The first confirmed coronavirus case in the U.S. was reported on Jan. 19 in a Washington man after returning from Wuhan, China, where the first outbreak of COVID-19 occurred.
Now, data from a new government study paints a different picture — the coronavirus may have been silently spreading in America as early as December 2019.
Researchers with the Centers for Disease Control and Prevention collected 7,389 blood samples from routine donations to the American Red Cross between Dec. 13, 2019 and Jan. 17, 2020.
Of the samples, 106 contained coronavirus antibodies, suggesting those individuals’ immune systems battled COVID-19 at some point.
A total of 39 donations carrying coronavirus antibodies came from residents in the western states of California, Oregon and Washington and 67 samples from the more eastern states of Connecticut, Iowa, Massachusetts, Michigan, Rhode Island and Wisconsin.
The study, published Monday in the journal Clinical Infectious Diseases, adds to growing evidence that the coronavirus had been spreading right under our noses long before testing could confirm it.
“The presence of these serum antibodies indicate that isolated SARS-CoV-2 infections may have occurred in the western portion of the United States earlier than previously recognized or that a small portion of the population may have pre-existing antibodies that bind SARS-CoV-2,” the study reads.
However, the researchers say “widespread community transmission was not likely until late February.”
Some of these early infections may have gone unnoticed because patients with mild or asymptomatic cases may not have sought medical care at the time, the researchers explain in the study. Sick patients with symptoms who did visit a doctor may not have had a respiratory sample collected, so appropriate testing may not have been conducted.
But the researchers wonder if the detection of antibodies in these patient samples really does indicate a past coronavirus infection, and not of another pathogen in the coronavirus family, such as the common cold.
Scientists behind the finding say this “memory” of viruses past could explain why some people are only slightly affected by COVID-19, while others get severely sick.
The researchers call this phenomenon “cross reactivity,” but they note it’s just one of several limitations to their study. The team also said they can’t tell if the COVID-19 cases were community- or travel-associated and that none of the antibody results can be considered “true positives.”
“A true positive would only be collected from an individual with a positive molecular diagnostic test,” the researchers wrote in the study.
Back in May, doctors in Paris also learned the coronavirus had been silently creeping around Europe a month before the official first-known cases were diagnosed in the region.
The first two cases — with known travel to China — in France were reported Jan. 24, but after testing frozen samples from earlier patient records, doctors realized a man with no recent travel had the coronavirus in December.
In mid-November, as the United States set records for newly diagnosed COVID-19 cases day after day, the hospital situation in one hard-hit state, Wisconsin, looked concerning but not yet urgent by one crucial measure. The main pandemic data tracking system run by the Department of Health and Human Services (HHS), dubbed HHS Protect, reported that on 16 November, 71% of the state’s hospital beds were filled. Wisconsin officials who rely on the data to support and advise their increasingly strained hospitals might have concluded they had some margin left.
Yet a different federal COVID-19 data system painted a much more dire picture for the same day, reporting 91% of Wisconsin’s hospital beds were filled. That day was no outlier. A Science examination of HHS Protect and confidential federal documents found the HHS data for three important values in Wisconsin hospitals—beds filled, intensive care unit (ICU) beds filled, and inpatients with COVID-19—often diverge dramatically from those collected by the other federal source, from state-supplied data, and from the apparent reality on the ground.
“Our hospitals are struggling,” says Jeffrey Pothof, a physician and chief quality officer for the health system of the University of Wisconsin (UW), Madison. During recent weeks, patients filled the system’s COVID-19 ward and ICU. The university’s main hospital converted other ICUs to treat the pandemic disease and may soon have to turn away patients referred to the hospital for specialized care. Inpatient beds—including those in ICUs—are nearly full across the state. “That’s the reality staring us down,” Pothof says, adding: The HHS Protect numbers “are not real.”
HHS Protect’s problems are a national issue, an internal analysis completed this month by the Centers for Disease Control and Prevention (CDC) shows. That analysis, other federal reports, and emails obtained by Science suggest HHS Protect’s data do not correspond with alternative hospital data sources in many states (see tables, below). “The HHS Protect data are poor quality, inconsistent with state reports, and the analysis is slipshod,” says one CDC source who had read the agency’s analysis and requested anonymity because of fear of retaliation from the Trump administration. “And the pressure on hospitals [from COVID-19] is through the roof.”
Both federal and state officials use HHS Protect’s data to assess the burden of disease across the country and allocate scarce resources, from limited stocks of COVID-19 medicines to personal protective equipment (PPE). Untrustworthy numbers could lead to supply and support problems in the months ahead, as U.S. cases continue to rise during an expected winter surge, according to current and former CDC officials. HHS Protect leaders vigorously defend the system and blame some disparities on inconsistent state and federal definitions of COVID-19 hospitalization. “We have made drastic improvements in the consistency of our data … even from September to now,” says one senior HHS official. (Three officials from the department spoke with Science on the condition that they not be named.)
CDC had a long-running, if imperfect, hospital data tracking system in place when the pandemic started, but the Trump administration and White House Coronavirus Task Force Coordinator Deborah Birx angered many in the agency when they shifted much of the responsibility for COVID-19 hospital data in July to private contractors.TeleTracking Technologies Inc., a small Pittsburgh-based company, now collects most of the data, while Palantir, based in Denver, helps manage the database. At the time, hundreds of public health organizations and experts warned the change could gravely disrupt the government’s ability to understand the pandemic and mount a response.
The feared data chaos now seems a reality, evident when recent HHS Protect figures are compared with public information from states or data documented by another hospital tracking system run by the HHS Office of the Assistant Secretary for Preparedness and Response (ASPR). ASPR manages the Strategic National Stockpile of medicines, PPE—in perilously short supply in many areas—and other pandemic necessities. ASPR collects data nationwide, although it is more limited than what HHS Protect compiles, to help states and hospitals respond to the pandemic.
In Alabama, HHS Protect figures differ by 15% to 30% from daily state COVID-19 inpatient totals. Karen Landers, assistant state health officer, said nearly all of the state’s hospitals report data to HHS via the Alabama Department of Public Health. Although reporting delays sometimes prevent the systems from syncing precisely, Landers says, she cannot account for the sharp differences.
Many state health officials contacted by Science were reluctant to directly criticize HHS Protect or attribute supply or support problems to its data. Landers notes that Alabama relies on its own collected data, rather than HHS Protect’s, for its COVID-19 response. “We are very confident in our data,” she says, because the state reporting system was developed over several years and required little adjustment to add COVID-19. HHS, she adds, has generally been responsive to state requests for medicines and supplies, although Alabama has not always gotten all the PPE it has requested.
Other states, however, say they do rely on HHS Protect. A spokesperson for the Wisconsin Department of Health Services wrote in a response to questions, “When making decisions at the state level we use the HHS Protect data,” but declined to comment about its accuracy. HHS informed Wisconsin officials it distributes scarce supplies based on need indicated by HHS Protect data, the spokesperson wrote.
Pothof says UW’s hospital system has its own sophisticated data dashboard that draws on state, local, and internal sources to plan and cooperate on pandemic response with other hospitals. But small hospitals in Wisconsin—now experiencing shortages of some medicines, PPE, and other supplies—are more dependent on federal support largely based on HHS Protect data. Help might not arrive, Pothof says, if the data show “things look better than they are.”
If the HHS Protect data are suspect, “that’s a very large problem,” says Nancy Cox, former director of CDC’s influenza division and now an affiliated retiree of the agency. If HHS officials use bad data, they will not distribute medicines and supplies equitably, Cox notes, adding: “Undercounting in the hardest hit states means a lower level of care and will result in more severe infections and ultimately in more deaths.”
Birx and the other managers of HHS Protect “really had no idea what they were doing,” says Tom Frieden, CDC director under former President Barack Obama. (Birx declined to comment for this article.) Frieden cautions that ASPR data might also be erroneous—pointing to the need for an authoritative and clear federal source of hospital data. The original CDC system, called the National Healthcare Safety Network (NHSN), should be improved, he said, but it handles nursing home COVID-19 data skillfully and could do the same with hospitals. NHSN is “not just a computer program. It’s a public health program” built over 15 years and based on relationships with individual health facilities, Frieden says. (CDC insiders say HHS officials recently interfered with publication of an analysis showing that NHSN performed well early in the pandemic [see sidebar, below]).
An HHS official says HHS Protect’s data are complex and the department can’t verify any findings in the reports reviewed by Science without conducting its own analysis, which it did not do. But the official says HHS Protect has improved dramatically in the past 2 months and provides consistent and reliable results.
As for the difference between state and HHS Protect data, an HHS official contends state numbers “are always going to be lower” by up to 20%. That’s because hospitals could lose Medicare funding if they do not report to HHS, the official says, but face no penalty for failing to report to the state. So rather than expect identical numbers, HHS looks for state and federal data to reflect the same trajectory—which they do in all cases for COVID-19 inpatient data, according to another confidential CDC analysis of HHS Protect, covering all 50 states.
Yet the same analysis found 27 states recently alternated between showing more or fewer COVID-19 inpatients than HHS Protect—not always just fewer, as HHS says should be the case. Thirty states also showed differences between state and HHS Protect figures that were frequently well above the 20% threshold cited by HHS, and HHS Protect data fluctuated erratically in 21 states (see chart, below).
“Hospital capacity metrics can and should be a national bellwether,” the CDC data expert says. “One important question raised by the discordant data reported by HHS Protect and the states is whether HHS Protect is systematically checking data validity.” HHS has not provided its methodology for HHS Protect data estimates for review by independent experts. But an HHS official says a team of data troubleshooters, including CDC and ASPR field staff, work to resolve anomalies and respond to spikes in cases in a state or hospital.
Out of sync
Tracking hospital inpatients who have COVID-19 has become a crucial measure of the pandemic’s severity. Department of Health and Human Services (HHS) data from the HHS Protect system often diverge sharply from state-supplied data. This chart, drawn from a data analysis from the Centers for Disease Control and Prevention, summarizes some of the similarities and differences for COVID-19 inpatient totals over the past 2 months.
Along with improving trust in its data, HHS Protect needs to make it more accessible, CDC data scientists say. The publicly accessible HHS Protect data are far less complete than the figures in its password-protected database. This effectively hides from public view key pandemic information, such as local supplies of protective equipment.
The site also does not provide graphics highlighting patterns and trends. This might explain, in part, why most media organizations—as well as President-elect Joe Biden’s transition team—instead have relied on state or county websites that vary widely in completeness and quality, or on aggregations such as The Atlantic magazine’s COVID Tracking Project, which collects, organizes, and standardizes state data. (In comparing state and federal data, CDC also used the COVID Tracking Project.)
Frieden and other public health specialists call reliable, clear federal data essential for an effective pandemic response. “The big picture is that we’re coming up to 100,000 hospitalizations within the next few weeks. Hospital systems all over the country are going to be stressed,” Frieden says. “There’s not going to be any cavalry coming over the hill from somewhere else in the country, because most of the country is going to be overwhelmed. We’re heading into a very hard time with not very accurate information systems. And the government basically undermined the existing system.”
Since the beginning of the coronavirus pandemic, Florida has blocked, obscured, delayed, and at times hidden the COVID-19 data used in making big decisions such as reopening schools and businesses.
And with scientists warning Thanksgiving gatherings could cause an explosion of infections, the shortcomings in the state’s viral reporting have yet to be fixed.
While the state has put out an enormous amount of information, some of its actions have raised concerns among researchers that state officials are being less than transparent.
It started even before the pandemic became a daily concern for millions of residents. Nearly 175 patients tested positive for the disease in January and February, evidence the Florida Department of Health collected but never acknowledged or explained. The state fired its nationally praised chief data manager, she says in a whistleblower lawsuit, after she refused to manipulate data to support premature reopening. The state said she was fired for not following orders.
The health department used to publish coronavirus statistics twice a day before changing to once a day, consistently meeting an 11 a.m. daily deadline for releasing new information that scientists, the media and the public could use to follow the pandemic’s latest twists.
But in the past month the department has routinely and inexplicably failed to meet its own deadline by as much as six hours. On one day in October, it published no update at all.
News outlets were forced to sue the state before it would publish information identifying the number of infections and deaths at individual nursing homes.
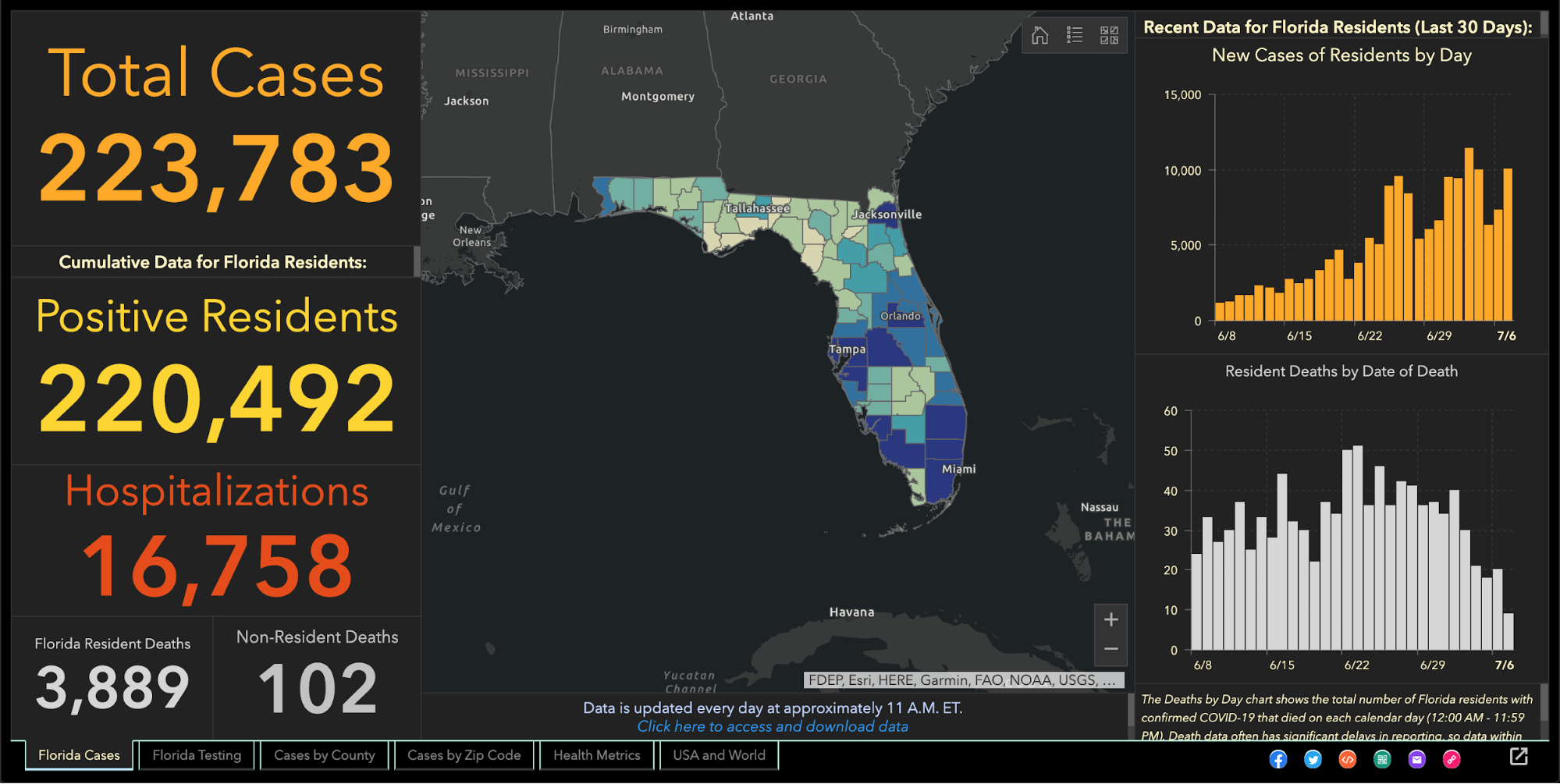
Throughout it all, the state has kept up with the rapidly spreading virus by publishing daily updates of the numbers of cases, deaths and hospitalizations.
“Florida makes a lot of data available that is a lot of use in tracking the pandemic,” University of South Florida epidemiologist Jason Salemi said. “They’re one of the only states, if not the only state, that releases daily case line data (showing age, sex and county for each infected person).”
Dr. Terry Adirim, chairwoman of Florida Atlantic University’s Department of Integrated Biomedical Science, agreed, to a point.
“The good side is they do have daily spreadsheets,” Adirim said. “However, it’s the data that they want to put out.”
The state leaves out crucial information that could help the public better understand who the virus is hurting and where it is spreading, Adirim said.
The department, under state Surgeon General Dr. Scott Rivkees, oversees 53? health agencies covering Florida’s 67 counties, such as the one in Palm Beach County headed by Dr. Alina Alonso.
Rivkees was appointed in April 2019. He reports to Gov. Ron DeSantis, a Republican who has supported President Donald Trump’s approach to fighting the coronavirus and pressured local officials to reopen schools and businesses despite a series of spikes indicating rapid spread of the disease.
At several points, the DeSantis administration muzzled local health directors, such as when it told them not to advise school boards on reopening campuses.
DOH Knew Virus Here Since January
The health department’s own coronavirus reports indicated that the pathogen had been infecting Floridians since January, yet health officials never informed the public about it and they did not publicly acknowledge it even after The Palm Beach Post first reported it in May.
In fact, the night before The Post broke the story, the department inexplicably removed from public view the state’s dataset that provided the evidence. Mixed among listings of thousands of cases was evidence that up to 171 people ages 4 to 91 had tested positive for COVID-19 in the months before officials announced in March the disease’s presence in the state.
Were the media reports on the meaning of those 171 cases in error? The state has never said.
No Testing Stats Initially
When positive tests were finally acknowledged in March, all tests had to be confirmed by federal health officials. But Florida health officials refused to even acknowledge how many people in each county had been tested.
State health officials and DeSantis claimed they had to withhold the information to protect patient privacy, but they provided no evidence that stating the number of people tested would reveal personal information.
At the same time, the director of the Hillsborough County branch of the state health department publicly revealed that information to Hillsborough County commissioners.
And during March the state published on a website that wasn’t promoted to the public the ages and genders of those who had been confirmed to be carrying the disease, along with the counties where they claimed residence.
Firing Coronavirus Data Chief
In May, with the media asking about data that revealed the earlier onset of the disease, internal emails show that a department manager ordered the state’s coronavirus data chief to yank the information off the web, even though it had been online for months.
A health department tech supervisor told data manager Rebekah Jones on May 5 to take down the dataset. Jones replied in an email that was the “wrong call,” but complied, only to be ordered an hour later to put it back.
That day, she emailed reporters and researchers following a listserv she created, saying she had been removed from handling coronavirus data because she refused to manipulate datasets to justify DeSantis’ push to begin reopening businesses and public places.
Two weeks later, the health department fired Jones, who in March had created and maintained Florida’s one-stop coronavirus dashboard, which had been viewed by millions of people, and had been praised nationally, including by White House Coronavirus Task Force Coordinator Deborah Birx.
The dashboard allows viewers to explore the total number of coronavirus cases, deaths, tests and other information statewide and by county and across age groups and genders.
DeSantis claimed on May 21 that Jones wanted to upload bad coronavirus data to the state’s website. To further attempt to discredit her, he brought up stalking charges made against her by an ex-lover, stemming from a blog post she wrote, that led to two misdemeanor charges.
Using her technical know-how, Jones launched a competing COVID-19 dashboard website, FloridaCOVIDAction.com in early June. After national media covered Jones’ firing and website launch, people donated more than $200,000 to her through GoFundMe to help pay her bills and maintain the website.
People view her site more than 1 million times a day, she said. The website features the same type of data the state’s dashboard displays, but also includes information not present on the state’s site such as a listing of testing sites and their contact information.
Jones also helped launch TheCOVIDMonitor.com to collect reports of infections in schools across the country.
Jones filed a whistleblower complaint against the state in July, accusing managers of retaliating against her for refusing to change the data to make the coronavirus situation look better.
“The Florida Department of Health needs a data auditor not affiliated with the governor’s office because they cannot be trusted,” Jones said Friday.
Florida Hides Death Details
When coronavirus kills someone, their county’s medical examiner’s office logs their name, age, ethnicity and other information, and sends it to the Florida Department of Law Enforcement.
During March and April, the department refused requests to release that information to the public, even though medical examiners in Florida always have made it public under state law. Many county medical examiners, acknowledging the role that public information can play in combating a pandemic, released the information without dispute.
But it took legal pressure from news outlets, including The Post, before FDLE agreed to release the records it collected from local medical examiners.
When FDLE finally published the document on May 6, it blacked out or excluded crucial information such as each victim’s name or cause of death.
But FDLE’s attempt to obscure some of that information failed when, upon closer examination, the seemingly redacted details could in fact be read by common computer software.
Outlets such as Gannett, which owns The Post, and The New York Times, extracted the data invisible to the naked eye and reported in detail what the state redacted, such as the details on how each patient died.
Reluctantly Revealing Elder Care Deaths, Hospitalizations
It took a lawsuit against the state filed by the Miami Herald, joined by The Post and other news outlets, before the health department began publishing the names of long-term care facilities with the numbers of coronavirus cases and deaths.
The publication provided the only official source for family members to find out how many people had died of COVID-19 at the long-term care facility housing their loved ones.
While the state agreed to publish the information weekly, it has failed to publish several times and as of Nov. 24 had not updated the information since Nov. 6.
It took more pressure from Florida news outlets to pry from the state government the number of beds in each hospital being occupied by coronavirus patients, a key indicator of the disease’s spread, DeSantis said.
That was one issue where USF’s Salemi publicly criticized Florida.
“They were one of the last three states to release that information,” he said. “That to me is a problem because it is a key indicator.”
Confusion Over Positivity Rate
One metric DeSantis touted to justify his decision in May to begin reopening Florida’s economy was the so-called positivity rate, which is the share of tests reported each day with positive results.
But Florida’s daily figures contrasted sharply with calculations made by Johns Hopkins University, prompting a South Florida Sun-Sentinel examination that showed Florida’s methodology underestimated the positivity rate.
The state counts people who have tested positive only once, but counts every negative test a person receives until they test positive, so that there are many more negative tests for every positive one.
John Hopkins University, on the other hand, calculated Florida’s positivity rate by comparing the number of people testing positive with the total number of people who got tested for the first time.
By John Hopkins’ measure, between 10 and 11 percent of Florida’s tests in October came up positive, compared to the state’s reported rate of between 4 and 5 percent.
Health experts such as those at the World Health Organization have said a state’s positivity rate should stay below 5 percent for 14 days straight before it considers the virus under control and go forward with reopening public places and businesses. It’s also an important measure for travelers, who may be required to quarantine if they enter a state with a high positivity rate.
Withholding Detail on Race, Ethnicity
The Post reported in June that the share of tests taken by Black and Hispanic people and in majority minority ZIP codes were twice as likely to come back positive compared to tests conducted on white people and in majority white ZIP codes.
That was based on a Post analysis of internal state data the health department will not share with the public.
The state publishes bar charts showing general racial breakdowns but not for each infected person.
If it wanted to, Florida’s health department could publish detailed data that would shed light on the infection rates among each race and ethnicity or each age group, as well as which neighborhoods are seeing high rates of contagion.
Researchers have been trying to obtain this data but “the state won’t release the data without (making us) undergo an arduous data use agreement application process with no guarantee of release of the data,” Adirim said. Researchers must read and sign a 26-page, nearly 5,700-word agreement before getting a chance at seeing the raw data.
While Florida publishes the ages, genders and counties of residence for each infected person, “there’s no identification for race or ethnicity, no ZIP code or city of the residence of the patient,” Adirim said. “No line item count of negative test data so it’s hard to do your own calculation of test positivity.”
While Florida doesn’t explain its reasoning, one fear of releasing such information is the risk of identifying patients, particularly in tiny, non-diverse counties.
Confusion Over Lab Results
Florida’s daily report shows how many positive results come from each laboratory statewide. Except when it doesn’t.
The report has shown for months that 100 percent of COVID-19 tests conducted by some labs have come back positive despite those labs saying that shouldn’t be the case.
While the department reported in July that all 410 results from a Lee County lab were positive, a lab spokesman told The Post the lab had conducted roughly 30,000 tests. Other labs expressed the same confusion when informed of the state’s reporting.
The state health department said it would work with labs to fix the error. But even as recently as Tuesday, the state’s daily report showed positive result rates of 100 percent or just under it from some labs, comprising hundreds of tests.
Mistakenly Revealing School Infections
As DeSantis pushed in August for reopening schools and universities for students to attend in-person classes, Florida’s health department published a report showing hundreds of infections could be traced back to schools, before pulling that report from public view.
The health department claimed it published that data by mistake, the Miami Herald reported.
The report showed that COVID-19 had infected nearly 900 students and staffers.
The state resumed school infection reporting in September.
A similar publication of cases at day-care centers appeared online briefly in August only to come down permanently.
Updates Delayed
After shifting in late April to updating the public just once a day at 11 a.m. instead of twice daily, the state met that deadline on most days until it started to falter in October. Pandemic followers could rely on the predictability.
On Oct. 10, the state published no data at all, not informing the public of a problem until 5 p.m.
The state blamed a private lab for the failure but the next day retracted its statement after the private lab disputed the state’s explanation. No further explanation has been offered.
On Oct. 21, the report came out six hours late.
Since Nov. 3, the 11 a.m. deadline has never been met. Now, late afternoon releases have become the norm.
“They have gotten more sloppy and they have really dragged their feet,” Adirim, the FAU scientist, said.
No spokesperson for the health department has answered questions from The Post to explain the lengthy delays. Alberto Moscoso, the spokesman throughout the pandemic, departed without explanation Nov. 6.
The state’s tardiness can trip up researchers trying to track the pandemic in Florida, Adirim said, because if one misses a late-day update, the department could overwrite it with another update the next morning, eliminating critical information and damaging scientists’ analysis.
Hired Sports Blogger to Analyze Data
As if to show disregard for concerns raised by scientists, the DeSantis administration brought in a new data analyst who bragged online that he is no expert and doesn’t need to be.
Kyle Lamb, an Uber driver and sports blogger, sees his lack of experience as a plus.
“Fact is, I’m not an ‘expert’,” Lamb wrote on a website for a subscribers-only podcast he hosts about the coronavirus. “I also don’t need to be. Experts don’t have all the answers, and we’ve learned that the hard way throughout the entire duration of the global pandemic.”
Much of his coronavirus writings can be found on Twitter, where he has said masks and mandatory quarantines don’t stop the virus’ spread, and that hydroxychloroquine, a drug touted by President Donald Trump but rejected by medical researchers, treats it successfully.
While DeSantis says lockdowns aren’t effective in stopping the spread and refuses to enact a statewide mask mandate, scientists point out that quarantines and masks are extremely effective.
The U.S. Food and Drug Administration has said hydroxychloroquine is unlikely to help and poses greater risk to patients than any potential benefits.
Coronavirus researchers have called Lamb’s views “laughable,” and fellow sports bloggers have said he tends to act like he knows much about a subject in which he knows little, the Miami Herald reported.
DeSantis has yet to explain how and why Lamb was hired, nor has his office released Lamb’s application for the $40,000-a-year job. “We generally do not comment on such entry level hirings,” DeSantis spokesman Fred Piccolo said Tuesday by email.
It could be worse.
Texas health department workers have to manually enter data they read from paper faxes into the state’s coronavirus tracking system, The Texas Tribune has reported. And unlike Florida, Texas doesn’t require local health officials to report viral data to the state in a uniform way that would make it easier and faster to process and report.
It could be better.
In Wisconsin, health officials report the number of cases and deaths down to the neighborhood level. They also plainly report racial and ethnic disparities, which show the disease hits Hispanic residents hardest.
Still, Salemi worries that Florida’s lack of answers can undermine residents’ faith.
“My whole thing is the communication, the transparency,” Salemi said. “Just let us know what’s going on. That can stop people from assuming the worst. Even if you make a big error people are a lot more forgiving, whereas if the only time you’re communicating is when bad things happen … people start to wonder.”
Dressed in blue scrubs and carrying a stethoscope around her neck, an oncology nurse in Salem, Ore., looked to the Grinch as inspiration while suggesting that she ignored coronavirus guidelines outside of work.
In a TikTok video posted Friday, she lip-dubbed a scene from “How the Grinch Stole Christmas” to get her point across to her unaware colleagues: She does not wear a mask in public when she’s not working at Salem Hospital.
“When my co-workers find out I still travel, don’t wear a mask when I’m out and let my kids have play dates,” the nurse wrote in a caption accompanying the video, which has since been deleted.
Following swift online backlash from critics, her employer, Salem Health, announced Saturday that the nurse had been placed on administrative leave. In a statement, the hospital said the nurse, who has not been publicly identified by her employer, “displayed cavalier disregard for the seriousness of this pandemic and her indifference towards physical distancing and masking out of work.”
“We also want to assure you that this one careless statement does not reflect the position of Salem Health or the hardworking and dedicated caregivers who work here,” said the hospital, adding that an investigation is underway.
Salem Health did not respond to The Washington Post’s request for comment as of early Monday.
The nurse’s video offers a startling and rare glimpse of a front-line health-care worker blatantly playing down a virus that has killed at least 266,000 Americans. It also has been seen in some coronavirus patients, some on their deathbeds, who still refuse to believe the pandemic is real.
The incident comes at a time when Oregon has continued to see a spike in new coronavirus cases and virus-related hospitalizations. Just last week, the state’s daily reported deaths and hospitalizations rose by 33.3 and 24.2 percent respectively, according to The Post’s coronavirus tracker. At least 74,120 Oregonians have been infected with the virus since late February; 905 of them have died.
The clip posted to TikTok on Friday shows the nurse mocking the health guidelines while using audio from a scene in which the Grinch reveals his true identity to Cindy Lou Who.
Although the original video was removed, TikTok users have shared a “duet” video posted by another user critical of the nurse, which had more than 274,000 reactions as of early Monday.
Soon after she posted the clip, hundreds took to social media and the hospital’s Facebook page to report the nurse’s video and demand an official response from her employer. Some requested that the nurse be removed from her position and that her license be revoked.
Hospital officials told the Salem Statesman Journal that the investigation is aiming to figure out which other staff members and patients have come in contact with the nurse, who works in the oncology department.
But for some, the hospital’s apologies and actions were not enough.
“The video supplied should be evidence enough,” one Facebook user commented. “She needs to be FIRED. Not on PAID leave. As someone fighting cancer, I can only imagine how her patients feel after seeing this news.”
The hospital thanked those who alerted them of the incident, emphasizing that its staff, patients and visitors must adhere to the Centers for Disease Control and Prevention guidelines.
“These policies are strictly enforced among staff from the moment they leave their cars at work to the moment they start driving home,” hospital officials told the Statesman Journal.
At a rural health system in Wisconsin, officials and medical experts began drawing up protocols for the once unthinkable practice of deciding which patients should get care. The chief quality officer of a major New York hospital network double- and triple-checked his system’s stockpile of emergency equipment, grimly recalling the last time he had to count how many ventilators he had left. In Arizona, a battle-weary doctor watched in horror as people flooded airports and flocked to stores for Black Friday sales, knowing it was only a matter of time before some of them wound up in his emergency room.
Days after millions of Americans ignored health guidance to avoid travel and large Thanksgiving gatherings, it’s still too soon to tell how many people became infected with the coronavirus over the course of the holiday weekend. But as travelers head home to communities already hit hard by the disease, hospitals and health officials across the country are bracing for what scientist Dave O’Connor called “a surge on top of a surge.”
“It is painful to watch,” said O’Connor, a virologist at the University of Wisconsin at Madison. “Like seeing two trains in the distance and knowing they’re about to crash, but you can’t do anything to stop it.”
“Because of the decisions and rationalizations people made to celebrate,” the scientist added, “we’re in for a very dark December.”
The holiday, which is typically one of the busiest travel periods of the year, fell at a particularly dire time in the pandemic. Some 4 million Americans have been diagnosed with the coronavirus in November — twice the previous record, which was set last month. More than 2,000 people are dying every day. Despite that, over a million people passed through U.S. airports the day before Thanksgiving — the highest number of travelers seen since the start of the outbreak.
Many states did not report new case counts over the holiday, and it typically takes about a week for official records to catch up after reporting delays, said Caitlin Rivers, an epidemiologist at the Johns Hopkins Center for Health Security.
But in two to three weeks, she said, “I fully expect on a national level we will see those trends continue of new highs in case counts and hospitalizations and deaths.”
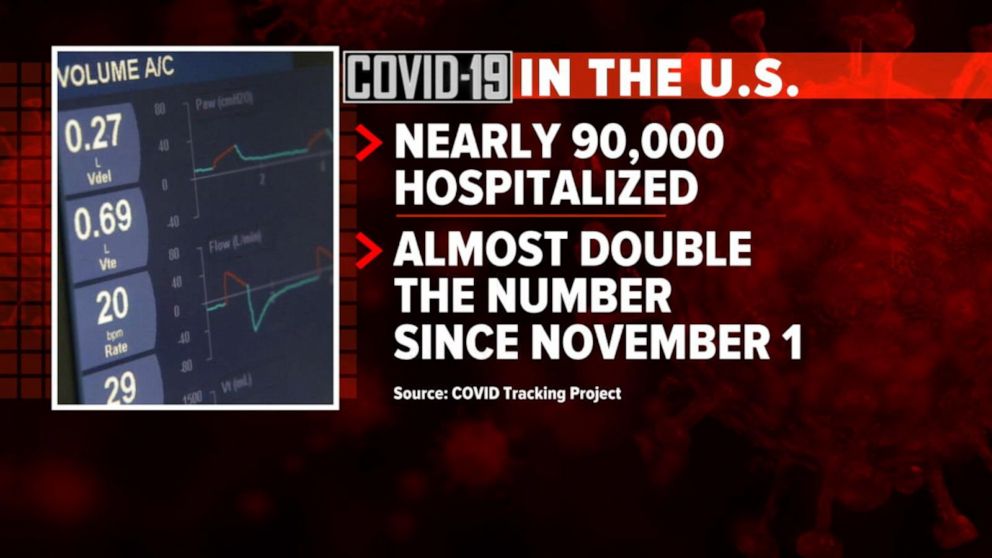
The nation has already notched several bleak milestones over the holiday weekend. On Thanksgiving Day, hospitalizations in the United States exceeded 90,000 people for the first time. The following day, the country hit 13 million cases. At least nine states have seen 1 in every 1,000 residents die of the coronavirus.
Mark Jarret, the chief quality officer for New York’s Northwell Health system, said he understood that many people are tiring of constant vigilance after nine months of isolation and Zoom gatherings and waving at people from six feet away.
“But we’re so close to getting some control,” he said, noting that federal officials are on the verge of authorizing one or more vaccines against the virus next month. “This is not the time to let up. This is the time to put on the best defense we can to prevent further spread, further death.”
Officials urged people who traveled or spent time with people outside their household to stay at home for 14 days to avoid further spread of the virus. Some jurisdictions are moving toward lockdown measures not seen since the spring. Los Angeles County on Friday issued a three-week “safer at home” order, limiting business capacity and prohibiting gatherings other than religious services and protests.
Meanwhile, the December holidays are looming.
“Hopefully people will try to minimize their risks around Christmas, especially if there’s data that show Thanksgiving was really harmful,” O’Connor said.
To Cleavon Gilman, a Navy veteran and emergency room doctor in Yuma, Ariz., the wave of holiday travel was “a slap in the face.”
“It’s as if there’s not a pandemic happening,” he said. “We’re in a war right now, and half the country isn’t on board.”
On Friday, members of the University of Arizona coronavirus modeling team issued an urgent warning to state health officials, projecting that the state will exceed ICU capacity by the beginning of December.
“If action is not immediately taken, then it risks a catastrophe on a scale of the worst natural disaster the state has ever experienced,” the team wrote in a letter to Steven Bailey, chief of the Bureau of Public Health Statistics. “It would be akin to facing a major forest fire without evacuation orders.”
Arizona has no statewide mask mandate, and businesses in many parts of the state, including indoor dining at restaurants, remain open.
Gilman said the intensive care unit at his hospital is full and there’s nowhere to transfer new patients. When he’s home, his mind echoes with the sound of people gasping for breath. He and his colleagues are exhausted, and with cases spiking across the country, he worries there is no way they can handle the surge that will probably follow Thanksgiving celebrations.
In La Crosse, Wis., Gundersen Health System chief executive Scott Rathgaber echoed that fear. “We’ve had to tell our hard-working staff, ‘There’s no one out there to come rescue us,’” he said.
Like many in his college town, Rathgaber is anxious about what will happen when students who spent the holiday with their families return to campus. Though the University of Wisconsin and other schools shifted classes online for the remainder of the semester, he anticipates students who have jobs and apartments in La Crosse will return to town.
“We had trouble the first time the students came back,” Rathgaber said, noting that the start of college classes in September preceded outbreaks in nursing homes and a spike in deaths in La Crosse County. “I will continue to implore, to beg people to take this seriously.”
Gundersen has already more than tripled the size of the covid-19 ward at its main hospital, and even before this week it was almost entirely full. Physicians from the system’s rural clinics have been reassigned to La Crosse to help in the ICU. Staff who may have been exposed to the virus are being called back before completing their 14-day quarantine. And Rathgaber now attends regular meetings with ethicists and end-of-life caregivers to figure out Gundersen’s triage protocol if the hospital becomes overwhelmed.
“We’re not at a breaking point, but we are getting there,” Rathgaber said. “I’m concerned about what the next two weeks will bring.”
Detroit Mayor Mike Duggan (D) on Sunday said mitigation efforts such as mask mandates have been effective in reducing coronavirus rates in the city, calling such efforts an alternative to mass shutdowns.
“Detroit actually has the lowest infection rate in the state of Michigan,” Duggan said on CBS’s “Face the Nation.” “And it’s because behavior changed. In March and April, Michigan was hammered along with New York, and we had within a few weeks, a thousand people hospitalized and 50 of our neighbors dying every day.”
In contrast, he said, the city currently had about 200 patients hospitalized and one or two deaths per day.
“It’s still too high, but the commitment to the testing, the commitment to the masks, has shown that you can dramatically drop the infection rate,” Duggan added.
The mayor noted that the city’s infection rate is about half of those of its surrounding suburbs.
“If you make a commitment to the masks, we don’t have to shut the economy down,” he said.
Asked how the city’s mask mandate and other measures had affected the spread of the virus, Duggan responded that “assembly lines are in our DNA” and pointed to the city’s drive-through testing apparatus.
Duggan went on to say that frontline workers such as firefighters, hospital workers and emergency medical technicians would likely be the first people in the city to receive a coronavirus vaccine, followed by the elderly.
“Occupation is going to go first…then people over the age over 65,” he said. “That’s the way they’re talking about it, I will be really glad when [President-elect] Joe Biden takes control of this and we get clear direction, but we will follow whatever protocols are there.”
The United States recorded 90,481 people currently hospitalized with COVID-19 Nov. 26, marking the 17th consecutive day of record hospitalizations and the first time the daily count topped 90,000, according to The COVID Tracking Project.
The Project has noted that several data points will likely “wobble” over the next several days due to the Thanksgiving holiday, which may cause data points for COVID-19 testing, new cases and deaths to flatten or drop for several days before spiking. It is unlikely that Thanksgiving infections will be clearly visible in official case data until at least the second week of December.
However, the Project’s staff has noted that the new admissions metric in the public hospitalization dataset from HHS shows only moderate volatility and will likely be an additional source of useful data through the expected holiday dip and subsequent spike in test, case and death data.
“If you’re a reporter covering COVID-19, we recommend focusing on current hospitalizations and new admissions as the most reliable indicator of what is actually happening in your area and in the country as a whole,” reads the Nov. 24 blog from The COVID Tracking Project.