https://www.linkedin.com/pulse/15-innovative-ideas-fixing-healthcare-from-brilliant-pearl-m-d-/

After 18 years as CEO in Kaiser Permanente, I set my sights on improving the heatlh of the nation, hoping to find a way to achieve the same quality, technology and affordability our medical group delivered to 5 million patients on both coasts.
That quest launched the Fixing Healthcare podcast in 2018, and it inspired interviews with dozens of leaders, thinkers and doers, both in and around medicine. These experts shared innovative ideas and proven solutions for achieving (a) superior quality, (b) improved patient access, (c) lower overall costs, and (d) greater patient and clinician satisfaction.
This month, after 150 combined episodes, three questions emerged:
- Which of the hundreds of ideas presented remain most promising?
- Why, after five years and so many excellent solutions, has our nation experienced such limited improvements in healthcare?
- And finally, how will these great ideas become reality?
To answer the first question, I offer 15 of the best Fixing Healthcare recommendations so far. Some quotes have been modified for clarity with links to all original episodes (and transcripts) included.
Fixing the business of medicine
1. Malcolm Gladwell, journalist and five-time bestselling author: “In other professions, when people break rules and bring greater economic efficiency or value, we reward them. In medicine, we need to demonstrate a consistent pattern of rewarding the person who does things better.”
2. Richard Pollack, CEO of the American Hospital Association (AHA): “I hope in 10 years we have more integrated delivery systems providing care, not bouncing people around from one unconnected facility to the next. I would hope that we’re in a position where there’s a real focus on ensuring that people get care in a very convenient way.”
Eliminating burnout
3. Zubin Damania, aka ZDoggMD, hospitalist and healthcare satirist: “In the culture of medicine, specialists view primary care as the weak medical students, the people who couldn’t get the board scores or rotation honors to become a specialist. Because why would you do primary care? It’s miserable. You don’t get paid enough. It’s drudgery. We must change these perceptions.”
4. Devi Shetty, India’s leading heart surgeon and founder of Narayana Health: “When you strive to work for a purpose, which is not about profiting yourself, the purpose of our action is to help society, mankind on a large scale. When that happens, cosmic forces ensure that all the required components come in place and your dream becomes a reality.”
5. Jonathan Fisher, cardiologist and clinician advocate: “The problem we’re facing in healthcare is that clinicians are all siloed. We may be siloed in our own institution thinking that we’re doing it best. We may be siloed in our own specialty thinking that we’re better than others. All of these divides need to be bridged. We need to begin the bridging.”
Making medicine equitable
6. Jen Gunter, women’s health advocate and “the internet’s OB-GYN”: “Women are not listened to by doctors in the way that men are. They have a harder time navigating the system because of that. Many times, they’re told their pain isn’t that serious or their bleeding isn’t that heavy. We must do better at teaching women’s health in medicine.”
7. Amanda Calhoun, activist, researcher and anti-racism educator: “A 2015 survey showed that white residents and medical students still thought Black people feel less pain, which is wild to me because Black is a race. It’s not biological. This is actually an historical belief that persists. One of the biggest things we can do as the medical system is work on rebuilding trust with the Black community.”
Addressing social determinants of health
8. Don Berwick, former CMS administrator and head of 100,000 Lives campaign: “We know where the money should go if we really want to be a healthy nation: early childhood development, workplaces that thrive, support to the lonely, to elders, to community infrastructures like food security and transportation security and housing security, to anti-racism and criminal-justice reform. But we starve the infrastructures that could produce health to support the massive architecture of intervention.”
9. David T. Feinberg, chairman of Oracle Health: “Twenty percent of whether we live or die, whether we have life in our years and years in our life, is based on going to good doctors and good hospitals. We should put the majority of effort on the stuff that really impacts your health: your genetic code, your zip code, your social environment, your access to clean food, your access to transportation, how much loneliness you have or don’t have.”
Empowering patients
10. Elisabeth Rosenthal, physician, author and editor-in-chief of KHN: “To patients, I say write about your surprise medical bills. Write to a journalist, write to your local newspaper. Hospitals today are very sensitive about their reputations and they do not want to be shamed by some of these charges.”
11. Gordon Chen, ChenMed CMO: “If you think about what leadership really is, it’s influence. Nothing more, nothing less. And the only way to achieve better health in patients is to get them to change their behaviors in a positive way. That behavior change takes influence. It requires primary care physicians to build relationship and earn trust with patients. That is how both doctors and patients can drive better health outcomes.”
Utilizing technology
12. Vinod Khosla, entrepreneur, investor, technologist: “The most expensive part of the U.S. healthcare system is expertise, and expertise can relatively be tamed with technology and AI. We can capture some of that expertise, so each oncologist can do 10 times more patient care than they would on their own without that help.”
13. Rod Rohrich, influential plastic surgeon and social media proponent: “Doctors, use social media to empower your audience, to educate them, and not to overwhelm them. If you approach social media by educating patients about their own health, how they can be better, how can they do things better, how they can find doctors better, that’s a good thing.”
Rethinking medical education
14. Marty Makary, surgeon and public policy researcher: “I would get rid of all the useless sh*t we teach our medical students and residents and fellows. In the 16 years of education that I went through, I learned stuff that has nothing to do with patient care, stuff that nobody needs to memorize.”
15. Eric Topol, cardiologist, scientist and AI expert: “It’s pretty embarrassing. If you go across 150 medical schools, not one has AI as a core curriculum. Patients will get well versed in AI. It’s important that physicians stay ahead, as well.”
Great ideas, but little progress
Since 2018, our nation has spent $20 trillion on medical care, navigated the largest global pandemic in a century and developed an effective mRNA vaccine, nearly from scratch. And yet, despite all this spending and scientific innovation, American medicine has lost ground.
American life expectancy has dropped while maternal mortality rates have worsened. Clinician burnout has accelerated amid a growing shortage of primary care and emergency medicine physicians. And compared to 12 of its wealthiest global peers, the United States spends nearly twice as much per person on medical care, but ranks last in clinical outcomes.
Guests on Fixing Healthcare generally agree on the causes of stagnating national progress.
Healthcare system giants, including those in the drug, insurance and hospital industries, find it easier to drive up prices than to prevent disease or make care-delivery more efficient. Over the past decade, they’ve formed a conglomerate of monopolies that prosper from the existing rules, leaving them little incentive to innovate on behalf of patients. And in this era of deep partisan divide, meaningful healthcare reforms have not (and won’t) come from Congress.
Then who will lead the way?
Industry change never happens because it should. It happens when demand and opportunity collide, creating space for new entrants and outsiders to push past the established incumbents. In healthcare, I see two possibilities:
1. Providers will rally and reform healthcare
Doctors and hospitals are struggling. They’re struggling with declining morale and decreasing revenue. Clinicians are exiting the profession and hospitals are shuttering their doors. As the pain intensifies, medical group leaders may be the ones who decide to begin the process of change.
The first step would be to demand payment reform.
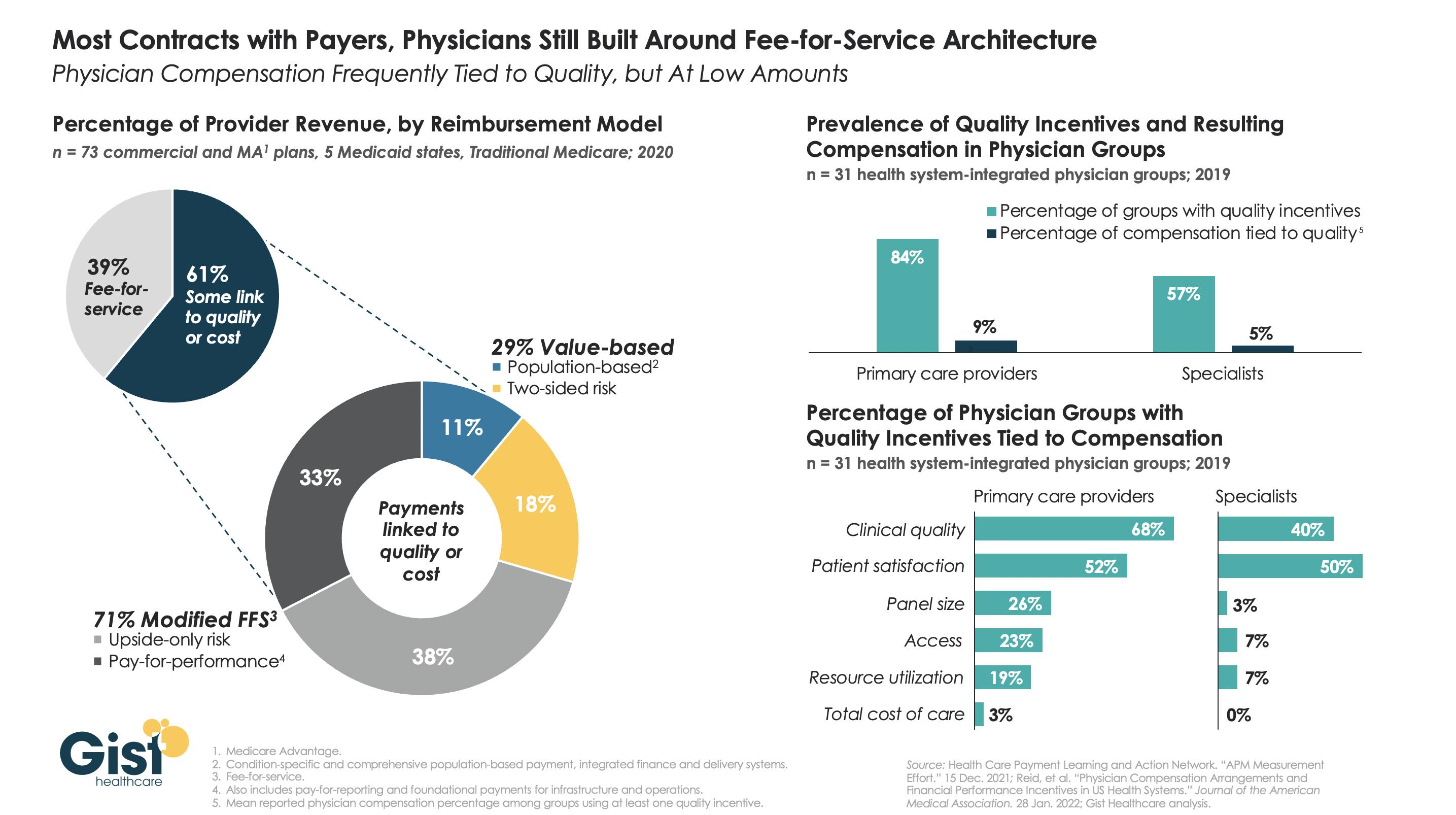
Today’s reimbursement model, fee-for-service, pays doctors and hospitals based on the quantity of care they provide—not the quality of care. This methodology pushes physicians to see more patients, spend less time with them, and perform ever-more administrative (billing) tasks. Physicians liken it to being in a hamster wheel: running faster and faster just to stay in place.
Instead, providers of care could be paid by insurers, the government and self-funded businesses directly, through a model called “capitation.” With capitation, groups of providers receive a fixed amount of money per year. That sum depends on the number of enrollees they care for and the amount of care those individuals are expected to need based on their age and underlying diseases.
This model puts most of the financial risk on providers, encouraging them to deliver high-quality, effective medical care. With capitation, doctors and hospitals have strong financial incentives to prevent illnesses through timely and recommended preventive screenings and a focus on lifestyle-medicine (which includes diet, exercise and stress reduction). They’re rewarded for managing patients’ health and helping them avoid costly complications from chronic diseases, such as heart attacks, strokes and cancer.
Capitation encourages doctors from all specialties to collaborate and work together on behalf of patients, thus reducing the isolation physicians experience while ensuring fewer patients fall through the cracks of our dysfunctional healthcare system. The payment methodology aligns the needs of patients with the interests of providers, which has the power to restore the sense of mission and purpose medicine has lost.
Capitation at the delivery-system level eliminates the need for prior authorization from insurers (a key cause of clinician burnout) and elevates the esteem accorded to primary care doctors (who focus on disease prevention and care coordination). And because the financial benefits are tied to better health outcomes, the capitated model rewards clinicians who eliminate racial and gender disparities in medical care and organizations that take steps to address the social determinants of health.
2. Major retailers will take over
If clinicians don’t lead the way, corporate behemoths like Amazon, CVS and Walmart will disrupt the healthcare system as we know it. These retailers are acquiring the insurance, pharmacy and direct-patient-care pieces needed to squeeze out the incumbents and take over American healthcare.
Each is investing in new ways to empower patients, provide in-home care and radically improve access to both in-person and virtual medicine. Once generative AI solutions like ChatGPT gain enough computing power and users, tech-savvy retailers will apply this tool to monitor patients, enable healthier lifestyles and improve the quality of medical care compared to today.
When Fixing Healthcare debuted five years ago, none of the show’s guests could have foreseen a pandemic that left more than a million dead. But, had our nation embraced their ideas from the outset, many of those lives would have been saved. The pandemic rocked an already unstable and underperforming healthcare system. Our nation’s failure to prevent and control chronic disease resulted in hundreds of thousands of unnecessary deaths from Covid-19. Outdated information technology systems, medical errors and disparities in care caused hundreds of thousands more. As a nation, we could have done much better.
With the cracks in the system widening and the foundation eroding, disruption in healthcare is inevitable. What remains to be seen is whether it will come from inside or outside the U.S. healthcare system.