

Cartoon – Your Blood Pressure is Too Low


http://www.healthcaredive.com/news/healthcare-workforce-growth-cuts/446182/

Employment in the healthcare industry has risen since the ACA was passed, but many health systems have been trimming their workforce under financial pressure.
It’s clear there have been a fair amount of hospital and provider layoffs in 2017.
In the past few months, hospitals of all sizes, and in all parts of the country, have said they are cutting jobs or eliminating open positions. Major providers affected have included Memorial Hermann, Brigham and Women’s Hospital, NYC Health + Hospitals, Summa Health and Hallmark Health. In May, Becker’s Hospital Review listed 48 layoffs across the industry the publication had reported on in 2017.
The layoffs come in contrast with the sharp rise in hiring in the healthcare sector ever since the Affordable Care Act (ACA) was enacted. While the hiring growth is a long-term trend — though it’s yet to be determined at what rate in 2017 — these layoffs are due in part to the short-term trends of softening admissions and flattening reimbursements. Many providers cited similar problems: declining reimbursements, lower admissions and shrinking operating incomes. Layoffs aren’t the only play for struggling organizations, but hospital expenses are rising on multiple fronts, and executives have to make some hard choices.
Big drivers of the growth are the aging population and the pending retirement of many registered nurses. It’s unclear how or when the layoff and healthcare job growth trends will change, but the underlying themes are not going away. The Bureau of Labor Statistics (BLS) is scheduled to release 2016-2026 occupational projections in October, while layoffs will continue to be tracked throughout the year.
Then there’s the elephant in the room over the buzzword of 2017: Uncertainty. Whether it be in Congress or in the executive branch, uncertainty over U.S. healthcare policy is making providers nervous as the insurance open enrollment period nears with no clear ACA reform or repeal in sight.
To date, the healthcare employment bubble hasn’t burst. Healthcare jobs, including hospital jobs, still are on the rise. While job growth is a different metric than layoffs and require different considerations, both underscore the themes affecting the industry’s workforce.
Ani Turner, co-director of Altarum Institute’s Center for Sustainable Health Spending, told Healthcare Dive there have been some clear trends in hospital job growth in recent years. In 2013, there was little job growth but the expanded coverage affect — where more individuals gained health insurance for the first time under the ACA — helped spur hospital job growth in 2014.
This expanded coverage helped hospitals experience new revenue opportunities thanks to more people entering the care delivery space, especially in states that expanded Medicaid. In addition, since the implementation of the ACA, the level of uncompensated care nationwide has gone down from $46.4 billion in 2013 to $35.7 billion in 2015.
Since that time, hospitals experienced great growth from a jobs perspective. In a 2015 Forbes article, Politico’s Dan Diamond noted that healthcare job growth surged at its fastest pace since 1991 starting in July 2014 up through May of 2015. In fact, healthcare practitioners and healthcare support positions are expected to be among the fastest growing jobs from 2014 to 2024. BLS notes the aging population and expanded insurance coverage will help fuel this growth as demand for healthcare services increases.
The recent surge is “somewhat unexpected,” Turner says. “One would think hospitals would be conservative in their hiring. Everything I’m seeing is flat or slightly declining volumes, especially on inpatient side.”
“The data don’t always cooperate with the story that makes sense,” Turner added.
Brian Augustian, principal at Deloitte, believes the job growth is going to continue to slow this year in part because there will be a push for greater automation and productivity. “As organizations are able to use machine learning, artificial intelligence and better utilize technology to get tasks done, it will not only result in…needing fewer people but also different types of people,” he told Healthcare Dive.
The rate of job growth will be an issue to watch throughout the year. As shown above, just two months worth of data changes the story from a narrative of “slowing growth” to “continuing to soar.” The looming retirement of registered nurses and the aging population do point to hospitals and providers arming themselves to smooth the transition of both the workforce as well as the pending flood of baby boomers entering into the care space.
However, as seen in the job cut announcements and recent quarterly earnings for hospital operators, providers are facing challenges that are affecting their bottom lines.
One of the biggest challenges for providers is declining or flattening admissions. In 2010, all hospital admissions totaled 36.9 million admissions. By 2013, admissions had dropped by 1.5 million; 35 million patients were admitted in 2015.
In the latest rounds of quarterly earnings, most for-profit hospital operators took a lashing, all acknowledging softening markets and weaker-than-expected patient volumes. Community Health Systems (CHS) reported it underperformed in Q2 2017 and is exploring more divestitures while HCA Healthcare reported it missed Q2 estimates due in part to higher expenses and lower-than-expected patient admissions. On Monday, Tenet Health reported a 4.5% decline in total admissions for the first six months of 2017.
Indiana University Health’s operating income suffered a 46% loss while seeing less individuals coming into the facilities, Modern Healthcare reported.
As seen in HCA Healthcare’s Q2 earnings call, lower acuity visits declined in the last quarter. At CHS, emergency department volume declined on the outpatient side, which Tim Hingtgen, president and COO of CHS, attributed to “industry dynamics, including urgent care growth, freestanding ED competition in select markets.” As Turner notes, the average person seeking a care setting visit is likely going to a physician’s office. This puts pressure on operators to rethink their lower acuity setting strategies and not rest on the strength of organic patient growth seen in previous years.
Another major issue for providers are expenses. More jobs equals more expenses, for example. Facility maintenance, equipment, electricity, telephone lines, internet, etc. all add up. According to the American Hospital Association, expenses for all U.S. registered hospitals are currently $936 billion, up from $859.4 billion in 2013. In addition to these changes, turning toward value-based care exposes providers more to risk-based contracts which can affect reimbursement formulas.
Ben Isgur, director of PricewaterhouseCoopers’ Health Research Institute, adds that squeezing costs isn’t a new concept for hospitals. There are many options for executives to manage out costs from its overhead. Supply chain, infrastructure and third party contracts are all go-to areas for such efforts. If two systems merge, departments can be streamlined or share services. In some cases, third-party contractors may be more beneficial to a provider than hiring for internal positions.
Igor Belokrinitsky, healthcare strategist at Strategy&, a member of the PwC network of firms, told Healthcare Dive in March many administrators faced with financial challenges tell their departments during the budgeting process to budget for zero cost increases or even for a reduction. “In the longer run, we are seeing and are working with health systems to take out pretty significant amounts of cost out of their operations, both clinical and nonclinical, and setting targets like 15-20%, which is a transformative change,” he said. “When talking about a 20% cost improvement, you’re questioning, ‘Do we need this facility? Do we need to provide this service at this location? Does this service need to be provided by a physician?'”
Isgur tells Healthcare Dive that healthcare industry layoffs should be watched closely and agrees with Turner that one of the biggest reasons is uncertainty in the industry.
As an example, he points to the Congressional Budget Office’s figure that 15 million individuals could have lost health coverage in 2018 if the Senate ACA repeal bill had become law. “Providers look at that and have to be ready for an environment where they have potentially fewer paying patients,” Isgur told Healthcare Dive.
During the heady time when ACA repeal-and/or-replace was on Congress’ plate this summer, many projections showed healthcare jobs would’ve been affected. One analysis of the House ACA bill estimated 725,000 jobs across the entire industry would be lost by 2026 if it had become law. The primary cause of the job disappearances and state economic downturns would have been attributable to cuts to healthcare funding, such as more than $800 billion to Medicaid, and lower premium subsidies.
Moody’s Investor Services projected the Senate ACA repeal bill would have caused uncompensated care costs to rise at hospitals.
The fight over healthcare policy is likely now headed to the executive branch, as Congress has failed to pass a bill that repeals or replaces the ACA. President Donald Trump has cost-sharing reduction payments to insurers hanging in the balance, and hasn’t publicly stated if the White House will continue to make these payments.
If these payments are discontinued, Fitch Ratings found in a new report that premiums could increase to the point where customers won’t be able to pay for coverage, thus increasing the chance for uncompensated payments to rise.
In addition, state Medicaid waivers will have to be looked at. Some applications, such as the Maine’s, could include work requirements, mandatory premiums and asset testing. It would be one of the most conservative state programs, and some health policy experts warn that the restrictions would push out many low-income adults who would otherwise qualify.
“When you add uncertainty to what’s already been going on in the reimbursement environment around how many more uninsured there may be going forward, that’s not the cause of [layoffs] but it’s certainly going to accelerate the thinking of executive teams to make sure [their organizations] are efficient and ready for anything,” Isgur said.
Isgur does think the industry will see more layoff announcements this year, but that it is an important trend to watch, especially as more decisions come out of Washington.
https://www.axios.com/the-collapse-of-community-health-systems-2471839258.html
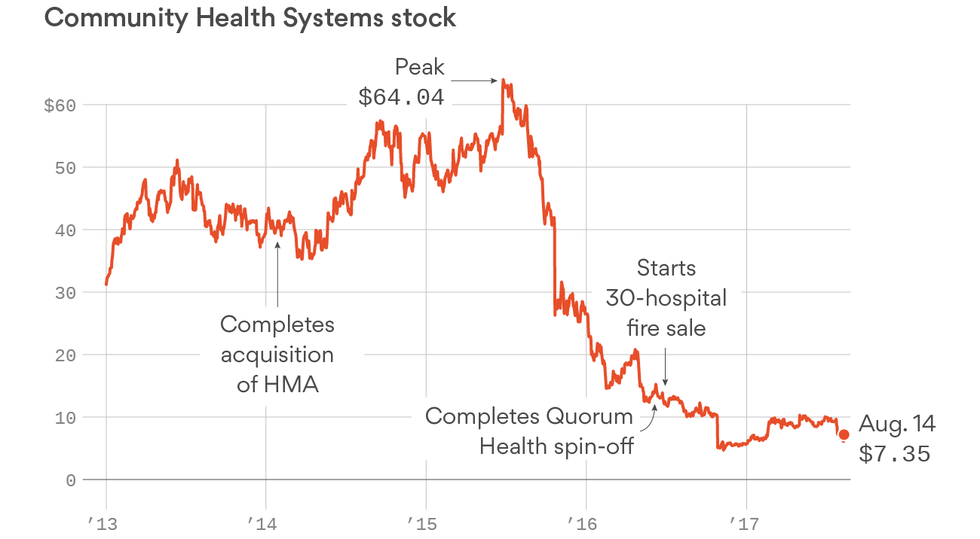
Just three years ago, Community Health Systems was the largest for-profit operator of hospitals with more than 200 facilities scattered in rural and suburban areas with growing populations. Now, the company is hemorrhaging money, sitting atop a mountain of debt and teetering on the edge of bankruptcy — all major reasons why CHS has lost almost 90% of its market value.
“I think the company has a nontrivial chance of defaulting,” said one CHS investor who asked to be unnamed because of the sensitivity of the issue. Tomi Galin, a CHS spokeswoman, did not make any company officials available for an interview, but said the company is confident it will have “a stronger core group of hospitals that are better positioned for long-term growth.”
Why it matters: CHS sits in a massive hole after a string of missteps, according to industry insiders. And it’s not likely to get better for CHS, or the local communities that rely on a CHS facility, as more people get treated in lower-cost outpatient centers instead of the hospital.
The collapse: It began in 2013 and continued into January 2014. That’s when CHS completed its acquisition of Health Management Associates, a for-profit hospital chain that had a slew of financial and legal problems. The deal was worth $7.6 billion, including debt, and made CHS the largest for-profit hospital company by number of facilities.
“That was the death knell,” a health care investment banker said. “HMA was a troubled company, and (CHS) thought bigger would be better.”
Here’s what has happened at CHS since then:
Looking ahead: CHS plans on divesting even more hospitals, executives said during their latest earnings call. They likely will be profitable hospitals, as buyers won’t touch money-losing inpatient facilities with dwindling admissions.
But large debt payments are due in 2019 through 2022. Short-term cash from transactions appears to be a bandage, and a subsequently smaller profit base won’t solve the big debt picture, making bankruptcy a real possibility, an investor said.
Galin, the CHS spokeswoman, said the money from the hospital sales “are being used to reduce our debt” and that “cash flow generation remains strong.”
Leadership questions: Many CHS executives have retired or left in the past two years, including longtime CFO Larry Cash. Wayne Smith, the CEO of the hospital chain since 1997, remains in his position. Smith is one of the highest earners among hospital executives and reaped more than $1 million in bonuses alone the past two years even though CHS’ stock price tanked.
Numerous sources would not go on the record to talk about CHS. One hospital industry analyst said this when asked how Smith still had his job despite the company’s problems: “Your question is very valid.”

Whether lawmakers are done with efforts to repeal the ACA or not, some important changes for healthcare could be on the horizon.
At least one part of the healthcare industry is still looking to Washington D.C. after the flurry of activity last month, if only for one action. In addition to the highly public failure to pass major healthcare legislation before leaving town for a month, Congress and President Donald Trump also left the Affordable Care Act (ACA) exchange markets in a dangerous flux by not taking action on the cost-sharing reduction (CSR) payments for insurers.
It’s not clear whether Congress will continue to take up Republican healthcare legislation to repeal the ACA when it returns. Even within the party, senators are singing different tunes, while President Donald Trump continues to pressure lawmakers to get an ACA repeal bill on his desk. A bipartisan group with members from both chambers has a few ideas, but the majority of lawmakers appear ready to move on. Regardless, they will still have to take up reauthorization of the Children’s Health Insurance Program (CHIP) in September, potential reigniting some debates around the ACA.
If GOP leaders do declare ACA repeal off the table for this year, its opponents will look to the executive branch for efforts to weaken the law and its effects. Here’s what to look out for.
Payers have been begging for assurance that CSRs will continue to be paid, but the White House and Congress have so far refused. The result has been many payers pulling out of the exchange markets or reducing their footprints, as well as premium hikes of 30% or more. Just last week, Anthem announced it is pulling out of the Nevada and Virginia exchange markets and reducing its participation in Georgia.
Not paying the CSRs would increase federal spending, because the higher premiums will require higher premium subsidies for the 84% in the exchanges who qualify for help. That’s not to mention the 30,000 or more who would have no insurance options.
Trump hasn’t been shy about his plan to halt any efforts that stabilize the exchange markets (like CSRs) in an effort to sabotage the ACA and force unwilling Democrats to cooperate on a repeal bill. Others in the GOP, however, have been reluctant to hurt constituents with such an overtly political play.
America’s Health Insurance Plans has said it is imperative the CSRs are funded. “These benefits are essential to making coverage and care affordable for American families who receive them,” the organization said. “Clarity and commitment to this funding is needed to eliminate confusion and anxiety for consumers.”
It may soon be too late for CSR payments to matter for next year. Payers must sign their contracts with HealthCare.gov by Sept. 21. The CMS and some states have tried to give insurers more flexibility because of the uncertainty by pushing back rate filing deadlines. Connecticut said it will allow payers to refile their rates if the CSR payments are eliminated, and California allowed them to file two sets of rates, one of which assumes no CSRs.
Trump’s threat to “let Obamacare implode” may go beyond refusing to shore up the exchange markets. His administration has already pulled advertising and promotion of the exchanges, and is being investigated by the Government Accountability Office for pushing the GOP healthcare bills in official HHS communication channels. Immediately after his inauguration, Trump signed a wide-ranging executive order instructing federal agencies to “exercise all authority and discretion available to them to waive, defer, grant exemptions from, or delay any provision or requirement” of the ACA that imposes a fiscal or regulatory burden.
No major changes have resulted from the order so far, but it could be used to roll back benefit requirements for preventive care, contraception and mental health services.
HHS Secretary Tom Price could also make changes that weaken the ACA’s individual mandate. Repealing the mandate would mean 15 million fewer Americans would have coverage by 2026 and result in premium increases of about 20%, according to the Congressional Budget Office. Watering down the requirement instead of ditching it completely would have less drastic results, but there would still be an impact.
Price could create more exemptions for the mandate or attempt to force the Internal Revenue Service to stop enforcing it. Either of these actions would add turmoil to the exchanges markets and undermine the efforts of the ACA.
Those watching health legislation in Congress are eyeing CHIP reauthorization as a possible vehicle for changes to the ACA. Lawmakers will be hesitant, though, as CHIP is a successful program with bipartisan support.
The program, which turned 20 years old this past weekend, covered nearly 9 million children in fiscal 2016. CHIP coverage is more affordable than employer-sponsored or marketplace coverage, while children covered under CHIP are more likely to have a usual source of care and regularly attend well-child visits, according to the Medicaid and CHIP Payment and Access Commission, which recommends Congress extend CHIP funding through 2022.
The commission estimates more than a million children would lose coverage if CHIP loses funding.
A bipartisan group of about 40 members of the House is proposing some relatively small changes to the ACA that have received support from both sides of the aisle in the past. The plan is to put them in a bill that would also immediately fund the CSRs.
Their suggestions include exempting smaller businesses from the employer mandate, a fund states can go to for help covering people with high care costs and more flexibility and guidance for states looking to apply for ACA waivers. Another possible measure is repeal of the medical device tax.
Their proposal is to change the employer mandate by having it apply only to businesses with 500 or more employees, instead of the current requirement for businesses with 50 or more workers. Analysis from the Urban Instituteand Rand Corporation has shown the employer mandate has little effect on the number of people who have coverage, partly because nearly all businesses with at least 50 employees offered coverage even before the mandate went into effect.
The ACA has always given states the option of applying for a waiver that allows them to eschew essential health benefits and other requirements — as long as they can prove their plans will cover the same number of people with coverage that is just as comprehensive and affordable. HHS under President Barack Obama was careful in ensuring that state proposals met those guidelines, but current HHS Secretary Tom Price has said he wants to encourage more waivers and will be less strict with approvals of those waivers and Medicaid demonstration waivers.
With this in mind, some recent proposals have included aspects that would have previously been rejected. Last week, Maine applied for a Medicaid demonstration waiver that includes work requirements and asset testing. Those measures are likely to restrict access to coverage for people with low incomes.
Many of the options available for Congress and the executive branch could roil the industry, but some bipartisan options could provide much needed clarity. Summer is usually pretty quiet in Washington D.C., but this year has not been business as usual. Healthcare leaders would be wise to be ready for new developments with the ACA and beyond.

hen officials at Tufts Medical Center in Boston refused to allow nurses just off of a one-day strike return to their jobs, the footage spread across TV news programs and social media. Boston Mayor Martin Walsh, a former labor leader, spoke in favor of the striking nurses and the hospital found itself in an uncomfortable spotlight.
About 1,200 nurses went on a one-day strike after their union, the Massachusetts Nurses Association, and Tufts couldn’t come to a new contract agreement after more than a year of negotiations. Tufts, in turn, locked out the nurses when they attempted to return to work the next day.
Officials said the lockout was required because they needed to give at least five-day contracts to 320 temporary nurses brought in to fill the gap. The nurses are back on the job now without a new contract, but the strike and subsequent lockout got the public’s attention.
Hospital strikes aren’t that common — usually, the sides agree to a new contract. Strikes or threatened strikes in recent years have typically involved conflicts over pay, benefits and staff workloads.
When strikes do happen, however, they can hurt a hospital’s reputation, finances and patient care.
A study on nurses’ strikes in New York found that labor actions have a temporary negative effect on a hospital’s patient safety.
Study authors Jonathan Gruber and Samuel A. Kleiner found that nurses’ strikes increased in-patient mortality by 18.3% and 30-day readmission by 5.7% for patients admitted during the strike. Patients admitted during a strike got a lower quality of care, they wrote.
“We show that this deterioration in outcomes occurs only for those patients admitted during a strike, and not for those admitted to the same hospitals before or after a strike. And we find that these changes in outcomes are not associated with any meaningful change in the composition of, or the treatment intensity for, patients admitted during a strike,” they said.
They said a possible reason for the lower quality is fewer major procedures performed during a strike, which could lead partially to diminished outcomes. The study authors found that patients that need the most nursing care are the ones who make out worst during strikes.
“We find that patients with particularly nursing-intensive conditions are more susceptible to these strike effects, and that hospitals hiring replacement workers perform no better during these strikes than those that do not hire substitute employees,” they wrote.
Allina Health’s Abbott Northwestern Hospital in Minneapolis faced a patient safety issue during a strike last year that resulted in the CMS placing the hospital in “immediate jeopardy” status after a medication error. A replacement nurse administered adrenaline to an asthmatic patient through an IV rather than into the patient’s muscle. The patient, who was in the emergency room (ER), wound up in intensive care for three days because of the error. Allina said the error was not the nurse’s fault, but was the result of a communication problem.
The CMS accepted the hospital plan of correction, which included having a nurse observer when needed and retraining ER staff to repeat back verbal orders.
Hospitals also take a financial hit during strikes. Even the threat of a one- or two-day nurse strike can cost a hospital millions.
Bringing in hundreds or thousands of temporary nurses from across the country is costly for hospitals. They need to advertise the positions, pay for travel and often give bonuses to lure temporary nurses.
The most expensive recent nurse strike was when about 4,800 nurses went on strike at Allina Health in Minnesota two times last year. The two strikes of seven days and 41 days cost the health system $104 million. The hospital also saw a $67.74 million operating loss during the quarter of those strikes.
To find temporary replacements, Allina needed to include enticing offers, such as free travel and a $400 bonus to temporary nurses.
Even the threat of a strike can cost millions. Brigham and Women’s Hospital in Boston spent more than $8 million and lost $16 million in revenuepreparing for a strike in 2016. The 3,300-nurse union threatened to walk out for a day and much like Tufts Medical Center, Brigham & Women’s said the hospital would lock out nurses for four additional days if nurses took action.
At that time, Dr. Ron Walls, executive vice president and chief operating officer at Brigham and Women’s Hospital, said the hospital spent more than $5 million on contracting with the U.S. Nursing Corp. to bring on 700 temporary nurses licensed in Massachusetts. The hospital also planned to cut capacity to 60% during the possible strike and moved hundreds of patients to other hospitals. They also canceled procedures and appointments in preparation of a strike.
The Massachusetts Nurses Association and Brigham & Women’s were able to reach a three-year agreement before a strike, but the damage was already done to the hospital’s finances.
Richard L. Gundling, senior vice president of healthcare financial practices at Healthcare Financial Management Association, told Healthcare Dive that healthcare organizations need to plan for business continuity in case of an event, such as a labor strike, natural disaster or cyberattack.
“Business continuity is directly related to the CFO’s responsibility for maintaining business functions. The plan should include having business continuity insurance in place to replace the loss associated with diminished revenue and increased expenses during the event,” Gundling said.
These plans should provide adequate staffing, training, materials, supplies, equipment and communications in case of a strike. Hospitals should also keep payers, financial agencies and other important stakeholders informed of potential issues.
“It’s also key to keep financial stakeholders well informed; this includes insurance companies, bond rating agencies, banks, other investors, suppliers and Medicare/Medicaid contractors,” he said.
“Business continuity is directly related to the CFO’s responsibility for maintaining business functions. The plan should include having business continuity insurance in place to replace the loss associated with diminished revenue and increased expenses during the event.”
Richard Gundling
Senior vice president of healthcare financial practices, Healthcare Financial Management Association
Hospital strikes, particularly nurses’ strikes, can also wreak havoc on a hospital’s reputation. Nurses are a beloved profession. They work hard, often long hours and don’t make a fortune doing it. The median registered nurses’ salary is about $70,000, according to the Bureau of Labor Statistics.
Nurses’ contract disputes involving staffing levels are a sticky situation for hospitals. Nurses will almost always win the PR battle against hospital executives.
If a hospital can’t avoid a strike, Seitel said two keys for the organization are telling the truth and not being passive about untrue statements from the other side. They don’t want to be adversarial and escalate the situation, but go with a more measured approach.
Fraser Seitel, president of Emerald Partners, a communications management consulting company, told Healthcare Dive there are two ways that hospital leadership can avoid a strike.
“The best way to prevent a strike is by the management of the hospital having a robust communications program with the staff of the hospital as well as keeping competitive in terms of salaries and benefits,” said Seitel, who has helped hospitals during times of labor strife.
Seitel said labor issues often crop up when management isn’t communicative. Communication, transparency and competitive compensation are the best preventative medicine for a strike, he said.
http://www.healthcaredive.com/news/upmc-moves-ahead-on-purchase-of-pinnaclehealth/449305/

The deal, first announced in March, is UPMC’s largest ever and the first to involve an entire health system. Previous purchases have involved single hospitals, the most recent being Sunbury Community Hospital and Lock Haven Hospital from Quorum Health. Those hospitals will become part of Williamsport, Pa.-based UPMC Susquehanna, which was added to the UPMC system last fall.
With Pinnacle’s acquisition now on track, UPMC also stands to boost its health insurance product line, which accounted for close to half of its 2016 operating revenue. The move will pit UPMC Health Plan against Capital BlueCross and Highmark, which together have 75% of the central Pennsylvania market. Aetna holds the rest.
Gaining a foothold in the Harrisburg region could help to compete with Highmark, which four years ago bought Pittsburgh-based Allegheny Health Network, putting it in direct competition with UPMC’s medical and coverage operations.
Merger and acquisition activity has kept up a steady pace this year, with no signs of abating. Reasons for deals include declining admissions, rising costs and a desire to expand into new regions or service lines.
In May, Cleveland Clinic and Dover, Ohio-based Union Hospital signed a letter of intent to merge Union into Cleveland Clinic. The move will expand Cleveland Clinic’s footprint into southern Ohio, while bringing new services and resources to Union, officials said at the time.
Cleveland Clinic CEO Toby Cosgrove, who is stepping down later this year, said in April that consolidation and a greater focus on telemedicine would help providers transition from volume to value payment as healthcare reform continues to evolve.
UPMC expects to complete the acquisition September 1, pending regulatory approvals. For the fiscal year ended June 30, 2016, Pinnacle reported revenue of $1.05 billion.


What you believe about yourself, others, and events governs your attitudes and behaviors.
Limiting beliefs produce limited results.
3 prevailing beliefs that limit leadership:
#1. Leaders are tough.
Leaders do tough things. Successful leaders do tough things with openness, kindness, and empathy. Navigating tensions between doing tough things with a kind heart is one of the greatest accomplishments on the leader’s journey.
The soft side of toughness:
- Openness: Open leaders listen, seek input, and ask questions.
- Kindness: Kind leaders make it easier for others to achieve great results.
- Empathy – Empathetic leaders know how to take the perspective of others.
Openness, kindness, and empathy are expressions of curiosity.
#2. Leaders tell people what to do.
When the house is on fire, command and control is appropriate. But command and control as a daily practice limits potential and marginalizes the talent.
One of the toughest transitions of leadership is the transformation from giving solutions to asking questions. Early in your career you earned promotions by providing solutions. But the leader’s job is building relationships and creating environments where others provide solutions.
#3. Leaders get things done.
The thing leaders really do is help others get things done.
In many organizations you are both leader and doer. You don’t have the luxury of focusing exclusively on the performance of others. For example, you implement the new initiative and you lead the team to implement the new initiative. You have to execute and help others execute.
Shifting hats from doer to leader means facing the challenge of stepping back so others can step in.
3 tips:
- Ask open questions in meetings.
- Pat people on the back. Do this literally and frequently.
- Remember that the orchestra makes the music. The conductor doesn’t make a sound. (Thanks to Ben Zander for this insight.)
What prevailing beliefs limit leadership?
How might leaders overcome limiting beliefs?
