Cartoon – We are not a Not-for-Profit Organization
Rep. Pramila Jayapal (D-Wash.) is seeking buy-in from more fellow Democrats for a sweeping Medicare-for-all bill she is poised to release near the end of the month.
It’s a proposal that has become a rallying cry for progressives and 2020 presidential candidates, but it is also exposing deep rifts in the Democratic Party over exactly how to achieve universal health coverage in the United States.
The Medicare for All Act of 2019, which Jayapal had planned to roll out this week but delayed because she was seeking more co-sponsors, would create a government-run single-payer health system even more generous than the current Medicare program. Her office hasn’t publicly released the details of the upcoming measure, but Democratic members told me it would cover long-term care and mental health services, two areas where Medicare coverage is sparse.
The bill also proposes to add dental, vision, prescription drugs, women’s reproductive health services, maternity and newborn care coverage to plans that would be available to people of all ages and would require no out-of-pocket costs for any services, according to a letter Jayapal sent to colleagues on Tuesday asking them to consider co-sponsoring the effort.
“Medicare for All is the solution our country needs,” the letter said. “Patients, nurses, doctors, working families, people with disabilities and others have been telling us this for years, and it’s time that Congress listens.”
The 150-page bill had 93 co-sponsors as of Tuesday, although Jayapal spokesman Vedant Patel said more Democrats have signed on since then. That’s still fewer than the 124 Democrats who co-sponsored a much less detailed Medicare-for-all proposal from then-Rep. John Conyers (D-Mich.) last year. A strategist who has been working with Democrats on health-care ideas told me there have been some frustrations that more members haven’t yet signed on to Jayapal’s bill, despite the fact that there are 40 more Democrats in the House this year.
But Jayapal said she’s confident she’ll have 100 co-sponsors by the time of the bill’s planned Feb. 26 release, explaining she’s not surprised members would take more time to consider it given its length.
“It’s a 150-page bill … it’s not an eight-page resolution,” Jayapal told me yesterday. “Now we’re actually putting detail into it, and so we feel confident we will continue to add cosponsors even after introduction.”
Patel also noted it’s still early in the year, saying he “disagrees” with the notion that it’s taking a long time to bring Democrats on board.
“It’s the second week of February and we are at more than 95 co-sponsors,” he said. “Coalition building is a process, but we are on track to introduce this historic legislation with resounding support at the end of the month.”
Yet differences are emerging among Capitol Hill Democrats over how to expand coverage, part of a larger debate roiling the party as 2020 candidates, many of them senators, and a new class of freshmen House Democrats move the party left not only on health care but also on the environment.
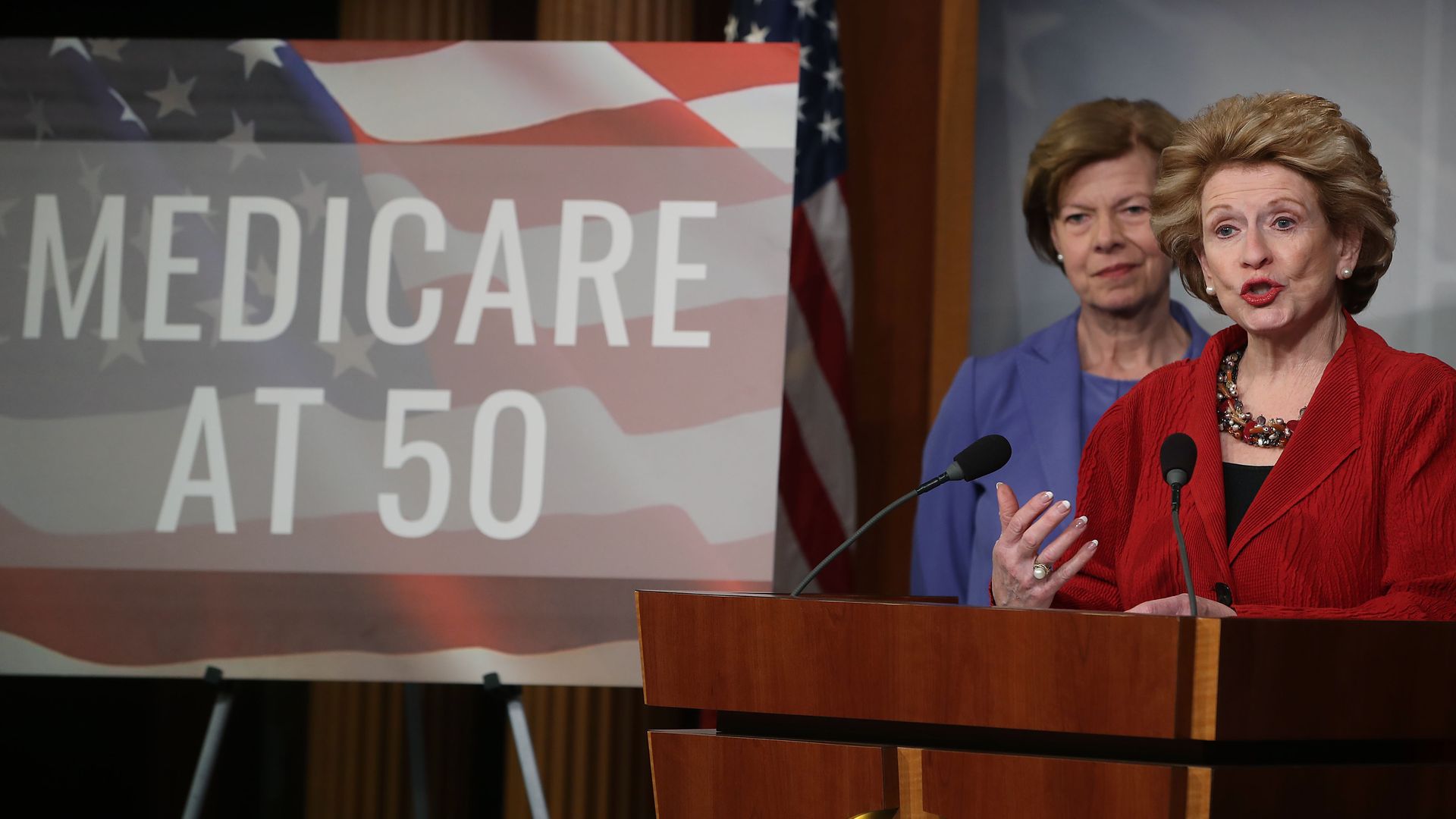
The cracks were especially apparent yesterday, as a separate group of lawmakers gathered to re-introduce their own proposal to allow people to buy in to Medicare starting at age 50. That measure, offered by Sen. Debbie Stabenow (D-Mich.) and Rep. Brian Higgins (D-N.Y.), would take a more incremental approach to expanding health coverage — one that could play better with voters who would stand to lose private coverage under a single-payer program.
Their bill, dubbed the “Medicare at 50 Act,” would allow people to buy Medicare plans instead of purchasing private coverage on the Obamacare marketplaces if they are uninsured or prefer it to coverage offered in their workplace.
And today, Sen. Brian Schatz (D-Hawaii) and Rep. Ben Ray Luján (D-N.M.) are reintroducing their State Public Option Act, which allows people to buy a Medicaid plan regardless of their income. That measure has broad backing from not just lawmakers (20 senators co-sponsored it last year) but also well-known health policy wonks including former Centers for Medicare and Medicaid Services Administrator Andy Slavitt.
Higgins is one of several Democrats on the House Budget Committee who have proposed a total of three separate and contrasting bills to expand Medicare to more people. The others are Reps. Rosa DeLauro (D-Conn.) and Jan Schakowsky (D-Ill.), who have a bill to expand Medicare to all ages while still preserving employer-sponsored coverage, and Jayapal.
Once Jayapal rolls out her legislation, the Congressional Budget Office is expected to release an analysis of how much it would cost by the end of March or the beginning of April, Budget Committee Chairman John Yarmuth (D-Ky.) told me. At that point, the committee will hold a hearing with the CBO to go over the cost and its potential impact on the federal budget.
That’s where Jayapal could run into roadblocks.Given the extensive benefits she’s proposing, her bill would probably come at a steep cost to taxpayers — and paying for things is almost always Congress’s trickiest task. Of course, supporters of the legislation stress its benefits would fill in much-needed gaps in coverage under the current Medicare program.
“The biggest change I give her so much credit for is it has long-term care,” said Rep. Ro Khanna (D-Calif.), who is a co-sponsor of Jayapal’s Medicare-for-all bill. “This is huge.”
And then there’s also the question of how voters might react if told they would lose their current coverage. Sen. Kamala Harris (D-Calif.), who has gone the furthest of all the 2020 candidates in pushing for an overhaul of the U.S. health-care system, attracted widespread attention recently when she suggested she’d be fine with entirely eliminating private coverage in favor of government-run plans.
“We’re very aware that there is anxiety about — however imperfect — a system you know and doctors you know, and that is going to be all part of the hearing process, public input into: How do we build a system in this country that really cares about all Americans?” said Rep. Katherine Clark (D-Mass.), another co-sponsor of the Jayapal bill.

Congressional Democrats have quickly lined up to oppose the Trump Administration’s proposal to eliminate regulations that make it illegal for drug companies to reduce – or eliminate – what Medicare consumers pay for prescriptions under the Part D program.
Instead, they are pushing plans to give health insurers and the pharmacy benefit management (PBM) companies they run and own even more control over what medicine consumers can choose and how much they cost. In doing so, Democrats are backing a government-sanctioned drug pricing cartel that extorts nearly a quarter of trillion dollars a year from prescription drug rebates, discounts, and patients (in the form of out-of-pocket costs), and shares a pittance with the patients who need medicines the most. Eighty percent of drug benefits are managed by the 3 largest PBMs, which in turn are owned by or in part by the 3 largest insurance companies.
Current Medicare regulations makes it illegal for any firm other than PBMs to handle drug prices and distribution. Specifically, PBMs are given free rein to determine what medicines patients can and can’t use. This power allows them to reduce the list price of drugs by obtaining rebates in exchange for encouraging the use of some treatments while discouraging the use of other medicines. PBMs either require patients to try drugs that generate the most rebates first or force people to pay part or all of the list price of medicines that don’t generate much money.
As a result, of $140 billion Medicare Part D spent on medicines, $64 billion was pocketed by PBMs and health plans. And of the $460 billion all Americans spent on drugs in 2018 nearly $166 billion went to discounts and rebates.
Parroting the PBM/insurer talking points, Nancy Pelosi’s health policy advisor, Wendell Primus, said prices – not rebates – are the cause of high drug costs, and savings from rebates negotiated by pharmacy benefit managers go toward reducing insurance premiums.
In fact, PBMs keep Part D premiums artificially low by collecting rebates and other fees at the retail counter. Because Medicare starts paying for 80 percent of drug costs after seniors shell out over $4500 at the pharmacy, plumping up the retail price with rebates means PBMs and insurers reduce premiums by shifting more cost to the government and ultimately by forcing seniors to pay more for medicines.
Moreover, PBMs are using rebates extracted from the medicines the most seriously ill patient uses to subsidize the drug spending and premiums of everyone else. People with cancer, HIV, Parkinson’s, autoimmune diseases are only 2 percent of the population. But in 2017 the drugs they use generated $53 billion, or 32 percent of all rebates and discounts.
These rebates could be used to reduce out-of-pocket costs of even the most expensive drugs to 50 dollars or less. Instead PBMs and plans actually make seniors pay a large percentage of the retail cost of the rebated drugs In fact, as rebates have increased, plans have made more consumers of these so-called specialty drugs to pay up to 50 percent of the retail price of medicines instead of a small copay. Nearly 25 percent of all consumers now pay full price for drugs. As an IQVIA report found: “people who use specialty medicines are 10 times more likely to pay full price for the most expensive medicine. On average, they are 10 times more likely to pay over $2500.”
In 2017, 2 percent of the most vulnerable consumers paid PBMs and health plans $16 billion in out-of-pocket costs. Soaking the sick to make the rich even richer. The quickest way to cut the cost of medicines to what they are in Europe is to eliminate the PBM protection racket and give drug companies the freedom to dramatically reduce the out-of-pocket cost for the most expensive medicines. To be sure, a growing number of drug firms and insurers are working together to eliminate out-of-pocket costs as part of programs to improve health by reducing barriers to access. Indeed, because PhRMA and BIO have stated that consumers should pay less, the Trump proposal is truly a ‘put up or shut up’ moment for the industry.
Under the current rules, it doesn’t pay for PBMs and insurers to choose a drug with lower out-of-pocket costs, and drug companies have no incentive to tie out-of-pocket costs to better care. Under current rules, patients are unable to afford the medicines that keep them alive. The Trump proposal would change all that. It’s up to Democrats to explain why, instead of cutting drug costs dramatically and directly, they want to line the pockets of big corporations with money from the sickest patients.
Insurers and hospitals came out swinging yesterday against Democrats’ proposal to let people older than 50 buy into Medicare — a reminder that almost any expansion of public health coverage will provoke a battle with the health care industry.
Between the lines: Politically, an age-restricted Medicare buy-in is about as moderate as it gets for Democrats in the age of “Medicare for All.”
Yes, but: Being on the more moderate end of the political spectrum does not shield you from a fight.
The bottom line: Any proposal that would compete with (never mind eliminate) private coverage, particularly employer coverage, will meet this kind of resistance.
That’s why Medicaid is the public program Democrats and industry can agree to love. Expanded access to Medicaid has rarely been an alternative to commercial insurance — it’s usually an alternative to being uninsured.

Abstract: This article looks into the importance of selling in business and the relevance of the development of selling skills to career success regardless of your role in an organization.
Really? You’re not a salesman or saleswoman or salesperson? What are you then? Zig Ziglar and others argue that everyone is in selling whether he or she recognize or acknowledge it or not. I have come across people that say that they consciously and intentionally do not know anything about selling or that selling is below their station in life. Some of them have no idea that some of the best-compensated people in society achieve the success they enjoy from being successful in sales.
What is selling anyway? I would define selling as bringing someone else around to your way of thinking. The hoped result of the selling process is that the other party will decide to act upon your suggestions and recommendations (closing questions). Sometimes this results in a sale for value in which goods or services are exchanged. In other cases, you are selling a concept or ideas like a strategy or recommended course of action to a decision maker that must put their reputation and possibly their job on the line by committing to your proposed course of action.
When some people hear the term ‘salesman’ the image that pops up in their mind is the high-pressure wielding scoundrel at the ‘buy here, pay here, Se Habla Español’ used car dealership with the moussed hair, polyester leisure suit, braided leather suspenders, and patent leather platform shoes. The sales weasel is the offensive stereotype that ‘professionals’ avoid at all costs. However, the argument can be made that the scoundrel has a much easier way of making a living than those of us that make our living by selling ideas, concepts, and strategies into sophisticated organizations. He is not up against counterparties that in many cases are considerably more experienced, educated, credentialed or intelligent than he is. More often than not, the reverse is true.
If you would just as soon not be bothered with selling, my suggestion is that you dispense with aspirations of obtaining or staying in a C-Suite role. What is a C-Suite? One definition is that it is a marketplace of ideas. The environment is characterized by continuous, ongoing debate of concepts and strategies to move the organization forward or respond to problems and threats. If you are not effective in getting your ideas heard, debated and accepted, you might want to start thinking about finding another way to make a living. If you cannot successfully sell your fair share of ideas in what is usually a very intimidating, competitive and sometimes hostile environment, your perceived value will fall along with the probability of achieving your career ambitions.
What types of selling occur? Direct selling involves interactions with the intended purpose of an agreement to exchange goods or services for money. What I will refer to as professional selling is focused on winning in the marketplace of ideas. In other words, getting decision-makers to take your advice, respond to your counsel or choose a course of action based primarily upon your input. Professional selling is infinitely more difficult because it has a variable that is usually not present in direct selling – politics. The politics are carried out generally behind the scenes by competitors of yours that could be trusted co-workers that advocate for their ideas behind the scenes or behind your back, without giving you the courtesy or respect of a face-to-face argument. They use whatever leverage is available to them behind the scenes, under the table, and behind your back to advance their causes, frequently resulting in decisions that do not make rational sense. Suboptimal results occur because, in the presence of politics, decision making is usually irrational.
For example, I experienced a situation where some physicians were not happy with some of the decisions coming out of the boardroom and the front office. Do you know how many visits I had from any of the doctors? The answer is zero! Instead, they took their grievances directly to members of the board or county commission that humored and engaged them possibly in utter and absolute ignorance of the degree to which this amounted to the active undermining of the leadership team of the organization. I learned that one board member was accosted in the church vestibule and never made it into the sanctuary to join their family for the service. Others are caught at their places of work or during unrelated social events. As we are seeing in our society right now, people that are sufficiently strident about their position will resort to extreme means including violence to have their ideology imposed upon the rest of us. If you are in a board meeting and something entirely unexpected comes out of left field and derails something that you have put a lot of time and energy into, there is a good chance you are a victim of cowardly, destructive politics.
The stakes of success in a political environment are exponentially higher. If you are to be successful when you are up against political resistance, your arguments or the effectiveness of your selling must be sufficiently compelling to not only overcome the logical burden of your case but the political forces that may be working against you behind the scenes or maybe more accurately stated, behind your back. If this is not selling, I don’t know what is. Most of the time, to one degree or another, your career is potentially on the line when you are selling to your leader or a board of trustees. Must close selling puts you in an Apollo 13 situation where failure is not an option. I sold vacuum cleaners in college. I learned these concepts early on. In-home vacuum selling can be very intense, high-pressure selling. That said, selling vacuum cleaners is infinitely more comfortable than surviving in the shark tank that is the C-Suite of most organizations I have experienced. I guess that’s why good vacuum cleaner salesmen make around $50K and C-Suite roles pay into seven figures.
So, the obvious question is what you should be doing? My recommendation is that you start dedicating significant time and energy to learning as much as you can about selling. The quintessential sales trainer is Zig Ziglar. He is one of the best but not the only one. I would also recommend Harvey Mackay. Both of these guys are retired, but their work is as relevant as ever. Effective selling requires a healthy positive attitude. There are many excellent motivational speakers. Some of my favorites are Les Brown, Earl Nightingale, Dr. Angela Duckworth, Zig Ziglar, and Ed Foreman. Don’t overlook some of the incredible ministers that deliver messages of hope and inspiration. For starters, I recommend Charles Stanley, Johnny Hunt, Robert Schuller, and Joel Osteen. I have found that the more time I spend listening to these inspiring people, the luckier I become in the marketplace of ideas in a consulting firm, among my compadres, in a hospital C-Suite or down at the local watering hole.
Contact me to discuss any questions or observations you might have about these articles, leadership, transitions or interim services. I might have an idea or two that might be valuable to you. An observation from my experience is that we need better leadership at every level in organizations. Some of my feedback is coming from people that are demonstrating an interest in advancing their careers, and I am writing content to address those inquiries.
The easiest way to keep abreast of this blog is to become a follower. You will be notified of all updates as they occur. To become a follower, click the “Following” bubble that usually appears near the bottom of each web page.
I encourage you to use the comment section at the bottom of each article to provide feedback and stimulate discussion. I welcome input and feedback that will help me to improve the quality and relevance of this work.
This blog is original work. I claim copyright of this material with reproduction prohibited without attribution. I note and provide links to supporting documentation for non-original material. If you choose to link any of my articles, I’d appreciate notification.

The clash over free trade in North America has long been fought over familiar issues: low-paid Mexican workers. U.S. factories that move jobs south of the border. Canada’s high taxes on imported milk and cheese.
But as Democrats in Congress consider whether to back a revamped regional trade pact being pushed by President Donald Trump, they’re zeroing in on a new point of conflict: drug prices. They contend that the new pact would force Americans to pay more for prescription drugs, and their argument has dimmed the outlook for one of Trump’s signature causes.
The president’s proposed replacement for the 25-year-old North American Free Trade Agreement is meant to win over Democrats by incentivizing factories to hire and expand in the United States. Yet the pact would also give pharmaceutical companies 10 years’ protection from cheaper competition in a category of ultra-expensive drugs called biologics, which are made from living cells.
Shielded from competition, critics warn, the drug companies could charge exorbitant prices for biologics.
“This is an outrageous giveaway to Big Pharma,” Rep. Rosa DeLauro, a Connecticut Democrat, said in an interview. “The government guarantees at least 10 years of market exclusivity for biologic medicine. It’s a monopoly. It’s bad policy.”
The objections of DeLauro and other Democrats suddenly carry greater potency. The need to curb high drug prices has become a rallying cry for voters of all political stripes. Trump himself has joined the outcry. The revamped North America trade deal must be approved by both chambers of Congress, and Democrats have just regained control of the House.
Rep. Earl Blumenauer of Oregon, the new chairman of the House Ways and Means subcommittee on trade, told The Associated Press that “I don’t think candidly that it passes out of my trade subcommittee” with the biologics provision intact.
“The biologics are some of the most expensive drugs on the planet,” Blumenauer said.
Still, the politics of NAFTA 2.0 are tricky for Democrats and not necessarily a sure-fire winner for them.
The original NAFTA, which took effect in 1994, tore down most trade barriers separating the United States, Canada and Mexico. Like Trump, many Democrats blamed NAFTA for encouraging American factories to abandon the United States to capitalize on lower-wage Mexican labor and then to ship goods back into the U.S., duty-free.
Having long vilified NAFTA, Trump demanded a new deal — one far more favorable to the United States and its workers. For more than a year, his top negotiator, Robert Lighthizer, held talks with Canada and Mexico. Lighthizer managed to insert into the new pact provisions designed to appeal to Democrats and their allies in organized labor. For example, 40 percent of cars would eventually have to be made in countries that pay autoworkers at least $16 an hour — that is, in the United States and Canada and not in Mexico — to qualify for duty-free treatment.
The new deal also requires Mexico to encourage independent unions that will bargain for higher wages and better working conditions.
Late last year, the three countries signed their revamped deal, the U.S.-Mexico-Canada Agreement. But it wouldn’t take effect until their three legislatures all approved it. In the meantime, the old NAFTA remains in place.
The question now is: Are Democrats prepared to support a deal that addresses some of their key objections to NAFTA and thereby hand Trump a political victory? Some Democrats have praised the new provisions that address auto wages, though many say they must be strengthened before they’d vote for the USMCA.
Protection for drug companies is another matter. Many Democrats had protested even when the Obama administration negotiated eight years of protection for biologics— from cheap-copycat competitors called “biosimilars” — in a 12-country Pacific Rim trade pact called the Trans-Pacific Partnership, or TPP.
Trump abandoned the TPP in his first week in office. But the pharmaceutical industry is a potent lobby in Washington, and Trump’s negotiators pressed for protection for U.S. biologics in the new North American free trade deal. They ended up granting the drug companies two additional years of protection in the pact.
Top biologics include the anti-inflammatory drug Humira, the cancer fighter Rituxan and Enbrel, which is used to treat rheumatoid arthritis.
The administration and drug companies argue that makers of biologics need time to profit from their creations before biosimilars sweep in, unburdened by the cost of researching and developing the drugs. Otherwise, they contend, the brand-name drug companies would have little incentive to invest in developing new medicines.
They note that a 2015 law authorizing presidents to negotiate trade deals requires American officials to push other countries toward U.S.-level protections for intellectual property such as biologic drugs. (The same law, somewhat contradictorily, directs U.S. negotiators to “promote access to medicines.”)
Supporters also note that existing U.S. law gives makers of biologics 12 years’ protection. So the new pact wouldn’t change the status quo in the United States, though it would force Mexico to expand biologics’ monopoly from five years and Canada from eight years. In fact, supporters of the biologics monopoly argue that the pact might cut prices in the United States because drug companies would no longer face pressure to charge Americans more to compensate for lower prices in Canada and Mexico.
But critics say that expanding biologics’ monopoly in a trade treaty would prevent the United States from ever scaling back the duration to, say, the seven years the Obama administration once proposed.
“By including 10 years in a treaty, we are locking ourselves in to a higher level of monopoly protection for drugs that are already taking in billions of dollars a year,” said Jeffrey Francer, general counsel for the Association for Accessible Medicines, which represents generic drug companies. “The only way for Congress to change it is to back out of the treaty. … Does the United States want to be in violation of its own treaty?”
For Democrats, higher drug prices are shaping up as a powerful political argument against approving the president’s new North American trade deal. In December, Stanley Greenberg, a leading Democratic pollster and strategist, conducted focus groups in Michigan and Wisconsin with Trump voters who weren’t affiliated with the Republican Party. Some had previously voted for Barack Obama. Others called themselves political independents. They’re the kinds of voters Democrats hope to attract in 2020.
Greenberg said he was “shocked” by the intensity of their hostility to drug companies — and to the idea that a trade pact would shield those companies from competition.
“It was like throwing a bomb into the focus group,” said Greenberg, who is married to DeLauro. He said the voters’ consensus view was essentially: “The president was supposed to go and renegotiate (NAFTA) so that it worked for American workers. But it must be that these lobbyists are working behind the scenes” to sneak in special-interest provisions.
That perception gives Democrats reason to reject the new pact as the 2020 election approaches.
“Democrats have no incentive to do this,” said Philip Levy, a senior fellow at the Chicago Council on Global Affairs and a White House economist under President George W. Bush. “Before you know it, the presidential election season is going to be upon us.”
U.S. trade rules are designed to force Congress to give trade agreements an up-or-down vote — no nitpicking allowed. Still, there are ways to bypass those restrictions. Congressional Democrats could, for example, push the administration to negotiate so-called side letters with Canada and Mexico to address their concerns. President Bill Clinton did this with the original NAFTA.
“Lighthizer and his team are very creative,” said Blumenauer, chair of the House trade subcommittee. “This is something that can be handled.”

What does health insurance coverage look like for Americans today, more than eight years after the Affordable Care Act’s passage? In this brief, we present findings from the Commonwealth Fund’s latest Biennial Health Insurance Survey to assess the extent and quality of coverage for U.S. working-age adults. Conducted since 2001, the survey uses three measures to gauge the adequacy of people’s coverage:
As the findings highlighted below show, the greatest deterioration in the quality and comprehensiveness of coverage has occurred among people in employer plans. More than half of Americans under age 65 — about 158 million people — get their health insurance through an employer, while about one-quarter either have a plan purchased through the individual insurance market or are enrolled in Medicaid.1Although the ACA has expanded and improved coverage options for people without access to a job-based health plan, the law largely left the employer market alone.2
The 2018 Commonwealth Fund Biennial Heath Insurance Survey included a nationally representative sample of 4,225 adults ages 19 to 64. SSRS conducted the telephone survey between June 27 and November 11, 2018.3 (See “How We Conducted This Study” for more detail.)
In this analysis, we use a measure of underinsurance that accounts for an insured adult’s reported out-of-pocket costs over the course of a year, not including insurance premiums, as well as his or her plan deductible. (The measure was first used in the Commonwealth Fund’s 2003 Biennial Health Insurance Survey.*) These actual expenditures and the potential risk of expenditures, as represented by the deductible, are then compared with household income. Specifically, we consider people who are insured all year to be underinsured if:
The out-of-pocket cost component of the measure is only triggered if a person uses his or her plan to obtain health care. The deductible component provides an indicator of the financial protection the plan offers and the risk of incurring costs before someone gets health care. The definition does not include other dimensions of someone’s health plan that might leave them potentially exposed to costs, such as copayments or uncovered services. It therefore provides a conservative measure of underinsurance in the United States.
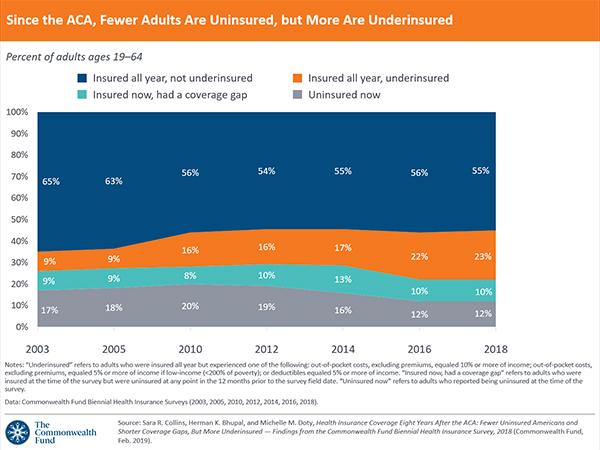
Compared to 2010, when the ACA became law, fewer people today are uninsured, but more people are underinsured. Of the 194 million U.S. adults ages 19 to 64 in 2018, an estimated 87 million, or 45 percent, were inadequately insured (see Tables 1 and 2).
Despite actions by the Trump administration and Congress to weaken the ACA, our survey found no statistically significant change in the adult uninsured rate by late 2018 compared to 2016 (Table 3). This finding is consistent with recent federal surveys, but other private surveys (including other Commonwealth Fund surveys) have found small increases in uninsured rates since 2016 (see “Changes in U.S. Uninsured Rates Since 2013”).
While there has been no change since 2010, statistically speaking, in the proportion of people who are insured now but have experienced a recent time without coverage, these reported gaps are of much shorter duration on average than they were before the ACA. In 2018, 61 percent of people who reported a coverage gap said it has lasted for six months or less, compared to 31 percent who said they had been uninsured for a year or longer. This is nearly a reverse of what it was like in 2012, two years before the ACA’s major coverage expansions. In that year, 57 percent of adults with a coverage gap reported it was for a year or longer, while one-third said it was a shorter gap.
There also has been some improvement in long-term uninsured rates. Among adults who were uninsured at the time of the survey, 54 percent reported they had been without coverage for more than two years, down from 72 percent before the ACA coverage expansions went into effect. The share of those who had been uninsured for six months or less climbed to 20 percent, nearly double the rate prior to the coverage expansions.
Of people who were insured continuously throughout 2018, an estimated 44 million were underinsured because of high out-of-pocket costs and deductibles (Table 1). This is up from an estimated 29 million in 2010 (data not shown). The most likely to be underinsured are people who buy plans on their own through the individual market including the marketplaces. However, the greatest growth in the number of underinsured adults is occurring among those in employer health plans.
Several factors may be contributing to high underinsured rates among adults in individual market plans and rising rates in employer plans:
It is well documented that people who gained coverage under the ACA’s expansions have better access to health care as a result.6 This has led to overall improvement in health care access, as indicated by multiple surveys.7 In 2014, the year the ACA’s major coverage expansions went into effect, the share of adults in our survey who said that cost prevented them from getting health care that they needed, such as prescription medication, dropped significantly (Table 4). But there has been no significant improvement since then.
The lack of continued improvement in overall access to care nationally reflects the fact that coverage gains have plateaued, and underinsured rates have climbed. People who experience any time uninsured are more likely than any other group to delay getting care because of cost (Table 5). And among people with coverage all year, those who were underinsured reported cost-related delays in getting care at nearly double the rate of those who were not underinsured.
There was modest but significant improvement following the ACA’s coverage expansions in the proportion of all U.S. adults who reported having difficulty paying their medical bills or said they were paying off medical debt over time (Table 4). Federal surveys have found similar improvements.8 However, those gains have stalled.
Inadequate insurance coverage leaves people exposed to high health care costs, and these expenses can quickly turn into medical debt. More than half of uninsured adults and insured adults who have had a coverage gap reported that they had had problems paying medical bills or were paying off medical debt over time (Table 6). Among people who had continuous insurance coverage, the rate of medical bill and debt problems is nearly twice as high for the underinsured as it is for people who are not underinsured.
Having continuous coverage makes a significant difference in whether people have a regular source of care, get timely preventive care, or receive recommended cancer screenings. Adults with coverage gaps or those who were uninsured when they responded to the survey were the least likely to have gotten preventive care and cancer screenings in the recommended time frame.
Being underinsured, however, does not seem to reduce the likelihood of having a usual source of care or receiving timely preventive care or cancer screens — provided a person has continuous coverage. This is likely because the ACA requires insurers and employers to cover recommended preventive care and cancer screens without cost-sharing. Even prior to the ACA, a majority of employer plans provided predeductible coverage of preventive services.9
U.S. working-age adults are significantly more likely to have health insurance since the ACA became law in 2010. But the improvement in uninsured rates has stalled. In addition, more people have health plans that fail to adequately protect them from health care costs, with the fastest deterioration in cost protection occurring in the employer market. The ACA made only minor changes to employer plans, and the erosion in cost protection has taken a bite out of the progress made in Americans’ health coverage since the law’s enactment.
Both the federal government and the states, however, have the ability to extend the law’s coverage gains and improve the cost protection of both individual-market and employer plans. Here is a short list of policy options:
Health care costs are primarily what’s driving growth in premiums across all health insurance markets. Employers and insurers have kept premiums down by increasing consumers’ deductibles and other cost-sharing, which in turn is making more people underinsured. This means that policy options like the ones we’ve highlighted above will need to be paired with efforts to slow medical spending. These could include changing how health care is organized and providers are paid to achieve greater value for health care dollars and better health outcomes.28 The government also could tackle rising prescription drug costs29 and use antitrust laws to combat the growing concentration of insurer and provider markets.30
Hospital Mergers Improve Health? Evidence Shows the Opposite

Many things affect your health. Genetics. Lifestyle. Modern medicine. The environment in which you live and work.
But although we rarely consider it, the degree of competition among health care organizations does so as well.
Markets for both hospitals and physicians have become more concentrated in recent years. Although higher prices are the consequences most often discussed, such consolidation can also result in worse health care. Studies show that rates of mortality and of major health setbacks grow when competition falls.
This runs counter to claims some in the health care industry have made in favor of mergers. By harnessing economies of scale and scope, they’ve argued, larger organizations can offer better care at lower costs.
In one recent example, two Texas health systems — Baylor Scott & White, and Memorial Hermann Health System — sought to merge, forming a 68-hospital system. The systems have since abandoned the plan, but not before Jim Hinton, Baylor Scott & White’s chief executive, told The Wall Street Journal that “the end, the more important end, is to improve care.”
Yet Martin Gaynor, a Carnegie Mellon University economist who been an author of several reviews exploring the consequences of hospital consolidation, said that “evidence from three decades of hospital mergers does not support the claim that consolidation improves quality.” This is especially true when government constrains prices, as is the case for Medicare in the United States and Britain’s National Health Service.
“When prices are set by the government, hospitals don’t compete on price; they compete on quality,” Mr. Gaynor said. But this doesn’t happen in markets that are highly consolidated.
In 2006, the National Health Service introduced a policy that increased competition among hospitals. When recommending hospital care, it required general practitioners to provide patients with five options, as well as quality data for each. Because hospital payments are fixed by the government — whichever hospital a patient chooses gets the payment for care provided to that patient — hospitals ended up competing on quality.
Mr. Gaynor was an author of a study showing that consequences of this policy included shorter hospital stays and lower mortality. According to the study, for every decrease of 10 percentage points in hospital market concentration, 30-day mortality for heart attacks fell nearly 3 percent.
Another study found that hospital competition in the N.H.S. decreased heart attack mortality, and several studies of Medicare also found that hospital competition results in lower rates of mortality from heart attacks and pneumonia.
Another piece of evidence in the competition-quality connection comes from other types of health care providers, including doctors. Recently, investigators from the Federal Trade Commission examined what happens when cardiologists team up into larger groups. The study, published in Health Services Research, focused on the health care outcomes of about two million Medicare beneficiaries who had been treated for hypertension, for a cardiac ailment or for a heart attack from 2005 to 2012.
The study found that when cardiology markets are more concentrated, these kinds of patients are more likely to have heart attacks, visit the emergency department, be readmitted to the hospital or die. These effects of market concentration are large.
To illustrate, consider a cardiology market with five practices in which one becomes more dominant — going from just below a 40 percent market share to a 60 percent market share (with the rest of the market split equally across the other four practices). The study found that the chance of having a heart attack would go up 5 to 7 percent as the largest cardiology practice became more dominant. The chance of visiting the emergency department, being readmitted to the hospital or dying would go up similarly.
The study also found that greater market concentration led to higher spending. And a different study of family doctors in England found that quality and patient satisfaction increased with competition.
For many goods and services, Americans are comfortable with the idea that competition leads to lower prices and better quality. But we often think of health care as different — that it somehow shouldn’t be “market based.”
What the research shows, though, is that there are lots of ways markets can function, with more or less government involvement. Even when the government is highly involved, as is the case with the British National Health Service or American Medicare, competition is a valuable tool that can drive health care toward greater value.