In talking to our health system members from across the country in the past few weeks, we’ve heard that the COVID surge is happening everywhere. Nearly everyone we’ve talked to has told us that their inpatient census of COVID patients is as high or higher now than during the initial wave of the pandemic in March and April. And nearly everyone is expecting it to get much worse over the next few weeks, as hospitalizations increase in the wake of the explosion of cases we’re seeing now.
But there is something striking in our conversations in comparison to eight months ago: no one seems to be panicking. Crisis management processes that were developed and honed early in the pandemic are proving very helpful now. Normal patient care services are continuing despite the uptick in COVID volume, and protections are in place to keep the care environment segregated and COVID-free as possible.
While dozens of health systems, many in the hardest hit states in the Midwest and Great Plains, have announced plans to curtail elective care during this third wave, the decisions are based on individual hospital capacity and staffing, instead of being mandated by states. Having largely worked through the “COVID backlog” across the summer and early fall, system leaders want to avoid canceling surgeries again, and few are expecting state governments to force them to.
Many of our members have drawn up plans for selective cancellations depending on capacity, but we’re not likely to see sweeping shutdowns again—unless the workforce becomes so overstretched that it impacts operations.
That’s good news, and will likely lead to less interrupted patient care. And it’s good news for hospitals’ and doctors’ economic survival, as many would not be able to absorb the body blow of another widespread shutdown. Fingers crossed.
A group of health system leaders in Missouri challenged state-reported hospital bed data, saying it could lead to a misunderstanding about hospital capacity, according to a Nov. 19 report in the St. Louis Business Journal.
A consortium of health systems, including St. Louis-based BJC HealthCare, Mercy, SSM Health and St. Luke’s Hospital, released urgent reports warning that hospital and ICU beds are nearing capacity while state data reports show a much different story.
The state reports, based on data from TeleTracking and the CDC-managed National Healthcare Safety Network, show inpatient hospital bed capacity at 35 percent and remaining ICU bed capacity at 29 percent on Nov. 19. However, the consortium reported hospitals are fuller, at 84 percent capacity as of Nov. 18, and ICUs at 90 percent capacity based on staffed bed availability. The consortium says it is using staffed bed data while the state’s numbers are based on licensed bed counts; the state contends it does take staffing into account, according to the report.
Stephanie Zoller Mueller, a spokesperson for the consortium, said the discrepancy between the state’s data and consortium’s data could create a “gross misunderstanding on the part of some and can be a dangerous message to the community.”
Sioux Falls, S.D.-based Sanford Health President and CEO Kelby Krabbenhoft shared his thoughts about having COVID-19 and why he won’t be wearing a mask in an email to health system staff, according to the Grand Forks Herald.
In the 1,000-word email sent Nov. 18, Mr. Krabbenhoft said he had COVID-19, but he’s now back in his office working without a mask. He said he won’t be wearing a mask because doing so would only be a “symbolic gesture.” He considers himself immune from the virus.
“The information, science, truth, advice and growing evidence is that I am immune for at least seven months and perhaps for years to come, similar to that of chicken pox, measles, etc. For me to wear a mask defies the efficacy and purpose of a mask and sends an untruthful message that I am susceptible to infection or could transmit it,” Mr. Krabbenhoft wrote. “I have no interest in using masks as a symbolic gesture when I consider that my actions in support of our family leave zero doubt to my support of all 50,000 of you. My team and I have a duty to express the truth and facts and reality and not feed the opposite.”
The CDC says those who have had COVID-19 should take steps to reduce the risk of spreading the virus, including wearing a mask in public places and staying at least 6 feet away from other people.
In his email, Mr. Krabbenhoft argues the “on-again, off-again” use of masks is absurd. “Masks have been a symbolic issue that frankly frustrates me,” he wrote.
“On the other hand, for people who have not contracted the virus and may acquire it and then spread it … it is important for them to know that masks are just plain smart to use and in their best interest,” Mr. Krabbenhoft wrote.
The health system CEO concluded his letter by sharing his optimism for the future, noting that some Sanford Health workers would be among the first to get a COVID-19 vaccine once it is available.
Sanford Health didn’t respond to Becker’s Hospital Review‘s request for comment by deadline.
Read the Grand Forks Herald article here, which includes full text of the email Mr. Krabbenhoft sent to employees.
At least 250,000 people in the United States have died of covid-19, the disease caused by the coronavirus, since February, and many public health officials warn the pandemic is just entering its deadliest phase. Yet, as the country confronts this horrifying death toll, there is little understanding of what a loss of this size represents.
Here is some historical perspective about losing a quarter of a million people, looking at major events in our past that have cost American lives.
More than 58,000 Americans were killed during the decade-plus of involvement in the Vietnam War. So the pandemic’s fatalities represent four Vietnam Wars since February.
During the Korean War, nearly 37,000 Americans were lost; covid-19 has claimed nearly seven times more.
During World War II, the country mourned 405,000 members of the “Greatest Generation.” The pandemic has taken nearly two-thirds as many people, a lot of them old enough to remember the fight against the Nazis and the Japanese.
And World War I? 116,000 U.S. dead in two years of fighting. The pandemic has more than doubled that number in a fraction of the time.
What about our deadliest conflict, the Civil War? Death toll estimates range from 600,000 to 850,000. Even at the high end of that range, the pandemic has permanently taken nearly 30 percent as many family members from Thanksgiving tables.
On Sept. 11, 2001, almost 3,000 people were killed in terrorist attacks in New York, Washington and Shanksville, Pa.
The deadliest day of the pandemic so far — Sept. 18 — surpassed that, at 3,660 deaths. Wednesday, as the virus surged across the country, the daily death toll had risen again to 1,894. Public health officials fear that by the end of this month, the United States could lose more people per day from the pandemic than the 2,403 Americans killed inthe Japanese attack on Pearl Harbor on Dec. 7, 1941.
And how does this pandemic compare to others in U.S. history?
The Centers for Disease Control and Prevention keeps records on four of them. The 2009 H1N1 pandemic killed 12,469 Americans. The 1968 Influenza A pandemic killed about 100,000 people. And the 1957-1958 Influenza A pandemic took 116,000 U.S. lives.
One of the more conservative disease models currently projects the United States could reach 438,000 deaths, more than during World War II, by March 1, 2021.
No state in America could clear the threshold right now to safely allow indoor gatherings, Axios’ Sam Baker and Andrew Witherspoon report.
The big picture: This is bad as the pandemic has ever been — the most cases, the most explosive growth and the greatest strain on hospitals.
If businesses were closed right now, it would not be safe to reopen them. And holiday travel will be risky no matter where you’re coming from or where you’re going.
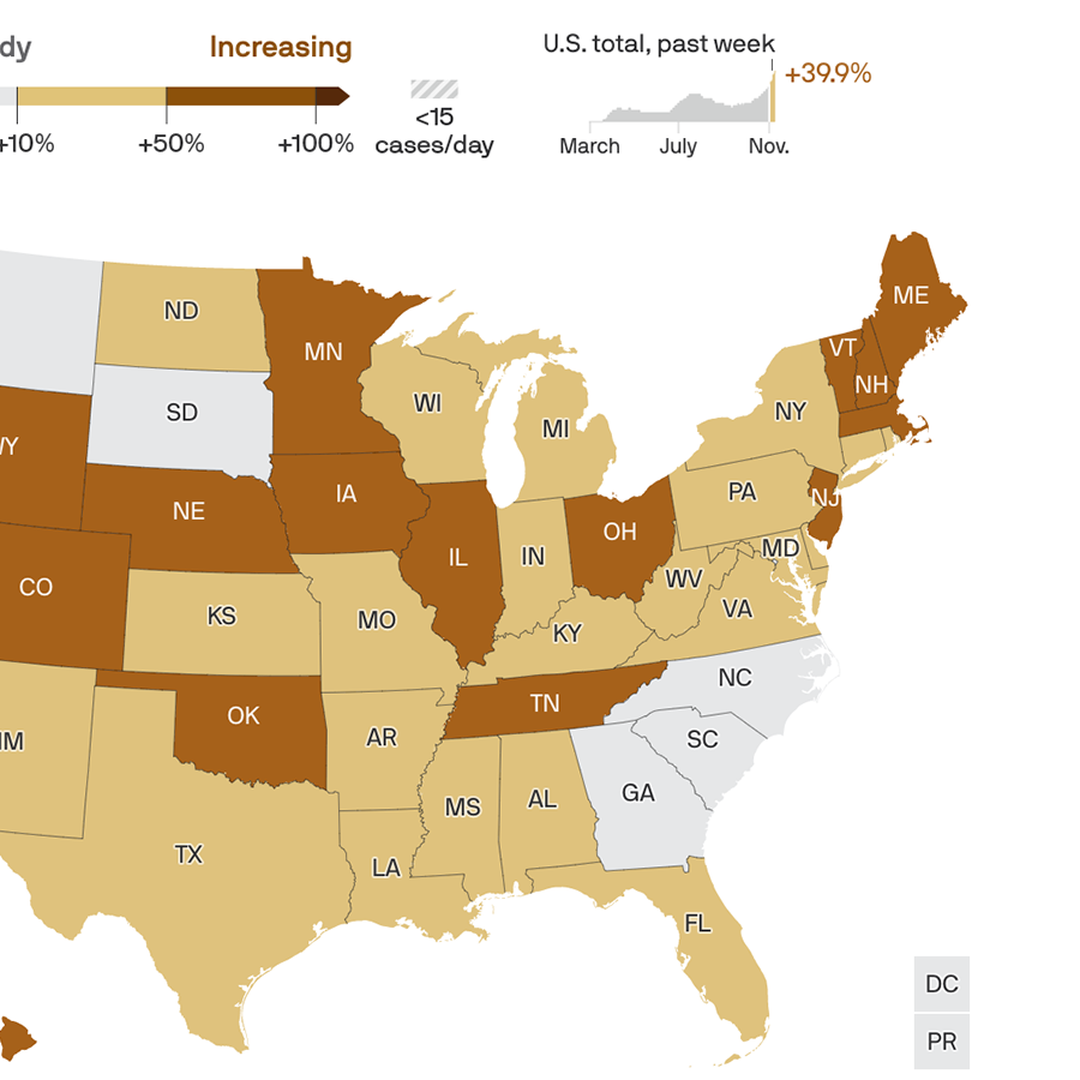
By the numbers: Over the past week, the U.S. averaged more than 154,000 new cases per day, the highest rate of the entire pandemic.
The number of new infections rose in 46 states, held steady in three, and declined in only one — Hawaii.
This week’s nationwide totals are a 30% increase over last week, which was a 40% increase over the week before that. Daily infections have been rising by at least 15% for the past six weeks.
Testing was up about 11% over the past week. The U.S. is now conducting about 1.5 million tests per day. That’s a lot, but cases clearly are still rising faster than testing.
Between the lines:Whatever metric you might use to decide whether it’s safe to have a large Thanksgiving get-together, or to sit inside a bar or restaurant, the answer is probably no.
Experts recently told The Atlantic that they wouldn’t feel comfortable attending an indoor dinner party at all, but that it would be least risky in areas with only about 10–25 new cases per day, per 100,000 people.
The bottom line: Eating and drinking indoors with large groups of people, at a time when 150,000 people are contracting the virus every day, is about as risky as it gets.
The disease caused by the novel coronavirus has killed at least 247,000 people in the United States since February and has enveloped nearly every part of the country.
As health officials long predicted, autumn brought soaring case counts, strained hospital capacity and increased deaths nationwide, as the virus is not only popping up in new places but also circling back to areas that once appeared to have it contained. Nearly all metrics in most of the country are trending in the wrong direction.
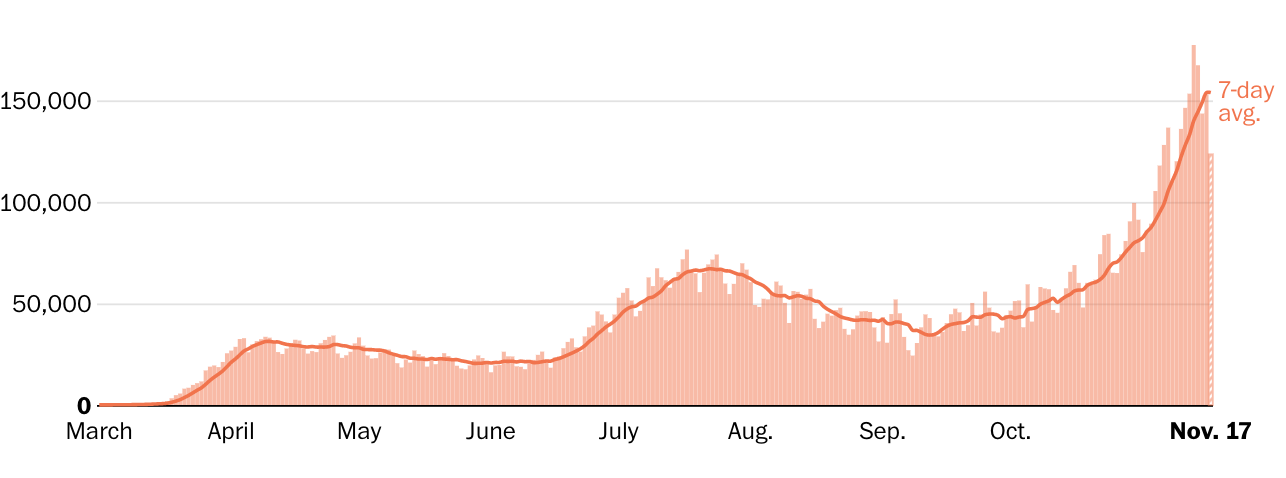
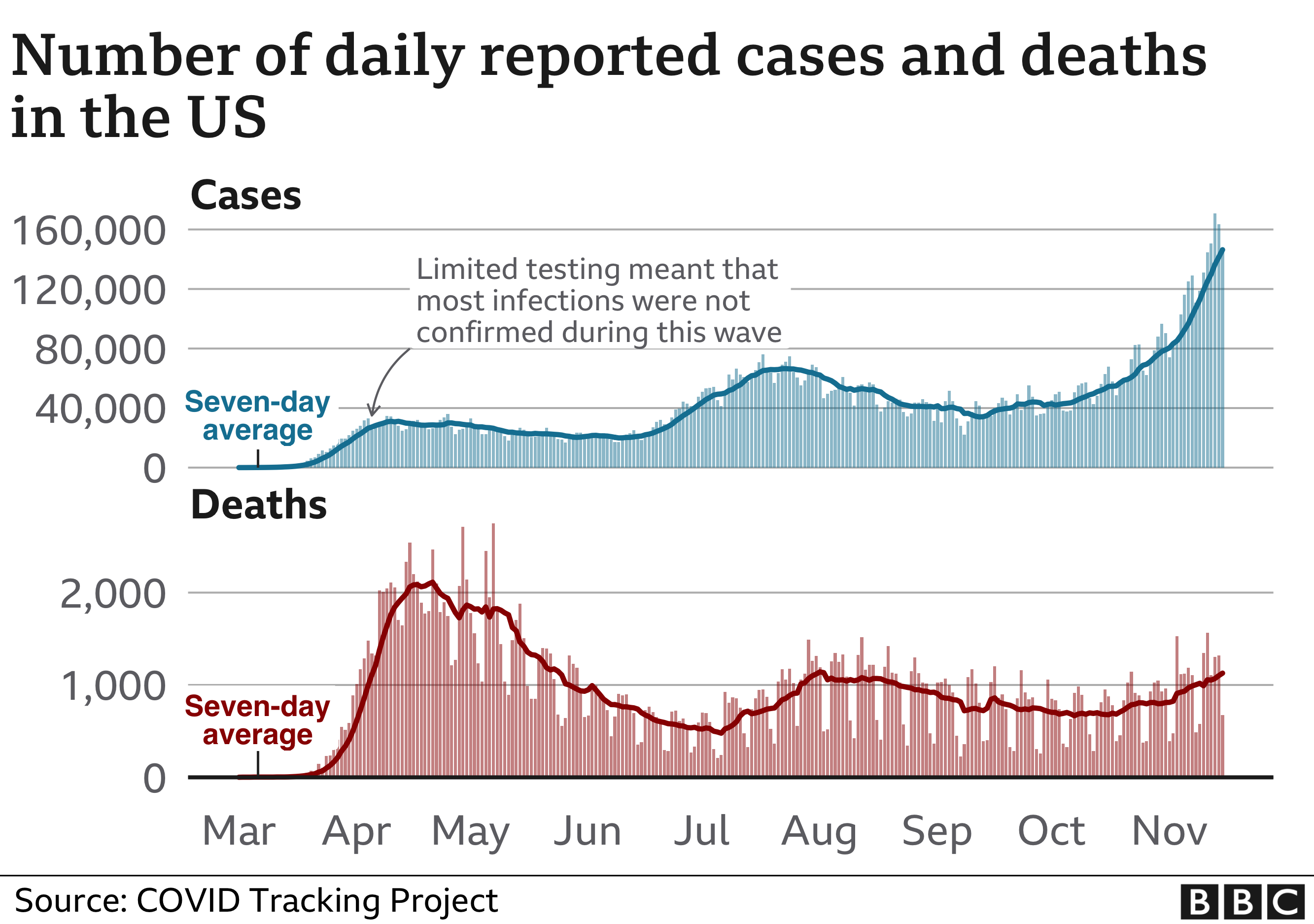
During an April peak, the seven-day-average U.S. death toll hit more than 2,000 per day, but cases were concentrated largely in the Northeast. During a July lull, average deaths sank to a low of 463 per day, although cases surged in the Sun Belt.
By early November, however, the country was recording more new cases than ever — well over 100,000 per day — and many states reported record-high caseloads and hospitalizations. The average U.S. deaths per day again shot past 1,000, despite improvements in treatment that make survival more likely.
In the past week in the U.S….New daily reported cases rose 26% New daily reported deaths rose 13.5% Covid related hospitalizations rose 23.9%.
Among reported tests, the positivity rate was 10%.
The number of tests reported rose 9.6% from the previous week.
Numbers in this article have fluctuated as testing and reporting criteria have evolved, particularly in areas that were hit early. Three spikes in the deaths chart above reflect large, one-time adjustments: In mid-April, New York City added more than 3,700 deaths. New Jersey added more than 1,800 on June 25. And in September, The Post changed its methodology for reporting deaths in New York and added a one-day increase of more than 2,700 on Sept. 18.
Health officials, including the country’s top infectious disease expert, Anthony S. Fauci, have said the virus has killed more people than official death tolls indicate.
New York, which was slammed with the new disease in spring and where at least 33,000 have died, is one of several states experiencing a second or even third wave.
Sun Belt states had serious outbreaks after Memorial Day when people flocked to beaches. By late summer, parts of the Midwest were inundated. In August and September, clusters appeared in newly reopened college campuses, particularly in the Northeast and Midwest. By October, Upper Midwest, Great Plains and Western states that had previously been mostly spared were reporting major outbreaks, including Minnesota, Wisconsin, Arkansas, the Dakotas and Alaska.
In November, most states reported record-high case counts and greater demand for hospital beds. Several set records for single-day fatalities.
A majority of states and many retail chains required masks in public places by late July, and public health officials touted them as one of the easiest ways to stop the pandemic. Still, some people in even the hardest-hit areas refuse to wear them, despite evidence that they protect wearers and those around them.
People older than 65 and those with obesity and underlying health problems are the mostly likely to die from covid-19, but a large percentage of infections occur in younger, more mobile people. People younger than 40 tend to become less sick but also unknowingly may pass the disease to others around them.
Sparsely populated areas don’t have the huge raw numbers that cities have reported, but some rank among the highest in deaths and cases per capita.
By late October, covid-19 had been documented in all but three U.S. counties and areas in Montana, the Dakotas and Idaho had some of the highest per capita caseloads.
People in very rural areas may be more vulnerable to covid-19 than urbanites, according to a Post analysis of CDC data.
Demand has often overwhelmed testing infrastructure, muddying the ability of officials to get a true picture of the virus’s reach. In June, CDC Director Robert Redfield estimated that, based on antibody tests, the actual number of U.S. residents who had been infected by the virus was likely to be 10 times as high as the number of confirmed cases. More recently, conflicting CDC guidelines about whether people without symptoms should be tested caused confusion and inhibited contact tracing.
A sharp increase in hospitalizations in late October and November demonstrates that the virus is spreading, not just that more testing is finding more asymptomatic cases. A group of Illinois health-care workers predicted in a Nov. 10 open letter to state and Chicago officials that “Illinois will surpass its ICU bed capacity by Thanksgiving.”
Some hospitals, straining to find beds and health-care workers to handle the crush of patients, are considering unusual measures.
In North Dakota, health-care workers who test positive but have no symptoms can continue working in covid-19 wards, according to Gov. Doug Burgum (R). Some facilities in Oklahoma, Kansas and Ohio are limiting routine care and deferring non-emergency surgeries.
Not all news is bleak, however.
On Nov. 9, Pfizer announced that its promising vaccine — one of many in the works — appeared more than 90 percent effective in an ongoing trial. The same day, regulators granted emergency authorization to an antibody treatment that may keep mild illness from becoming severe.
And the next day, Fauci told CNN that the average American may have access to a vaccine by April.
State-level reports are the best publicly available data on child COVID-19 cases in the United States. The American Academy of Pediatrics and the Children’s Hospital Association are collaborating to collect and share all publicly available data from states on child COVID-19 cases (definition of “child” case is based on varying age ranges reported across states; see report Appendix for details and links to all data sources).
As of November 12th, over 1 million children have tested positive for COVID-19 since the onset of the pandemic. The age distribution of reported COVID-19 cases was provided on the health department websites of 49 states, New York City, the District of Columbia, Puerto Rico, and Guam. Children represented 11.5% of all cases in states reporting cases by age.
A smaller subset of states reported on hospitalizations and mortality by age; the available data indicated that COVID-19-associated hospitalization and death is uncommon in children.
The number of new child COVID-19 cases reported this week, nearly 112,000, is by far the highest weekly increase since the pandemic began. At this time, it appears that severe illness due to COVID-19 is rare among children. However, there is an urgent need to collect more data on longer-term impacts on children, including ways the virus may harm the long-term physical health of infected children, as well as its emotional and mental health effects.
Summary of Findings (data available as of 11/12/20) :
(Note: Data represent cumulative counts since states began reporting)
Cumulative Number of Child COVID-19 Cases*
1,039,464 total child COVID-19 cases reported, and children represented 11.5% (1,039,464/9,037,991) of all cases
Overall rate: 1,381 cases per 100,000 children in the population
Change in Child COVID-19 Cases*
111,946 new child COVID-19 cases were reported the past week from 11/5-11/12 (927,518 to 1,039,464)
Over two weeks, 10/29-11/12, there was a 22% increase in child COVID-19 cases (185,829 new cases (853,635 to 1,039,464))
Testing (10 states reported)*
Children made up between 5.0%-17.4% of total state tests, and between 3.9%-18.8% of children tested were tested positive
Hospitalizations (23 states and NYC reported)*
Children were 1.2%-3.3% of total reported hospitalizations, and between 0.5%-6.1% of all child COVID-19 cases resulted in hospitalization
Mortality (42 states and NYC reported)*
Children were 0.00%-0.21% of all COVID-19 deaths, and 16 states reported zero child deaths
In states reporting, 0.00%-0.15% of all child COVID-19 cases resulted in death
* Note: Data represent cumulative counts since states began reporting; All data reported by state/local health departments are preliminary and subject to change
Like a lot of people, I have really gotten into listening to podcasts over the last year. They’re such an immersive way to learn about the world, and I like how the format lets you dive as deep on a topic as you want. So, I was inspired to start one of my own—but I knew I couldn’t do it on my own.
I couldn’t ask for a better partner on this project than Rashida Jones. A mutual friend suggested that the two of us might have a lot to talk about, and it turned out he was right. I already knew she was a talented actor, but I was impressed by her thoughtful perspective on the world. So, we decided to start a podcast that lets us think through some of today’s most pressing problems together. In our first episode, Rashida and I explore a big question that is top of mind for many people: what will the world look like after COVID-19?
I know it’s hard to imagine right now while new cases are surging around the world, but there will come a time when the COVID-19 pandemic is behind us. I think it’s safe to assume that society will be changed forever, given how disruptive the virus has been to virtually every part of our lives.
Unfortunately, we still have a long way to go before life truly gets back to “normal.” Rashida and I were joined by Dr. Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases, to discuss what to expect in the months to come. I’ve had the opportunity to work with Dr. Fauci on a number of global health issues over the years, including the quest for an HIV vaccine and cure. He’s such a quiet and unassuming guy normally, so it’s been wild to watch him become a huge celebrity.
Dr. Fauci and I are both optimistic that a vaccine will bring an end to the pandemic at some point in the near future. But what the world looks like after that is a lot less clear. I suspect that some of the digitization trends we’ve seen—especially in the areas of online learning, telemedicine, and remote work—will become a regular part of our lives. I hope this episode leaves you hopeful about the future and curious about what comes next.
Coronavirus cases reported in the United States passed 11 million on Sunday, as the nation shatters records for hospitalizations and daily new infections and as leaders turn to new, painful restrictions to stem the pandemic’s long-predicted surge.
The milestone came one week after the country hit 10 million cases, a testament to just how rapidly the virus is spreading — the first 1 million cases took more than three months. This new wave has increased covid-19 hospitalizations past the peaks seen in April and July, straining health-care systems and pushing some reluctant Republican governors to enact statewide mask mandates for the first time.
Other states are reenacting stay-at-home orders and store closures. Michigan Gov. Gretchen Whitmer (D) on Sunday announced sweeping new limits on gatherings for three-weeks — including a ban on indoor dining at restaurants and bars, and a halt to in-person classes at high schools and colleges. Washington Gov. Jay Inslee (D) also laid out a slew of new rules, which prohibit indoor social gatherings with people outside one’s household and indoor service at restaurants, bars and more.
“As hard as those first months were for our state, these next few are going to be even harder,” Whitmer said at a news conference, as health experts fear that winter weather driving people indoors will accelerate the crisis.
Inslee acknowledged that slowing the virus would come at a steep price for struggling businesses, even as the state works to distribute millions more in aid. He and Whitmer both appealed to the federal government to step in with more help. Congress remains deadlocked on a stimulus package, and President Trump — still denying his election loss — has largely tuned out the pandemic’s surge; his refusal to concede is also stalling the transition to a new administration, including the formal transfer of information on the nation’s pandemic response.
Whitmer said that Trump has “an opportunity to meet the needs of the people of this country” and emphasized the importance of his final months in office. Inslee was already looking ahead to the administration of President-elect Joe Biden.
“All of us who feel, as I do, the pain of the small-business people ought to be pounding the doors of the Congress and the new president, who I’m glad we’re going to have, to really get this job done,” Inslee said.
Washington’s restrictions are not as tough as its stay-at-home order issued in March but extend into nearly every aspect of daily life. Wedding and funeral receptions are forbidden. Religious services and in-store retail are forced to operate at reduced capacity. Even outdoor social gatherings must be kept to a maximum of five people from outside one’s household.
Inslee and other leaders in the state emphasized the need to intervene early amid spiraling statistics, even as Washington posts some of the lowest numbers for new coronavirus infections in the country. The number of hospital patients with covid-19 recently rose about 40 percent in a week, officials said, and Seattle’s mayor said that nearly a fifth of the city’s cases have come just in the past two weeks.
Clint Wallace, an ICU nurse in Spokane, joined Inslee at Sunday’s news conference to plead with residents for their help. He called the ICU “as busy as I’ve seen it.”
“We are exhausted,” Wallace said of health-care workers around the state.
State and local officials nationwide are reinstating restrictions to fight the virus. New Mexico and Oregon on Friday ordered extensive new statewide shutdowns, while the Navajo Nation — devastated early on by the virus — reissued its stay-at-home order for at least three weeks. The Navajo Nation said cases threaten to swamp the health system on the southwestern reservation without immediate action.
North Dakota Gov. Doug Burgum (R) on Friday issued a statewide mask mandate and new capacity limits on businesses, less than a week after Utah Gov. Gary R. Herbert (R) announced a similar mask order in the face of overwhelmed hospitals warning that they might have to ration care.
“Our situation has changed, and we must change with it,” Burgum said in a late-night video message.
But state rules are just one piece of the puzzle, and some leaders are looking to Congress and the incoming president to take stronger action.
Ron Klain, Joe Biden’s incoming chief of staff, said Sunday it’s critical for the president-elect’s transition team to start working with Trump administration officials to ensure “nothing drops in this change of power” that could imperil the distribution of a potential coronavirus vaccine.
“Joe Biden is going to become president of the United States in the midst of an ongoing crisis. That has to be a seamless transition,” Klain said on NBC News’s “Meet the Press.”
President Trump’s White House is blocking the administration from formally cooperating with Biden, forcing the president-elect’s transition team to continue preparations with recently departed government officials and other experts. That means Biden’s team has not heard from Trump’s about vaccine development and other work to combat the pandemic.
A health expert on Biden’s covid-19 advisory board said there’s “a lot of information that needs to be transmitted. It can’t wait until the last minute.”
It is in the nation’s interest that the transition team get the threat assessments that the team knows about, understand the vaccine distribution plans, need to know where the stockpiles are, what the status is of masks and gloves,” said Atul Gawande, a surgeon at Brigham and Women’s Hospital and a professor at Harvard Medical School, on ABC News’s “This Week.”
Anthony S. Fauci, head of the National Institute of Allergy and Infectious Diseases, compared the process Sunday to “passing a baton in a race.”
“I’ve been through multiple transitions now, having served six presidents for 36 years, and it’s very clear that transition process that we go through … is really important in a smooth handing over of the information,” Fauci said on CNN’s “State of the Union.”
“Of course it would be better if we could start working with them,” he added when asked whether working with Biden’s team would serve the public interest.
On “Meet the Press,” Klain said there is “not that much Joe Biden can do right now to change things,” because he is not yet president.
“Right now we have a crisis that’s getting worse,” Klain said. “We had never had a day with 100,000 cases in a single day until last week. By next week, we may see 200,000 cases in a single day.”