be pretty vocal.”
Once vaccine supplies become more plentiful, perhaps by May or June, another consideration is sure to boost demand: requirements for proof of COVID vaccination for work and travel.
“It’s inevitable that you’re going to see immunity passports or that you’re required to show a certificate on the train, airplane, bus or subway,” Caplan predicted. “Probably also to enter certain hospitals, probably to enter certain restaurants and government facilities.”
But with a grueling winter surge ahead, and new predictions that COVID-19 will fell as many as 450,000 Americans by February, the tragic reality of the disease will no doubt fuel ample demand for vaccination.
“People now know someone who has gotten COVID, who has been hospitalized or has unfortunately died,” Limaye said.
“We’re all seeing this now,” said Kempe. “Even deniers are beginning to see what this illness can do.”
Trump administration officials deny there will be availability issues, but others say problems are possible in the second quarter.
Pfizer has told the Trump administration it cannot provide substantial additional doses of its coronavirus vaccine until late June or July because other countries have rushed to buy up most of its supply, according to multiple individuals familiar with the situation.
That means the U.S. government may not be able to ramp up as rapidly as it had expected from the 100 million doses of the Pfizer vaccine that it purchased earlier this year, raising questions about whether it can keep to its aggressive schedule to vaccinate most Americans by late spring or early summer.
Trump administration officials denied there would be availability issues in the second quarter, citing other vaccines in the pipeline — most immediately, Moderna’s, also expected to be approved in coming weeks. Both vaccines are two-dose regimens, so the 100 million doses purchased of each would cover 50 million people each.
“I’m not concerned about our ability to buy vaccines to offer to all of the American public,” Gen. Paul Ostrowski, who oversees logistics for Operation Warp Speed, the government’s initiative to expedite vaccine development, said in an interview Monday. “It’s clear that Pfizer made plans with other countries. Many have been announced. We understand those pieces.”
But several officials knowledgeable about the contracts said that supplies from other companies may be insufficient to fill the gap.
Last summer, Pfizer officials had urged Operation Warp Speed to purchase 200 million doses, or enough of the two-shot regimen for 100 million people, according to people knowledgeable about the issue who spoke on the condition of anonymity because they weren’t authorized to discuss the situation. But the Warp Speed officials declined, opting instead for 100 million doses, they said. The New York Times first reported that federal officials passed on the opportunity when Pfizer offered to sell more doses.
“Anyone who wanted to sell us … without an [FDA] approval, hundreds of millions of doses back in July and August, was just not going to get the government’s money,” said a senior administration official.
It was only last weekend, with a Food and Drug Administration clearance expected any day, that federal officials reached back out to the company asking to buy another 100 million doses. By then, Pfizer said it had committed the supply elsewhere and suggested elevating the conversation to “a high level discussion,” said a person familiar with the talks.
Pfizer said the company might be able to provide 50 million doses at the end of the second quarter, and another 50 million doses in the third quarter, the individuals said.
The government had a different type of contract with Pfizer than with other companies involved with Operation Warp Speed. Pfizer was the only company that did not take government money for research and development, which meant U.S. officials have had less insight into its decisions than it does with the other companies, said a senior administration official familiar with the matter who spoke on the condition of anonymity.
The contract between the government and Pfizer stipulated that if Pfizer’s vaccine was successful and received authorization from the FDA, the U.S. government would purchase 100 million doses at a set price.
Pfizer spokeswoman Amy Rose declined to confirm any information about the company’s discussions with the government, and said that beyond the first 100 million doses the U.S. has already secured, a separate agreement would have to be negotiated.
President Trump is expected to sign an executive order Tuesday that would prioritize vaccinating Americans before providing doses to other countries, according to a senior administration official who requested anonymity because he was not authorized to speak about the plans. Fox News first reported the executive order. It is not clear whether the order is related to the Pfizer supply issue, or whether the president can prevent an American company from fulfilling lawful contracts with other countries.
“The executive order reaffirms to the American people that we are going to put America first,” said a senior administration official, who spoke on the condition of anonymity because he was not authorized to discuss the issue publicly.
The order will be announced as part of a White House “vaccine summit” designed to highlight the administration’s accomplishments on vaccines.
The vaccine by Pfizer and German biotech firm BioNTech is expected to receive emergency authorization from the FDA in the next several days, and Moderna is lined up for likely clearance shortly after that. Shipments of the vaccines will begin within 24 hours of the approvals, federal officials have said.
Warp Speed officials hope that other companies with promising vaccine candidates will supplement the supply in the near future, but some are still conducting late-stage clinical trials, while others haven’t begun them.
That means it could be several weeks to months before they are ready to apply to the FDA for clearance. One of the companies, AztraZeneca recently reported encouraging vaccine data, but experts raised questions about it and what it meant about the efficacy of the vaccine.
Moncef Slaoui, chief science adviser to Warp Speed, said in an interview Monday that the U.S. government strategy was to spread its risk widely over many different types of vaccines from different manufacturers. He declined to comment on negotiations with any company, but said he did not believe there would be any kind of vaccine “cliff,” where the available doses would fall off sharply.
Slaoui said that Johnson & Johnson was likely to report trial results in early January and be ready to ship doses in February, if its vaccine is authorized. He predicted that AstraZeneca’s trial would report results in late January or early February and potentially begin providing doses later that month.
“We could have all of them,” Slaoui said. “And for this reason, we feel confident we could cover the needs without a specific cliff … We have planned things in such a way as we would indeed avoid a cliff.”
The contract that Pfizer signed with the government in July was to deliver 100 million vaccine doses, and contained an option to contract to buy an additional 500 million doses.
“Pfizer shall inform the Government of appropriate lead times based on purchase of raw materials, capacity reservation and other factors, and Pfizer and the Government shall mutually agree on an appropriate estimated delivery schedule,” the contract states.
“Recognizing the urgency of the need, our manufacturing teams have been working around-the-clock so we can bring the vaccine to the world as quickly, efficiently and equitably as possible,” Rose said.
Additional doses would be “subject to a separate and mutually acceptable agreement” she said.
No agreements with Moderna beyond its initial contract for 100 million have been announced, but the U.S. has the option to purchase 400 million additional doses. Moderna is expected to deliver 20 million doses by year’s end and another tranche in the first quarter of 2021.