Some health systems have recovered from the pandemic much better than others, and those with healthier margins tend to be the ones that made a stronger push into outpatient care.
By the numbers:
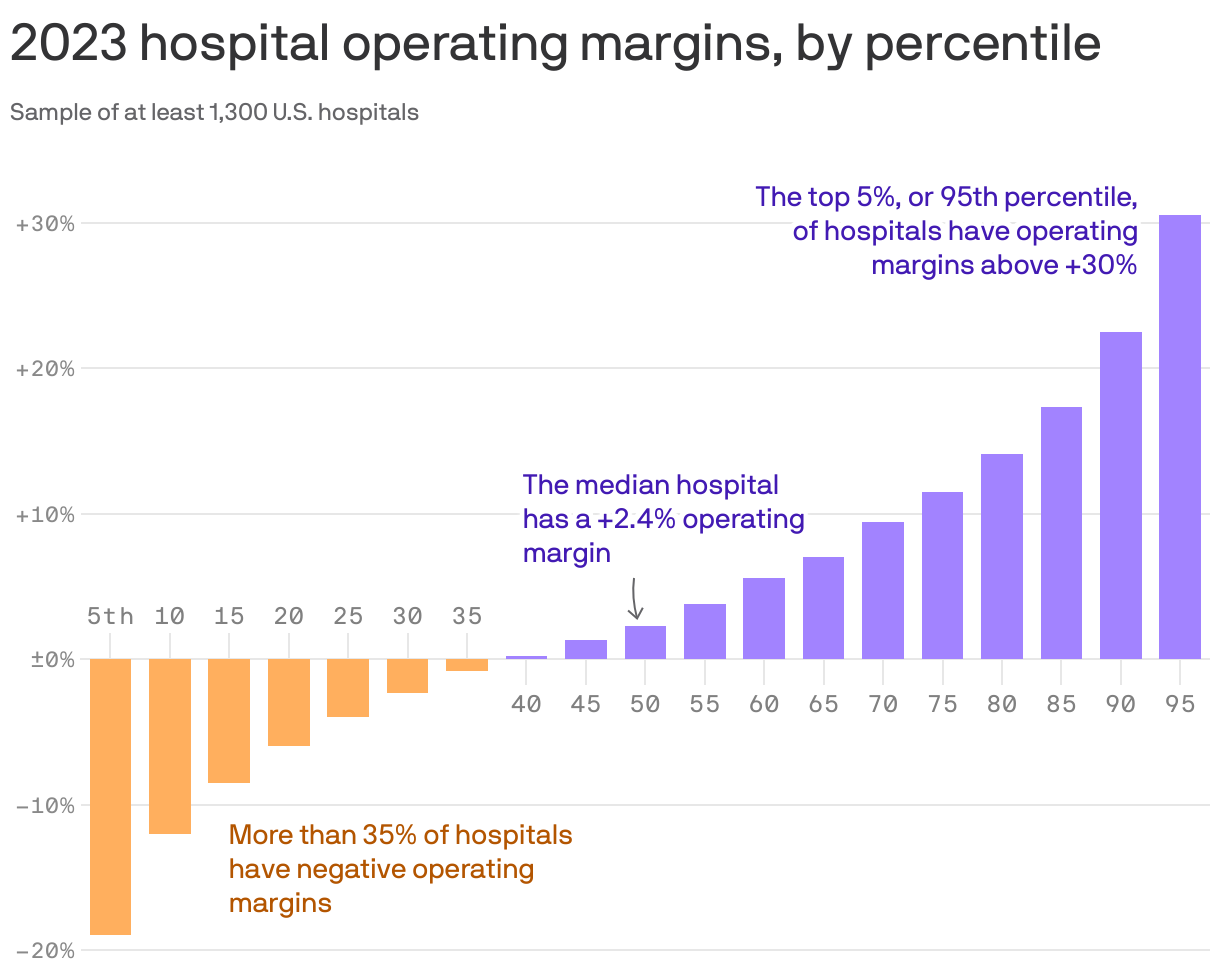
There’s a wildly large and growing difference between the operating margins of top-performing health systems and those at the bottom, according to Kaufman Hall data shared with Axios. (Go deeper on their analysis.)
“The hospitals that are not performing well are performing worse, but the hospitals that are recovering are performing extremely well,” firm co-founder Kaufman told Axios.
“I would say hospitals that are not doing particularly well … they’re not capturing that outpatient work, or at least not at the level that they need to,” he added.
Yes, but:
Operating margin is only one measure of a hospital’s financial health, and total margins are often much higher, said Anderson, the Johns Hopkins professor.
“You diversify where there is potential profit, and they have moved into all sorts of things where there is profit,” he added.“They have a whole portfolio of ways to make money now that they didn’t have 20 years [ago].”
Some experts also say that hospitals aren’t disciplined about keeping costs down.
“I think partly what happened over time is that … investments were not treated as investments, but as costs,” said Cooper, the Yale economist.
Hospitals’ business models are being upended by fundamental changes within the health care system, including one that presents a pretty existential challenge: People have far more options to get their care elsewhere these days.
Why it matters:
Health systems’ responses to major demographic, social and technological change have been controversial among policymakers and economists concerned about the impact on costs and competition.
Communities depend on having at least some emergency services available, making the survival of hospitals’ core services crucial.
But without adaptation — which is already underway in some cases — hospitals may be facing deep red balance sheets in the not-too-distant future, leading to facility closures and shutteredservices.
The big picture:
Many hospitals have recovered from the sector’s post-pandemic financial slump, which was driven primarily by staffing costs and inflation. But systemic, long-term trends will continue to challenge their traditional business model.
Many of the services that are shifting toward outpatient settings — like oncology, diagnostics and orthopedic care — are the ones that typically make hospitals the most money and effectively subsidize less profitable departments.
When hospitals lose these higher-margin services, “you’re starving the system that needs profits to provide services that we all might need, but particularly uninsured or underinsured people might need,” said UCLA professor Jill Horwitz.
And hospitals have long claimed that much higher commercial insurance rates make up for what they say are inadequate government rates.
But as the population ages and moves out of employer-sponsored health plans, fewer people will have commercial insurance, forcing hospitals to either cut costs or find new sources of revenue.
By the numbers:
Consulting firms are projecting a bleak decade for health systems.
Oliver Wyman recently predicted that under the status quo, hospitals will need to reduce their expenses by 15-20% by 2030 “to stay viable.”
Boston Consulting Group last year projected that health systems’ annual financial shortfall will total more than $200 billion by 2027, and their operating margins will have dropped by 10 percentage points.
To break even in 2027, a “typical” health system would need payment rate increases of between 5-8% annually — twice the rate growth over the last decade, according to BCG. If the load is borne solely by private insurers, hospitals will need a 10-16% year-over-year increase.
Between the lines:
This is the lens through which to view health systems’ spree of mergers and acquisitions, which have increasingly drawn criticism from policymakers, regulators and economists as being anticompetitive.
For better orworse, when hospitals have a larger market share, they are in a better position to negotiate and bring in more patients, and they can dilute some of the financial pain of poorer-performing facilities.
And when they acquire physician practices or other outpatient clinics, they’re still getting paid for delivering care even when patients aren’t receiving it in a traditional hospital setting.
“I think the hospitals have sort of said … ‘We can keep doing things the same way and we can just merge and get higher markups,'” said Yale economist Zack Cooper. “That push to consolidate is saying, ‘Let’s not move forward, let’s dig in.'”
Yes, but:
A big bonus of outpatient care is that it’s supposed to be cheaper. But when hospitals charge more for care than an independent physician’s office would have, or they tack on facility fees, costs don’t go down.
“They’ve protected their portfolio, and that’s added to the cost of health care,” said Johns Hopkins professor Gerard Anderson.
The other side:
Hospitals are typically on the losing end of negotiations with insurers right now, thanks to how large insurers have become, and are “in an extremely difficult competitive position,” said Ken Kaufman, co-founder of consulting agency Kaufman Hall.
Criticizing their mergers and acquisitions as anticompetitive is a “complete misunderstanding of the situation,” he said, and moving toward a new care model will take “an incredible amount of resources.”
Reality check:
Hospitals account for 30% of the country’s massive health spending tab, and they’ll have to be at the forefront of any real efforts to contain costs.
They’re also anchors in their communities and are powerful lobbyists, which helps explain why Congress has struggled to modestly reduce what Medicare pays hospital outpatient departments.
UPMC is laying off about 1,000 employees in a “realignment” the nonprofit said will help it face “the realities of a still-evolving, post-pandemic marketplace.”
The layoffs reflect about 1% of UPMC’s total workforce of over 100,000 people and are primarily among nonclinical and administrative staff, Vice President and Chief Communications Officer Paul Wood said in an emailed statement. He said the system will be offering those impacted “enhanced severance pay and benefits coverage.”
The “limited reductions” will also involve the closing of open positions, the elimination of redundancies and “other actions,” Wood said.
“This realignment will not alter UPMC’s investments in our communities, facilities, commitment to clinical care and research, strategic growth or to offering those throughout our workforce industry-leading benefits,” Wood wrote in the statement.
Pittsburgh-based UPMC is an integrated health system and one of Pennsylvania’s largest employers. Its provider, insurance and other business arms logged $27.7 billion of revenue across 2023 as volumes rose and insurance membership grew.
However, the nonprofit reported a $198.3 million operating loss (-0.7% operating margin) last year as insurance claims expenses jumped 13.6% and labor costs rose 6.4%. It had posted a $162 million operating gain (0.6% operating margin) the year before.
The system did narrow its 2023 bottom line loss to $31 million thanks to its investment returns, though it had logged roughly a billion in net losses during the 2022 fiscal year.
In its year-end financial report, UPMC’s management wrote that “even with increased expenses to deliver high-quality care as a result of various economic factors, in 2023 UPMC continued to forge ahead with investments to grow access to world-class clinical care … advance healthcare excellence through quality and innovation, care for our communities, grow our insurance services and invest in our future workforce.”
Long-term debt has long been a staple in healthcare, but many hospitals and health systems are responding to the increasing cost of debt and debt service in the rising rates environment.
Highly levered health systems are looking to sell hospitals, facilities or business lines to reduce their debt leverage and secure long-term sustainability, which creates significant growth opportunities for systems with balance sheets on a more solid financial footing.
Forty-three health systems ranked by their long-term debt:
Note: This is not an exhaustive list. The following long-term debt figures are taken from each health system’s most recent financial report.
The Federal Trade Commission banned noncompete agreements for most U.S. workers Tuesday with a new rule that will bar employers from enforcing clauses that restrict workers from switching employers within their industry, which the agency said suppresses wages and gums up labor markets.
The FTC voted 3 to 2 Tuesday to issue the rule it proposed more than a year ago. The new rule makes it illegal for employers to include the agreements in employment contracts and requires companies with active noncompete agreements to inform workers that they are void. The agency received more than 26,000 comments about the rule after it was proposed some 16 months ago. The rule will take effect after 180 days, although business groups have promised to challenge it in court, which could delay implementation.
Scholars cite a body of research that shows the agreements suppress worker pay and entrepreneurship while also imposing costs on firms wanting to hire workers bound by the agreements. A Labor Department study published in June 2022 estimated that 18 percent of Americans are bound by noncompete agreements, while other research suggests it could be closer to 5o percent. They are used in a wide range of industries, including technology, hairstyling, medicine and even dance instruction, while imposing restrictions on both high- and low-wage earners.
The FTC estimates that banning noncompete agreements could create jobs for 30 million Americans and raise wages by nearly $300 billion per year.
“I think the FTC has done a real public service here by compiling all this evidence, making a really strong case for a complete ban and establishing a new gold standard for policymaking in this area,” said Sandeep Vaheesan, legal director at the Open Markets Institute, which proposed a noncompete ban to the agency in 2019. “No employee or professional should be made to sign one of these contracts.”
Business groups opposed to the rule, such as the U.S. Chamber of Commerce, have said that the contracts are necessary to protect proprietary information and training, and justify investing in workers who might otherwise immediately jump to a competitor. The Chamber has argued the rule represents a “radical expansion” of the FTC’s authority and has vowed the challenge the rule in court.
Noncompete agreements have been prohibited in three states — California, North Dakota and Oklahoma — for more than a century. In recent years, 11 states and Washington, D.C., have passed laws that prohibit the agreements for hourly wage workers or those who fall below a salary threshold.
But the patchwork nature of the legal landscape has made bans difficult to enforce. Some legal experts said that companies include noncompete clauses in employee contracts regardless of state prohibitions, knowing workers and competitors will be wary of litigation.
Some observers fear that employers will also find workarounds to the FTC rule, but Vaheesan said that a federal rule will provide legal clarity and send a strong message.
“It establishes, in the place of this mushy standard that exists in most states, a bright line,” he said. “So everyone will know these contracts are illegal.”
After covering the Medicare privatization crisis for over two years, an investigative reporter takes a step back and examines what’s at stake.
Medicare, the country’s largest and arguably most successful health care program, is under duress, weakened by decades of relentless efforts by insurance companies to privatize it.
A rapidly growing Medicare Advantage market — now 52% of Medicare beneficiaries, up from 37% in 2018 — controlled by some of the largest and most powerful corporations in the world, threatens to both drain the trust fund and eliminate Medicare’s most important and controversial component: its ability to set prices.
It is not an overstatement to call it a heist of historic proportions, endangering the health not only of the more than 65 million seniors and people with disabilities who depend on Medicare but all Americans who benefit from the powerful role that Medicare has historically played in reining in health care costs.
The giant corporations that dominate Medicare Advantage have rigged the system to maximize payments from our government to the point that they are now being overpaid between $88 billion and $140 billion a year. The overpayments could soar to new heights if the insurers get their way and eliminate traditional Medicare.
All of America’s seniors and disabled people who depend on Medicare could soon be moved to a managed care model of ever-tightening networks, relentless prior authorization requirements and limited drug formularies. The promise of a humane health care system for all would be sacrificed at the altar of the almighty insurer dollar.
The Medicare Payments Advisory Commission (MedPAC), the independent congressional agency tasked with overseeing Medicare, last month released a searing report which found that Medicare spends 22% more per beneficiary in Medicare Advantage plans than if those beneficiaries had been enrolled in traditional fee-for-service Medicare. That’s up from a 6% estimate in the prior year.
A similar cost trend exists for diagnosis coding.
Medicare Advantage plans and their affiliated providers increasingly upcoded diagnoses to get higher reimbursements. In 2024, overpayments due to upcoding could total $50 billion, according to MedPAC, up from $23 billion in 2023. These enormous overpayments drive up the cost of premiums — MedPAC’s conservative estimate is that the premiums paid to Medicare out of seniors’ Social Security checks will be $13 billion higher in 2024 because of those overpayments.
There is evidence that Americans and lawmakers are starting to wake up.
Medicare Advantage enrollment growth slowed considerably in 2023. Support within the Democratic Party for Medicare Advantage is cratering. In 2022, 147 House Democrats signed an industry-backed letter supporting Medicare Advantage. This year, just 24 House Democrats signed the letter. Earlier this month, the Biden administration cut Medicare Advantage base payments for the second year in a row(while still increasing payments overall), over the fierce opposition of the insurance lobby. The investment bank Stephens called Biden’s decision a “highly adverse” outcome for insurers. Wall Street has taken note, punishing the stock price of the largest Medicare Advantage insurers, with Barron’s noting that Wall Street’s “love affair” with Humana is “ending in tears.” The cargo ship is turning. It is up to us to determine if that will be enough.
We can’t attack a problem if we don’t know how to diagnose it. I spoke with some of the most knowledgeable critics of Medicare Advantage about the danger the rapid expansion of Medicare privatization presents to the American public.
Rick Gilfillan is a medical doctor who in 2010 became the first director of the Center for Medicare and Medicaid Innovation (CMMI). He would go on to serve as CEO of Trinity Health from 2013 to 2019. In 2021 he launched an effort to halt the involuntary privatization of Medicare benefits.
“Right now, all investigations are finding tremendous overpayments,” Gilfillan said. “The overpayments are based on medical diagnoses that may or may not be meaningful from a patient care standpoint. Insurers are using chart reviews, nurse home visits and AI software to find as many diagnoses as possible and thereby inflate the health risks of the patients and the premium they get from Medicare. The overpayments are just outrageous,” he said.
The problem could get worse if the Supreme Court curtails the powers of regulatory agencies, as it may do this year. “It would make a huge difference in what CMS would be able to do,” Gilfillan said.
The logic behind Medicare privatization is that seniors and people with disabilities use too much care, egged on by their doctors. If true, a solution could have been to enforce the Stark Law, which bans physicians from having financial relationships with providers they refer to, or other anti-kickback statutes. States could also enforce laws 33 of them have enacted that prohibit the “corporate practice of medicine.”
Instead, health insurers were invited and incentivized by previous administrations to compete with the original Medicare program and “manage” beneficiaries’ care. Under this model— set in its modern form in 2003 — Medicare Advantage insurers are paid a rate based on a complex risk modeling process and estimated costs.
But Medicare Advantage plans have never been cheaper than traditional Medicare, as MedPAC has repeatedly pointed out.
This is a far more complex approach than the fee-for-service model in which CMS sets prices in health care in a public and transparent manner, Gilfillan notes. The prices negotiated by Medicare Advantage companies, by contrast, are not disclosed.
“With fee-for-service, a patient is provided a service, treatment or medication. The physician who provides the service charges a specific amount for that service,” Gilfillan said. “And then Medicare pays whatever it decided it was worth for that service. The benefit is you pay for what you get.”
Some Medicare Advantage plans use a “capitated” approach in paying primary care physicians. The amount is based on the premium they receive for the patient. The more codes submitted, the higher the capitation, the greater the profit. That approach is having far-reaching economic impacts on health care, said Hayden Rooke-Ley, an Oregon-based lawyer and health care consultant who co-authored a recent New England Journal of Medicine article on the corporatization of primary care. It is the capitation model, he says, that drives the rampant upcoding among Medicare Advantage plans.
From Horizontal to Vertical
“An undercovered aspect of Medicare Advantage is the way it is fueling vertical consolidation” in the insurance business, Rooke-Ley added, noting that until recent years, insurers bulked up by buying smaller competitors (known as horizontal integration). “With so much government money, we’re seeing insurance companies restructuring themselves as vertically integrated conglomerates [through the acquisition of physician practices, clinics and pharmacy operations] to become even more profitable, especially in Medicare Advantage.”
“A key part of this strategy is to own primary care practices,” he said, citing Humana’s partnership with the private-equity firm Welsh Carson to become the largest owner of Medicare-based primary care, CVS/Aetna’s acquisition of Oak Street, and UnitedHealth’s roll up of doctors practices across the country.
As Rooke-Ley explained, control of primary care allows insurance companies to more easily manipulate “risk scores” to increase payments from the government by claiming patients are in worse health than they really are.
“The easiest way to increase risk scores, short of simply fabricating diagnosis codes, is to control the behavior of physicians and other clinicians,” he said.
“When an insurance company owns the physician practice, it can configure workflows, technology, and incentives to drive risk coding.
UnitedHealth, for example, can preferentially schedule Medicare Advantage patients – and it can choose to reach out to health plan enrollees it identifies with its data as having high ‘coding opportunities.’ It can require its doctors to go to risk-code training, and it can prohibit doctors from closing their notes before they address all the ‘suggested’ diagnosis codes.”
“While Medicare Advantage insurance companies tout all their provider acquisitions as investments in value-based care, the concern is that it’s really just looking like a game of financialization,” Rooke-Ley said. “MA was supposed to save Medicare money, but the exact opposite has happened.
According to MedPAC, the government will over-subsidize MA to the tune of $88 billion this year, with $54 billion of that due to excess risk coding relative to what we see in traditional Medicare. That’s a staggering amount of money that could go directly to patients and clinicians by strengthening traditional Medicare.”
Two Possible Futures
There are two options for the future of Medicare, said Dr. Ed Weisbart, former chief medical officer of the pharmacy benefit manager Express Scripts, which Cigna bought in 2018, who now leads the Missouri chapter of Physicians for a National Health Program.
In one future, he said, “We will change the trajectory and get rid of the profiteers, and manage to divert the funds that are being profiteered to patient care.”
In another future, the business practices of Medicare Advantage plans “will be unfettered and more damaging and harmful than they are today,” he said. “If we continue on this course we’ll find an increasingly polarized health care system that caters increasingly to the wealthy and privileged. The barriers to care will be worse.”