The Department of Justice (DOJ) is appealing a Florida judge’s Monday decision to strike down the mask requirement for public transportation. Federal judge Kathryn Mizelle ruled the Centers for Disease Control and Prevention (CDC) exceeded its authority under the Public Health Service Act of 1944. Meanwhile, giddy passengers and flight crew have been discarding their face coverings as airlines, the Transportation Safety Administration, several local transit authorities, Uber and Lyft, all removed their mask requirements.
The Gist: Despite DOJ’s appeal, which appears to be aimed at preserving its own authority to act during health crises, rather than reinstating the current mask requirement (which was set to expire in two weeks anyway), the tone of the Biden administration is clearly shifting. Earlier this week President Biden told reporters that the decision to wear a mask is “up to them,” meaning individual Americans.
In the bumpy transition out of the emergency phase of the pandemic, we now have a patchwork of rules for masking. This is even true within healthcare facilities: some, including Houston Methodist and Iowa-based UnityPoint Health, are no longer requiring masks for visitors or employees who are not involved in patient care.
With COVID cases now rising in 41 states as mask mandates fall, the next month will prove critical in determining whether “endemic” COVID remains manageable, or once again stresses the healthcare system and other critical infrastructure.
But officials caution that people should not presume they have protection against the virus going forward.
Before omicron, one-third of Americans had been infected with the coronavirus, but by the end of February, that rate had climbed to nearly 60 percent — including about 75 percent of kids and 60 percent of people age 18 to 49, according to federal health data released Tuesday.
The data from blood tests offers the first evidence that over half the U.S. population, or 189 million people have been infected at least once since the pandemic began — double the number reflected in official case counts. Officials cautioned, however, that the data, in a report from the Centers for Disease Control and Prevention, does not indicate people have protection against the virus going forward, especially against increasingly transmissible variants.
“We continue to recommend that everyone be up to date on their vaccinations, get your primary series and booster, when eligible,” CDC Director Rochelle Walensky said during a media briefing.
Kristie Clarke, the CDC official who authored the report, said by February, “evidence of previous COVID-19 infections substantially increased among every age group, likely reflecting the increase in cases we noted as omicron surged in this country.”
Clarke said the greatest increases took place in those with the lowest levels of vaccination, noting that older adults were more likely to be fully vaccinated.
The largest increases were in children and teenagers through age 17 — about 75 percent of them had been infected by February, based on blood samples that look at antibodies developed in response to a coronavirus infection but not in response to vaccination. That’s about 58 million children.
The blood test data suggests 189 million Americans had covid-19 by end of February, well over double the 80 million cases shown by The Washington Post case tracker, which is based on state data of confirmed infections. Clarke said that’s because the blood tests captures asymptomatic cases and others that were never confirmed on coronavirus tests.
With the omicron surge, officials had expected there would be more infections. “But I didn’t expect the increase to be quite this much,” Clarke added.
Separately, CDC is about to publish another study that estimates three infections for every reported case, she said.
Sacramento-based Sutter Health said nurses who went on strike April 18 will not be allowed to return to work until the morning of April 23, the San Francisco Chronicle reported.
The strike affected nurses and healthcare workers at Sutter Health facilities in Northern California. The nurses are members of the California Nurses Association, and the other workers are members of the Caregivers and Healthcare Employees Union, an affiliate of the California Nurses Association.
More than 8,000 registered nurses and healthcare workers were expected to participate in the strike, according to an April 18 news release from the unions.
In a statement shared with Becker’s, Sutter Health said the organization conducted strike contingency planning, which included “securing staff to replace nurses who have chosen to strike, and those replacement contracts provide the assurance of five days of guaranteed staffing amid the uncertainty of a widespread work stoppage.”
“As always, our top priority remains safe, high-quality patient care and nurses may be reinstated sooner based on operational and patient care needs,” the statement said.
The California Nurses Association described Sutter Health’s decision as retaliatory, as well as “completely unnecessary and vindictive.”
“Nurses who are regularly scheduled to work during this lockout period will lose those days of pay,” the union said in a statement shared with Becker’s. “We urge Sutter to respect the nurses’ strike and let all nurses return to work.”
Sutter Health workers authorized a strike in March, and union officials announced an official strike notice April 8. Union members cited lack of transparency about the stockpile of personal protective equipment supplies and contact tracing as a reason for the strike. They also said they seek a contract that will help retain experienced nurses and provide sufficient staffing and training.
Nurses have been in contract negotiations since June.
Over the next few weeks, the U.S. should expect an increase in cases from the BA.2 variant, Dr. Anthony Fauci told ABC News, but it may not lead to as severe a surge in hospitalizations or deaths.
“I would not be surprised if in the next few weeks we see somewhat of either a flattening of our diminution or maybe even an increase,” Fauci told ABC News’ Brad Mielke on the podcast “Start Here.”
His prediction is based on conversations with colleagues in the U.K., which is currently seeing a “blip” in cases, Fauci said. The pandemic trajectory in the U.S. has often followed the U.K. by about three weeks.
However, he added, “Their intensive care bed usage is not going up, which means they’re not seeing a blip up of severe disease.”
The BA.2 variant, a more transmissible strain of omicron, now represents around 23% of all cases in the U.S., according to the latest data from the Centers for Disease Control and Prevention.
And while Fauci predicted that the BA.2 variant will eventually overtake omicron as the most dominant variant, it’s not yet clear how much of a problem that will be.
“Whether or not that is going to lead to another surge, a mini surge or maybe even a moderate surge, is very unclear because there are a lot of other things that are going on right now,” Fauci said.
Similar to the U.K., much of the U.S. has recently relaxed mitigation efforts like mask mandates and requirements for proof of vaccination. At the same time, people who were vaccinated over six months ago and still haven’t gotten a booster shot, which is about half of vaccinated Americans, according to the CDC, are facing continuously waning immunity.
It’s also not yet clear how long immunity from prior infection will last, Fauci said.
Taken together, it’s why Fauci and other experts, including CDC Director Rochelle Walensky, have increasingly predicted that elderly people will need a second booster shot soon. The Food and Drug Administration began reviewing data from Pfizer on the safety and efficacy this week, and its advisory panel will debate if and when the additional booster shot is necessary in the coming weeks.
At the same time, Fauci urged Americans who haven’t yet gotten their first booster, which would be their third shot in a Pfizer or Moderna series, to do so.
A resurgence of cases could also mean Americans are asked to wear masks again, which Fauci predicted would be an uphill battle.
“From what I know about human nature, which I think is pretty much a lot, people are kind of done with COVID,” Fauci said.
Still, he defended the CDC decision to loosen its mask recommendations earlier this month by shifting to a strategy that focused more on severe outcomes, like hospitalizations and deaths, rather than on daily case spread.
“You can go ahead and continue to tiptoe towards normality, which is what we’re doing, but at the same time, be aware that you may have to reverse,” Fauci said.
And if the U.S. does continue to make its way back toward normal times, Fauci himself has a personal choice to consider. At 81 years old, the director of the National Institute of Allergy and Infectious Diseases is “certainly” thinking about retirement.
“I have said that I would stay in what I’m doing until we get out of the pandemic phase and I think we might be there already, if we can stay in this,” Fauci said, referring to the falling cases and hospitalizations in the U.S.
“I can’t stay at this job forever. Unless my staff is gonna find me slumped over my desk one day. I’d rather not do that,” he said, laughing.
While he doesn’t currently have retirement plans, the recent hire of Dr. Ashish Jha, dean of the Brown University School of Public Health, to be White House coronavirus coordinator, could alleviate some of his pandemic response duties and give him a window.
But Fauci, who has dedicated his career to public health, primarily studying HIV and AIDS, and worked under seven U.S. presidents, said he doesn’t have any particular hobbies waiting for him in retirement.
“I, unfortunately, am somewhat of a unidimensional physician, scientist, public health person. When I do decide I’m going to step down, whenever that is, I’m going to have to figure out what it is I’m going to do,” he said.
“I’d love to spend more time with my wife and family. That would really be good.”
A surge in coronavirus infections in Western Europe has experts and health authorities on alert for another wave of the pandemic in the United States, even as most of the country has done away with restrictions after a sharp decline in cases.
Infectious-disease experts are closely watching the subvariant of omicron known as BA.2, which appears to be more transmissible than the original strain, BA.1, and is fueling the outbreak overseas.
In all, about a dozen nations are seeing spikes in coronavirus infections caused by BA.2, a cousin of the BA.1 form of the virus that tore through the United States over the past three months.
In the past two years, a widespread outbreak like the one now being seen in Europe has been followed by a similar surge in the United States some weeks later. Many, but not all, experts interviewed for this story predicted that is likely to happen. China and Hong Kong, on the other hand, are experiencing rapid and severe outbreaks, but the strict “zero covid” policies they have enforced make them less similar to the United States than Western Europe.
A number of variables — including relaxed precautions against viral transmission, vaccination rates, the availability of antiviral medications and natural immunity acquired by previous infection — may affect the course of any surge in the United States, experts said.
Most importantly, it is unclear at this point how many people will become severely ill, stressing hospitals and the health-care system as BA.1 did.
Another surge also may test the public’s appetite for returning to widespread mask-wearing, mandates and other measures that many have eagerly abandoned as the latest surge fades and spring approaches, experts said.
“It’s picking up steam. It’s across at least 12 countries … from Finland to Greece,” said Eric Topol, director of the Scripps Research Translational Institute in San Diego, who recently posted charts of the outbreak on Twitter. “There’s no question there’s a significant wave there.”
Topol noted that hospitalizations for covid-19, the disease caused by the virus, are rising in some places as well, despite the superior vaccination rates of many Western European countries.
At a briefing Monday, White House press secretary Jen Psaki said about 35,000 cases of BA.2 have been reported in the United States to date. But she offered confidence that “the tools we have — including mRNA vaccines, therapeutics and tests — are all effective tools against the virus. And we know because it’s been in the country.”
Kristen Nordlund, a spokeswoman for the Centers for Disease Control and Prevention, said in an email Tuesday that “although the BA.2 variant has increased in the United States over the past several weeks, it is not the dominant variant, and we are not seeing an increase in the severity of disease.”
The seven-day average of cases in the United States fell 17.9 percent in the past week, according to data tracked by The Washington Post, while the number of deaths dropped 17.2 percent and hospitalizations declined 23.2 percent.
Predicting the future course of the virus has proved difficult throughout the pandemic, and the current circumstances in Europe elicited a range of opinions from people who have closely tracked the pathogen and the disease it causes.
In the United States, just 65.3 percent of the population, 216.8 million people, are fully vaccinated, and only 96.1 million have received a booster shot, according to data tracked by The Post. In Germany, nearly 76 percent are fully vaccinated, according to the Johns Hopkins data, and the United Kingdom has fully vaccinated 73.6 percent.
That lower vaccination rate is very likely to matter as BA.2 spreads further in the United States, especially in regions where it is significantly lower than the national rate, several experts said. And even for people who are fully vaccinated and have received a booster shot, research data is showing that immunity to the virus fades over time. Vaccine-makers Pfizer and BioNTech asked the Food and Drug Administration on Tuesday for emergency authorization to offer a fourth shot to people 65 and older.
“Any place you have relatively lower vaccination rates, especially among the elderly, is where you’re going to see a bump in hospitalizations and deaths from this,” said Céline Gounder, an infectious-diseases physician and editor at large for public health at Kaiser Health News.
Similarly, as the public sheds masks — every state has dropped its mask mandate or announced plans to do so — another layer of protection is disappearing, several people tracking the situation said.
“Why wouldn’t it come here? Are we vaccinated enough? I don’t know,” said Kimberly Prather, a professor of atmospheric chemistry and an expert on aerosol transmission at the University of California at San Diego.
“So I’m wearing my mask still. … I am the only person indoors, and people look at me funny, and I don’t care.”
Yet BA.2 appears to be spreading more slowly in the United States than it has overseas, for reasons that aren’t entirely clear, Debbie Dowell, chief medical officer for the CDC’s covid-19 response, said in a briefing Saturday for clinicians sponsored by the Infectious Diseases Society of America.
“The speculation I’ve seen is that it may extend the curve going down, case rates from omicron, but is unlikely to cause another surge that we saw initially with omicron,” Dowell said.
One reason for that may be the immunity that millions of people acquired recently when they were infected with the BA.1 variant, which generally caused less-severe illness than previous variants. Yet no one really knows whether infection with BA.1 offers protection from BA.2.
“That’s the question,” said Jeffrey Shaman, an epidemiologist at the Columbia University Mailman School of Public Health. “Better yet, how long does it provide protection?”
Topol said the United States needs to improve its vaccination and booster rates immediately to protect more of the population against any coming surge.
“We have got to get the United States protected better. We have an abundance of these shots. We have to get them into people,” he said.
Biden administration officials said that whatever the further spread of BA.2 brings to the United States, the next critical step is to provide the $15.6 billion in emergency funding that Congress stripped from a deal to fund the government last week. That money was slated to pay for coronavirus tests, more vaccines and antiviral medications.
“That means that some programs, if we don’t get funding, could abruptly end or need to be pared back, Psaki said at Monday’s briefing. “And that could impact how we are able to respond to any variant.”
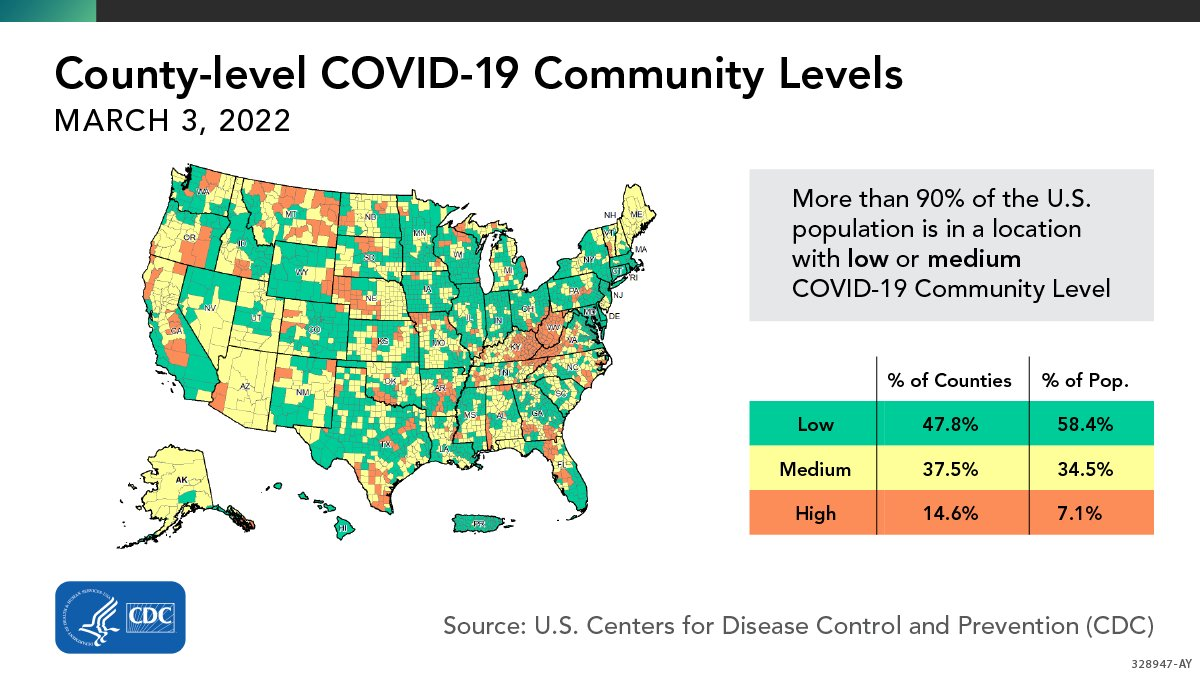
More than 90% of the U.S. population lives in an area with a “low” or “medium” risk of COVID-19, the U.S. Centers for Disease Control and Prevention (CDC) announced yesterday. Last week, the CDC changed the way it assesses county-level COVID-19 risk, using data on hospitalizations and health care capacity in addition to case counts. The CDC now recommends universal indoor masking only for counties that are at “high” risk under this system—which means that the vast majority of Americans are not currently advised to wear masks inside.
The U.S. may see an end to all pandemic restrictions, including mandatory mask-wearing, in the coming months, Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, told the Financial Times Feb. 8.
He said he hopes that the end to these restrictions will come soon and explained that the response to the pandemic going forward will be concentrated at a local level.
“As we get out of the full-blown pandemic phase of COVID-19, which we are certainly heading out of, these decisions will increasingly be made on a local level rather than centrally decided or mandated. There will also be more people making their own decisions on how they want to deal with the virus,” he told the FT.
The National Institute for Allergy and Infectious Diseases is preparing for the next pandemic by monitoring viruses that are known to cause severe illness.
This week the Biden Administration unveiled actions to make at-home COVID tests and N95 masks available, free of charge, to hundreds of millions of Americans. However, even as US COVID hospitalizations have now surpassed last winter’s previous peak, two newly-approved COVID antiviral drugs remain scarce. Just as fast as Omicron has surged across the country, it may be starting to recede, with cases beginning to drop in several states in the Northeast. Modelers now project the incredibly contagious variant will infect 40 percent of Americans and more than half the human race by the end of March.
The Gist:Absent another significant variant, experts are cautiously optimistic that enough of the US population will soon have either infection-acquired or vaccine-induced immunity that we may be nearing the end of the pandemic, and the beginning of “endemic COVID.”
The US must now shift from COVID “war footing” to learning how to live with the virus long term. That will mean tackling difficult and politically-charged decisions, such as what level of testing and masking are sustainable, and how many COVID deaths we are willing to tolerate.
Even as daily new COVID cases set all-time records and hospitals fill up, epidemiologists have arrived at a perhaps surprising consensus. Yes, the latest Omicron variant of the novel coronavirus is bad. But it could have been a lot worse.
Even as cases have surged, deaths haven’t—at least not to the same degree. Omicron is highly transmissible but generally not as severe as some older variants—“lineages” is the scientific term.
We got lucky. But that luck might not hold. Many of the same epidemiologists who have breathed a sigh of relief over Omicron’s relatively low death rate are anticipating that the next lineage might be much worse.
Fretting over a possible future lineage that combines Omicron’s extreme transmissibility with the severity of, say, the previous Delta lineage, experts are beginning to embrace a new public health strategy that’s getting an early test run in Israel: a four-shot regimen of messenger-RNA vaccine.
“I think this will be the strategy going forward,” Edwin Michael, an epidemiologist at the Center for Global Health Infectious Disease Research at the University of South Florida, told The Daily Beast.
Omicron raised alarms in health agencies all over the world in late November after officials in South Africa reported the first cases. Compared to older lineages, Omicron features around 50 key mutations, some 30 of which are on the spike protein that helps the virus to grab onto our cells.
Some of the mutations are associated with a virus’s ability to dodge antibodies and thus partially evade vaccines. Others are associated with higher transmissibility. The lineage’s genetic makeup pointed to a huge spike in infections in the unvaccinated as well as an increase in milder “breakthrough” infections in the vaccinated.
That’s exactly what happened. Health officials registered more than 10 million new COVID cases the first week of January. That’s nearly double the previous worst week for new infections, back in May. Around 3 million of those infections were in the United States, where Omicron coincided with the Thanksgiving, Christmas, and New Year holidays and associated traveling and family gatherings.
But mercifully, deaths haven’t increased as much as cases have. Worldwide, there were 43,000 COVID deaths the first week of January—fewer than 10,000 of them in the U.S. While deaths tend to lag infections by a couple weeks, Omicron has been dominant long enough that it’s increasingly evident there’s been what statisticians call a “decoupling” of cases and fatalities.
“We can say we dodged a bullet in that Omicron does not appear to cause as serious of a disease,” Stephanie James, the head of a COVID testing lab at Regis University in Colorado, told The Daily Beast. She stressed that data is still being gathered, so we can’t be certain yet that the apparent decoupling is real.
Assuming the decoupling is happening, experts attribute it to two factors. First, Omicron tends to infect the throat without necessarily descending to the lungs, where the potential for lasting or fatal damage is much, much higher. Second, by now, countries have administered nearly 9.3 billion doses of vaccine—enough for a majority of the world’s population to have received at least one dose.
In the United States, 73 percent of people have gotten at least one dose. Sixty-two percent have gotten two doses of the best mRNA vaccines. A third have received a booster dose.
Yes, Omicron has some ability to evade antibodies, meaning the vaccines are somewhat less effective against this lineage than they are against Delta and other older lineages. But even when a vaccine doesn’t prevent an infection, it usually greatly reduces its severity.
For many vaccinated people who’ve caught Omicron, the resulting COVID infection is mild. “A common cold or some sniffles in a fully vaxxed and boosted healthy individual,” is how Eric Bortz, a University of Alaska-Anchorage virologist and public health expert, described it to The Daily Beast.
All that is to say, Omicron could have been a lot worse. Viruses evolve to survive. That can mean greater transmissibility, antibody-evasion or more serious infection. Omicron mutated for the former two. There’s a chance some future Sigma or Upsilon lineage could do all three.
When it comes to viral mutations, “extreme events can occur at a non-negligible rate, or probability, and can lead to large consequences,” Michael said. Imagine a lineage that’s as transmissible as Omicron but also attacks the lungs like Delta tends to do. Now imagine that this hypothetical lineage is even more adept than Omicron at evading the vaccines.
That would be the nightmare lineage. And it’s entirely conceivable it’s in our future. There are enough vaccine holdouts, such as the roughly 50 million Americans who say they’ll never get jabbed, that the SARS-CoV-2 pathogen should have ample opportunities for mutation.
“As long as we have unvaccinated people in this country—and across the globe—there is the potential for new and possibly more concerning viral variants to arise,” Aimee Bernard, a University of Colorado immunologist, told The Daily Beast.
Worse, this ongoing viral evolution is happening against a backdrop of waning immunity. Antibodies, whether vaccine-induced or naturally occurring from past infection, fade over time. It’s not for no reason that health agencies in many countries urge booster doses just three months after initial vaccination. The U.S. Centers for Disease Control and Prevention is an outlier, and recommends people get boosted after five months.
A lineage much worse than Omicron could evolve at the same time that antibodies wane in billions of people all over the world. That’s why many experts believe the COVID vaccines will end up being annual or even semi-annual jabs. You’ll need a fourth jab, a fifth jab, a sixth jab, et cetera, forever.
Israel, a world leader in global health, is already turning that expectation into policy. Citing multiple studies that showed a big boost in antibodies with an additional dose of mRNA and no safety concerns, the country’s health ministry this week began offering a fourth dose to anyone over the age of 60, who tend to be more vulnerable to COVID than younger people.
That should be the standard everywhere, Ali Mokdad, a professor of health metrics sciences at the University of Washington Institute for Health, told The Daily Beast. “Scientifically, they’re right,” he said of the Israeli health officials.
If there’s a downside, it’s that there are still a few poorer countries—in Africa, mostly—where many people still struggle to get access to any vaccine, let alone boosters and fourth doses. If and when other richer countries follow Israel’s lead and begin offering additional jabs, there’s some risk of even greater inequity in global vaccine distribution.
“The downside is for the rest of the world,” Mokdad said. “I’m waiting to get my first dose and you guys are getting a fourth?”
The solution isn’t to deprive people of the doses they need to maintain their protection against future—and potentially more dangerous—lineages. The solution, for vaccine-producing countries, is to further boost production and double down on efforts to push vaccines out to the least privileged communities.
A sense of urgency is key. For all its rapid spread, Omicron has actually gone fairly easy on us. Sigma or Upsilon might not.
Over the past two years, historians and analysts have compared the coronavirus to the 1918 flu pandemic. Many of the mitigation practices used to combat the spread of the coronavirus, especially before the development of the vaccines, have been the same as those used in 1918 and 1919 — masks and hygiene, social distancing, ventilation, limits on gatherings (particularly indoors), quarantines, mandates, closure policies and more.
Yet, it may be that only now, in the winter of 2022, when Americans are exhausted with these mitigation methods, that a comparison to the 1918 pandemic is most apt.
The highly contagious omicron variant has rendered vaccines much less effective at preventing infections, thus producing skyrocketing caseloads. And that creates a direct parallel with the fall of 1918, which provides lessons for making January as painless as possible.
In February and March 1918, an infectious flu emerged. It spread from Kansas, through World War I troop and material transports, filling military post hospitals and traveling across the Atlantic and around the world within six months. Cramped quarters and wartime transport and industry generated optimal conditions for the flu to spread, and so, too, did the worldwide nature of commerce and connection. But there was a silver lining: Mortality rates were very low.
In part because of press censorship of anything that might undermine the war effort, many dismissed the flu as a “three-day fever,” perhaps merely a heavy cold, or simply another case of the grippe (an old-fashioned word for the flu).
Downplaying the flu led to high infection rates, which increased the odds of mutations. And in the summer of 1918, a more infectious variant emerged. In August and September, U.S. and British intelligence officers observed outbreaks in Switzerland and northern Europe, writing home with warnings that went largely unheeded.
Unsurprisingly then, this seemingly more infectious, much more deadly variant of H1N1 traveled west across the Atlantic, producing the worst period of the pandemic in October 1918. Nearly 200,000 Americans died that month. After a superspreading Liberty Loan parade at the end of September, Philadelphia became an epicenter of the outbreak. At its peak, nearly 700 Philadelphians died per day.
Once spread had begun, mitigation methods such as closures, distancing, mask-wearing and isolating those infected couldn’t stop it, but they did save many lives and limited suffering by slowing infections and spread. The places that fared best implemented proactive restrictions early; they kept them in place until infections and hospitalizations were way down, then opened up gradually, with preparations to reimpose measures if spread returned or rates elevated, often ignoring the pleas of special interests lobbying hard for a complete reopening.
In places in the United States where officials gave in to public fatigue and lobbying to remove mitigation methods, winter surges struck. Although down from October’s highs, these surges were still usually far worse than those in the cities and regions that held steady.
In Denver, in late November 1918, an “amusement” lobby — businesses and leaders invested in keeping theaters, movie houses, pool halls and other public venues open — successfully pressured the mayor and public health officials to rescind and then revise a closure order. This, in turn, generated what the Rocky Mountain News called “almost indescribable confusion,” followed by widespread public defiance of mask and other public health prescriptions.
In San Francisco, where resistance was generally less successful than in Denver, there was significant buy-in for a second round of masking and public health mandates in early 1919 during a new surge. But opposition created an issue. An Anti-Mask League formed, and public defiance became more pronounced. Eventually anti-maskers and an improving epidemic situation combined to end the “masked” city’s second round of mask and public health mandates.
The takeaway: Fatigue and removing mitigation methods made things worse. Public officials needed to safeguard the public good, even if that meant unpopular moves.
The flu burned through vulnerable populations, but by late winter and early spring 1919, deaths and infections dropped rapidly, shifting toward an endemic moment — the flu would remain present, but less deadly and dangerous.
Overall, nearly 675,000 Americans died during the 1918-19 flu pandemic, the majority during the second wave in the autumn of 1918. That was 1 in roughly 152 Americans (with a case fatality rate of about 2.5 percent). Worldwide estimates differ, but on the order of 50 million probably died in the flu pandemic.
In 2022, we have far greater biomedical and technological capacity enabling us to sequence mutations, understand the physics of aerosolization and develop vaccines at a rapid pace. We also have a far greater public health infrastructure than existed in 1918 and 1919. Even so, it remains incredibly hard to stop infectious diseases, particularly those transmitted by air. This is complicated further because many of those infected with the coronavirus are asymptomatic. And our world is even more interconnected than in 1918.
That is why, given the contagiousness of omicron, the lessons of the past are even more important today than they were a year ago. The new surge threatens to overwhelm our public health infrastructure, which is struggling after almost two years of fighting the pandemic. Hospitals are experiencing staff shortages (like in fall 1918). Testing remains problematic.
And ominously, as in the fall of 1918, Americans fatigued by restrictions and a seemingly endless pandemic are increasingly balking at following the guidance of public health professionals or questioning why their edicts have changed from earlier in the pandemic. They are taking actions that, at the very least, put more vulnerable people and the system as a whole at risk — often egged on by politicians and media figures downplaying the severity of the moment.
Public health officials also may be repeating the mistakes of the past. Conjuring echoes of Denver in late 1918, under pressure to prioritize keeping society open rather than focusing on limiting spread, the Centers for Disease Control and Prevention changed its isolation recommendations in late December. The new guidelines halved isolation time and do not require a negative test to reenter work or social gatherings.
Thankfully, we have an enormous advantage over 1918 that offers hope. Whereas efforts to develop a flu vaccine a century ago failed, the coronavirus vaccines developed in 2020 largely prevent severe illness or death from omicron, and the companies and researchers that produced them expect a booster shot tailored to omicron sometime in the winter or spring. So, too, we have antivirals and new treatments that are just becoming available, though in insufficient quantities for now.
Those lifesaving advantages, however, can only help as much as Americans embrace them. Only by getting vaccinated, including with booster shots, can Americans prevent the health-care system from being overwhelmed. But the vaccination rate in the country remains a relatively paltry 62 percent, and only a scant 1 in 5 have received a booster shot. And as in 1918, some of the choice rests with public officials. Though restrictions may not be popular, officials can reimpose them — offering public support where necessary to those for whom compliance would create hardship — and incentivize and mandate vaccines, taking advantage of our greater medical technology.
As the flu waned in 1919, one Portland, Ore., health official reflected that “the biggest thing we have had to fight in the influenza epidemic has been apathy, or perhaps the careless selfishness of the public.”
The same remains true today.
Vaccines, new treatments and century-old mitigation strategies such as masks, distancing and limits on gatherings give us a pathway to prevent the first six weeks of 2022 from being like the fall of 1918. And encouraging news about the severity of omicron provides real optimism that an endemic future — in which the coronavirus remains but poses far less of a threat — is near. The question is whether we get there with a maximum of pain or a minimum. The choice is ours.