In the mid 1960’s, Medicare was first created as a “Social Insurance Program”, designed to be consistently applied to all older Americans. Comprehensive, inexpensive, and relevant to the standards-of-care at the time, this was considered “Good” Coverage.
But the passing of years unveiled a multitude of unanticipated dynamics.
For example, the very definition of “health care” has both broadened and deepened materially since 1965. The first MRI or the first Angioplasty would not occur until a decade later.
Meanwhile, the age-65 life expectancy has expanded by nearly 50% since then, exposing the medical system to care demands and opportunities never contemplated, late in life.
While care technology, science and processes have responded to this expanding demand, they brought with them dramatically accelerating costs, year after year.
Finally, political pressures to respond to special populations, including dialysis patients, or emerging care settings like home health or hospice, or even outpatient prescription drugs… all resulted in substantial Medicare Program scope creep.
So it should not be surprising that since inception, Medicare COVERAGE itself has required regular, often dramatic modifications to keep its “social insurance purpose” in balance with these and other continually changing demands. Some of that pressure has even challenged the highly protected “social Insurance” model itself:
By the early 2000’s, these pressures yielded to means-based-pricing for seniors of varying income levels
A 2013 survey of Americans over age 65 revealed “raising the age of eligibility to 67” as the second most popular to reduce costs and improve long term viability.
Americans Are Not Very Informed About Medicare
Most Americans (even beneficiaries) are not really aware of the full effect of these sequential program changes, because they have been spread out over many years. After all, the Medicare program has been around for 50 years, but most beneficiaries participate for less than a dozen years. So, many assume this program has been stable and managable year after year, with surprising simplicity and effectiveness. But Medicare Coverage is not at all what it was 50 years ago.
Consider a small number of coverage dynamics between the late 1960’s and today:
Other coverage details and provisions have had to change along the way too, few offsetting the additional copayments, co-insurance, annual and lifetime limits or out-of-pocket cost exposure for beneficiaries.
Could Today’s Medicare Even Work Without The Private Market?
These exposures explain why most Medicare beneficiaries are compelled to purchase a supplemental private insurance plan to cover those costs not covered by today’s Medicare. Such private plans are called Medicare Supplement Plans, and they have been increasingly necessary as the exposures under the Traditional Medicare program have grown over the years. But they too have become expensive due to the the increasing uncovered portions of Medicare. Over the years, the average Medicare Supplement has increased in price from less than $20 per month in the 1980’s to a few Hundred dollars per month today.
Alternatively, Medicare beneficiaries today can choose to leave Traditional Medicare altogether, and apply their “benefit equivalent eligibility” to the purchase of an alternative from a private Insurance company. These programs, called Medicare Advantage Plans, attract nearly 1/3 of all Medicare Beneficiaries who simply can’t make Traditional Medicare pencil out.
So What Does This Mean?
Most of the Medicare-For-All proposals don’t advertise the high coverage gaps in the current model, and the dependency on either a private market supplement (Medicare Supplement Plans), or private market alternative (Medicare Advantage Plans). Without these, Medicare-For-All will be woefully inadequate to meet the coverage expectations of Americans. Alternatively, Medicare-For-All proposals could completely re-invent what Medicare is , increasing its coverage and raising its price substantially.
… like liberty and justice, Medicare is imagined by some to be All-American. But is it? Can it be? Should it be?
A Historical Perspective:
In 1965, the first year of Medicare, nearly 19 Million Americans enrolled, 56% of whom were previously uninsured according to a Kennedy-era study. It was a simple program back then, providing only acute hospital and physician coverage for Americans over age 65. It was the only real health insurance option for people over age 65, virtually all of whom retired by that age back then.
Today, an estimated 63 Mil or 18% of the US population are eligible for Medicare. And after decades of major program changes, the 2018 program covers more than just older Americans, and Medicare coverage is more complex and broader than the original program. Like the original program (Traditional Medicare), the coverage still has substantial patient exposures for deductibles, co-payments and lifetime / per-incident limits. And, despite popular folklore, it is far more expensive due to the same pressures that impact coverages for the rest of us.
Along the way, other alternative or complementary coverages have emerged. No surprise, this dynamic reflects in part, the vastly different nature and demands of American consumers including older American consumers. These newer coverage sources include private insurers, employers, unions, states, municipalities and school districts as well as expanded coverages for the poor (including the older poor).
Does Medicare ALONE Work For Those That Have Access Today?
Consider this:
38 Mil, or only 60% of those eligible are enrolled in Traditional Medicare. But because of indexing coverage limitations, only 19% of these Traditional Program participants do not have some form of supplemental or alternative coverage.
Another 9 Mil are over 65 but still working, and only because of their employer wrap-around coverage, Medicare is workable.
Another 21 Mil are enrolled in Private Alternatives to Medicare called Advantage Plans after opting out of Traditional Medicare. In 2018 there were 2,317 such Medicare Advantage plans available nationwide allowing the average beneficiary to choose among 21, an increase from 19 in 2017. This is anything but single-payer and becoming less single-payer-like each year due to natural market dynamics.
Finally, 12 Mil of all of these are also enrolled in Medicaid (dually eligible), due to low income, disability, etc. Most are part of the 38 Mil people with Traditional Medicare, but only because of the Medicaid program, their Medicare is coverage and price affordable and/or relevant.
What Does This Say About Medicare For All?
Nearly 1/2 of all who are offered Medicare today choose a private market alternative, or can only make it work due to other private market wraparound safety nets. So why do we think Medicare will be attractive to the rest of the population without similar private market protections?
It’s staggering to think of the challenges that CAHs face. Now OIG is calling for a re-examination of a program that it says has overpaid CAHs billions of dollars to provide skilled nursing services using hospital swing beds.
They’re called “Critical Access Hospitals” for a reason. These tiny healthcare outposts provide “critical access” to people who live in remote areas.
That was the intent of the legislation that created CAHs in 1997 at a time when rural hospitals were shuttering at an alarming rate. Congress understood that rural America needed extra Medicare dollars to keep the doors open at hospitals that serve an older, sicker and poorer patient mix.
It’s staggering to think of the challenges that CAHs face:
Because of their location and size, CAHs have few economies of scale, little leverage with vendors or payers, or a sufficiently large patient mix or volume of commercial payers to help cover costs.
CAHs are often limited in their ability to provide some of the more lucrative services that are cash cows for larger hospitals in urban areas.
Recruiting clinicians to rural areas is a slog.
And because of all those challenges, it’s also more difficult to merge or collaborate with other healthcare providers from such an isolated perch. It’s surprising to learn that only 40% of CAHs operate in the red.
Unfortunately, some people in Washington, DC have short institutional memories.
For the past couple of years, reports from the Office of the Inspector General at the Department of Health and Human Services have made it clear that they believe the CAH designation and funding scheme should be overhauled.
In its latest shot across the bow, OIG this week called for a re-examination of the swing bed program that allows CAHs to provide long-term care. The OIG audit claimed that the federal government has overpaid CAHs $4.1 billion over the past six years for services that could have cost less in relatively nearby skilled nursing and long-term care facilities.
Tavenner Pushes Back
Rural healthcare advocates rallied around the reply to the OIG recommendations from former Centers for Medicare & Medicaid Services Administrator Marilyn Tavenner, who challenged the OIG findings and recommendations in her formal response, and suggested that auditors don’t understand healthcare delivery in rural areas.
In that same response to OIG, however, Tavenner said the Obama 2016 budget has called for reducing the Medicare reimbursement that CAHs receive from 101% to 100% of allowable costs, and reassessing and eliminating CAH status for hospitals that are within 10 miles each other.
For a patient’s knee replacement, Medicare will pay a hospital $17,000. The same hospital can get more than twice as much, or about $37,000, for the same surgery on a patient with private insurance.
Or take another example: One hospital would get about $4,200 from Medicare for removing someone’s gallbladder. The same hospital would get $7,400 from commercial insurers.
The yawning gap between payments to hospitals by Medicare and by private health insurers for the same medical services may prove the biggest obstacle for advocates of “Medicare for all,” a government-run system.
If Medicare for all abolished private insurance and reduced rates to Medicare levels — at least 40 percent lower, by one estimate — there would most likely be significant changes throughout the health care industry, which makes up 18 percent of the nation’s economy and is one of the nation’s largest employers.
Some hospitals, especially struggling rural centers, would close virtually overnight, according to policy experts.
Others, they say, would try to offset the steep cuts by laying off hundreds of thousands of workers and abandoning lower-paying services like mental health.
he prospect of such violent upheaval for existing institutions has begun to stiffen opposition to Medicare for all proposals and to rattle health care stocks. Some officials caution that hospitals providing care should not be penalized in an overhaul.
Dr. Adam Gaffney, the president of Physicians for a National Health Program, warned advocates of a single-payer system like Medicare for all not to seize this opportunity to extract huge savings from hospitals. “The line here can’t be and shouldn’t be soak the hospitals,” he said.
“You don’t need insurance companies for Medicare for all,” Dr. Gaffney added. “You need hospitals.”
Soaring hospital bills and disparities in care, though, have stoked consumer outrage and helped to fuel populist support for proposals that would upend the current system. Many people with insurance cannot afford a knee replacement or care for their diabetes because their insurance has high deductibles.
Proponents of overhauling the nation’s health care argue that hospitals are charging too much and could lower their prices without sacrificing the quality of their care. High drug prices, surprise hospital bills and other financial burdens from the overwhelming cost of health care have caught the attention (and drawn the ire) of many in Congress, with a variety of proposals under consideration this year.
But those in favor of the most far-reaching changes, including Senator Bernie Sanders, who unveiled his latest Medicare for all plan as part of his presidential campaign, have remained largely silent on the question of how the nation’s 5,300 hospitals would be paid for patient care. If they are paid more than Medicare rates, the final price tag for the program could balloon from the already stratospheric estimate of upward of $30 trillion over a decade. Senator Sanders has not said what he thinks his plan will cost, and some proponents of Medicare for all say these plans would cost less than the current system.
The nation’s major health insurers are sounding the alarms, and pointing to the potential impact on hospitals and doctors. David Wichmann, the chief executive of UnitedHealth Group, the giant insurer, told investors that these proposals would “destabilize the nation’s health system and limit the ability of clinicians to practice medicine at their best.”
“There’s a hospital in every congressional district,” he said. Passing a Medicare for all proposal in which hospitals are paid Medicare rates “is going to be a really hard proposition.”
Richard Anderson, the chief executive of St. Luke’s University Health Network, called the proposals “naïve.” Hospitals depend on insurers’ higher payments to deliver top-quality care because government programs pay so little, he said.
“I have no time for all the politicians who use the health care system as a crash-test dummy for their election goals,” Mr. Anderson said.
The American Hospital Association, an industry trade group, is starting to lobby against the Medicare for all proposals. Unlike the doctors’ groups, hospitals are not divided. “There is total unanimity,” said Tom Nickels, an executive vice president for the association.
“We agree with their intent to expand coverage to more people,” he said. “We don’t think this is the way to do it. It would have a devastating effect on hospitals and on the system over all.”
Rural hospitals, which have been closing around the country as patient numbers dwindle, would be hit hard, he said, because they lack the financial cushion of larger systems.
Big hospital systems haggle constantly with Medicare over what they are paid, and often battle the government over charges of overbilling. On average, the government program pays hospitals about 87 cents for every dollar of their costs, compared with private insurers that pay $1.45.
Some hospitals make money on Medicare, but most rely on higher private payments to cover their overall costs.
Medicare, which accounts for about 40 percent of hospital costs compared with 33 percent for private insurers, is the biggest source of hospital reimbursements. The majority of hospitals are nonprofit or government-owned.
The profit margins on Medicare are “razor thin,” said Laura Kaiser, the chief executive of SSM Health, a Catholic health system. In some markets, her hospitals lose money providing care under the program.
She says the industry is working to bring costs down. “We’re all uber-responsible and very fixated on managing our costs and not being wasteful,” Ms. Kaiser said.
“If you’re in a consolidated market, you are a monopolist and are setting the price,” said Mark Miller, a former executive director for the group that advises Congress on Medicare payments. He describes the prices paid by private insurers as “completely unjustified and out of control.”
Many hospitals have invested heavily in amenities like single rooms for patients and sophisticated medical equipment to attract privately insured patients. They are also major employers.
“You would have to have a very different cost structure to survive,” said Melinda Buntin, the chairwoman for health policy at the Vanderbilt University School of Medicine. “Everyone being on Medicare would have a large impact on their bottom line.”
People who have Medicare, mainly those over 65 years old, can enjoy those private rooms or better care because the hospitals believed it was worth making the investments to attract private patients, said Craig Garthwaite, a health economist at the Kellogg School of Management at Northwestern University. If all hospitals were paid the same Medicare rate, the industry “should really collapse down to a similar set of hospitals,” he said.
Whether hospitals would be able to adapt to sharply lower payments is unclear.
“It would force health care systems to go on a very serious diet,” said Stuart Altman, a health policy professor at Brandeis University. “I have no idea what would happen. Nor does anyone else.”
But proponents should not expect to save as much money as they hope if they cut hospital payments. Some hospitals could replace their missing revenue by charging more for the same care or by ordering more billable tests and procedures, said Dr. Stephen Klasko, the chief executive of Jefferson Health. “You’d be amazed,’ he said.
While both the Medicare-for-all bill introduced by Representative Pramila Jayapal, Democrat of Washington, and the Sanders bill call for a government-run insurance program, the Jayapal proposal would replace existing Medicare payments with a whole new system of regional budgets.
“We need to change not just who pays the bill but how we pay the bill,” said Dr. Gaffney, who advised Ms. Jayapal on her proposal.
Hospitals would be able to achieve substantial savings by scaling back administrative costs, the byproduct of a system that deals with multiple insurance carriers, Dr. Gaffney said. Under the Jayapal bill, hospitals would no longer be paid above their costs, and the money for new equipment and other investments would come from a separate pool of money.
But the Sanders bill, which is supported by some Democratic presidential candidates including Senators Kirsten Gillibrand of New York, Cory Booker of New Jersey, Elizabeth Warren of Massachusetts and Kamala Harris of California, does not envision a whole new payment system but an expansion of the existing Medicare program. Payments would largely be based on what Medicare currently pays hospitals.
Some Democrats have also proposed more incremental plans. Some would expand Medicare to cover people over the age of 50, while others wouldn’t do away with private health insurers, including those that now offer Medicare plans.
Even under Medicare for all, lawmakers could decide to pay hospitals a new government rate that equals what they are being paid now from both private and public insurers, said Dr. David Blumenthal, a former Obama official and the president of the Commonwealth Fund.
“It would greatly reduce the opposition,” he said. “The general rule is the more you leave things alone, the easier it is.”
According to data from CMS, while dual-eligible patients make up only 15 percent of Medicaid enrollees, they are responsible for 33 percent of the program’s expenditures.
The Centers for Medicare & Medicaid Services is looking to partner with states to determine better models to treat the 12 million dual-eligible Medicaid and Medicare beneficiaries in the country.
CMS and states spend more than $300 billion annually on this patient population, many of whom suffer from multiple chronic conditions made more difficult to treat by social and economic barriers.
The cost for dual-eligible population is outsized when compared to its size. According to data from CMS, while dual-eligible patients make up only 15 percent of Medicaid enrollees, they are responsible for 33 percent of the program’s expenditures.
“Less than 10 percent of dually eligible individuals are enrolled in any form of care that integrates Medicare and Medicaid services, and instead have to navigate disconnected delivery and payment systems,” CMS Administrator Seema Verma said in a statement.
“This lack of coordination can lead to fragmented care for individuals, misaligned incentives for payers and providers, and administrative inefficiencies and programmatic burdens for all.”
The goal from the agency is to promote new models which can better integrate Medicare and Medicaid services and create a more seamless experience for both beneficiaries and providers working across the two programs.
One major goal is to allow states to share in savings and benefits gained from investment in better care for the dual-eligible population.
In a letter addressed to state Medicaid leaders, Verma laid out a few potential payment approaches to address the issue of dual eligible patients, including a capitated payment model which would provide the full array of Medicare and Medicaid services with a set dollar reimbursement amount.
Nine states are currently piloting the model, which creates a three-way contract between the state, CMS and Medicare-Medicaid Plans. So far, CMS said state savings for states have averaged 4.4 percent in these test markets.
Through the experiments, Verma said the agency has been able to foster a competitive marketplace with multiple offerings that incentivizes health plans to invest in services that address the patient population.
CMS said it is currently open to extending the initial state pilots and expanding the geographic scope of the capitated programs.
For states that administer dual-eligible patients on a fee-for-service basis, Verma laid out a merged managed care model that would allow states to share in Medicare savings for metrics like reducing hospital readmissions.
Washington and Colorado are currently testing out the model. In one instance, providers in Washington are using Medicaid health homes to deliver high-intensity care to high-risk beneficiaries and sharing in the cost savings.
CMS said preliminary data from Washington’s program has been positive, with gross savings for Medicare Part A and Part B of 11 percent over three years. This has resulted in $36 million in performance payments to the state.
The letter from CMS also opens up the opportunity to potentially partner on state-specific models developed internally meant to better serve dual eligible patients and reduce Medicare and Medicaid expenditures.
CMS has made payment delivery reform a key initiative, with the ultimate goal of moving towards a outcomes-based payment system and reducing expenditures as Medicare faces an uncertain future.
Anyone interacting with the U.S. health care system is bound to encounter examples of unnecessary administrative complexity—from filling out duplicative intake forms to transferring medical records between providers to sorting out insurance bills. This administrative complexity, with its associated high costs, is often cited as one reason the United States spends double the amount per capita on health care compared with other high-income countries even though utilization rates are similar.1
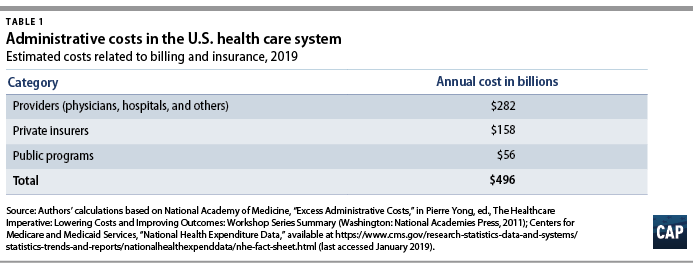
Each year, health care payers and providers in the United States spend about $496 billion on billing and insurance-related (BIR) costs, according to Center for American Progress estimates presented in this issue brief. As health care costs continue to rise, a logical starting point for potential savings is addressing waste. A 2010 report by the National Academy of Medicine (NAM) estimated that the United States spends about twice as much as necessary on BIR costs.2 That administrative excess currently amounts to $248 billion annually, according to CAP’s calculations.
This issue brief provides an overview of administrative expenditures in the U.S. health care system. It first explains the components of administrative costs and then presents estimates of the administrative costs borne by payers and providers. Finally, the issue brief describes how the United States can lower administrative costs through comprehensive reforms and incremental changes to its health care system. Many of the universal health care plans being discussed to expand coverage and lower costs would lower administrative costs through rate regulation, global budgeting, or simplifying the number of payers.3 Each of these financing changes deserves consideration—even in the absence of major systemwide reform.
Components of administrative costs
The main components of administrative costs in the U.S. health care system include BIR costs and hospital or physician practice administration.4 The first category, BIR costs, is part of the administrative overhead that is baked into consumers’ insurance premiums and providers’ reimbursements. It includes the overhead costs for the health insurance industry and providers’ costs for claims submission, claims reconciliation, and payment processing. The health care system also requires administration beyond BIR activities, including medical record-keeping; hospital management; initiatives that monitor and improve care quality; and programs to combat fraud and abuse.
To date, few studies have estimated the systemwide cost of health care administration extending beyond BIR activities. In a 2003 article in The New England Journal of Medicine, researchers Steffie Woolhandler, Terry Campbell, and David Himmelstein concluded that overall administrative costs in 1999 amounted to 31 percent of total health care expenditures or $294 billion5—roughly $569 billion today when adjusted for medical care inflation.6 A more recent paper by Woolhandler and Himmelstein, which looked at 2017 spending levels, placed the total cost of administration at $1.1 trillion.7
Billing and insurance-related costs
Many studies of administrative costs limit their scope to BIR costs. The BIR component of administration is most relevant to systemwide reforms that seek to reduce the expenses related to claims processing, billing rates, or health insurance. The largest share of BIR costs is attributable to insurance companies’ profits and overhead and to providers8where BIR costs include tasks such as record-keeping for claims submission and billing.
The costs associated with BIR administration can extend beyond the chief parties involved in receiving and submitting claims. The process of claims denials has become an industry unto itself, with private firms squeezing dollars out of Medicaid programs.9 One study estimated that the aggregate value of challenged claims ranges from $11 billion to $54 billion annually.10 Claims can also be manipulated to boost providers’ or insurers’ profits by recording services rendered in maximum detail and exaggerating the severity of patients’ conditions—a practice known as upcoding.11 Upcoding costs Medicare Advantage billions of dollars in excess expenditures,12 and in many cases the practice constitutes fraud.13
The NAM published one of the most thorough reports on U.S. administrative costs related to billing and insurance in 2010. In a synthesis of the literature on administrative costs, the NAM report concluded that BIR costs totaled $361 billion in 2009—about $466 billion in current dollars—among private insurers, public programs, and providers, amounting to 14.4 percent of U.S. health care spending at the time. The NAM estimated that BIR costs account for 13 percent of physician care spending; 8.5 percent of hospital care spending; 10 percent of spending on other providers; 12.3 percent of spending on private insurance; and 3.5 percent of public program spending, including Medicare and Medicaid.14
Applying the NAM’s percentages of BIR costs to recent projections of national health expenditures from the Centers for Medicare and Medicaid Services (CMS), CAP estimates that BIR costs will amount to $496 billion for 2019.15 (see Table 1) According to CAP’s calculations, this includes $158 billion in overhead for private insurance; $56 billion for administration of public insurance programs; and $282 billion for the BIR costs of hospitals, physicians, and other care providers. CAP’s estimate does not include the administrative costs associated with retail sales of medical products, including prescription drugs and durable medical equipment.
Even the most inclusive studies of administrative costs have not included at least one key piece of the U.S. health care system, namely, patients.16 The administrative complexity of the U.S. system also burdens patients, whether they are deciphering bewildering bills or shuttling records between providers. Three-quarters of consumers report being confused by medical bills and explanations of benefits.17 A Kaiser Family Foundation survey of people newly enrolled in the health insurance marketplace found that many were not confident in their understanding of the definitions of basic terms and concepts such as “premium,” “deductible,” or “provider network.”18 Insurers and employers spend an estimated $4.8 billion annually to assist consumers with low health insurance literacy, according to the consulting firm Accenture.19
Excess administrative costs
While U.S. administrative care spending is indisputably higher than that of other comparable countries, it’s unclear how much of the difference is excess and how much of that excess could be trimmed. The NAM report estimated that excess BIR costs amount to $190 billion—$245 billion in current dollars—or roughly half of total BIR expenditures in a year.20 The NAM report estimated that 66 percent of BIR costs for private insurers and 50 percent of BIR costs among providers are excess.21Based on these percentages, $248 billion of the total $496 billion BIR costs in CAP’s updated estimate are excess administrative costs.
Most studies that have attempted to identify excess costs in the American health care system rely on comparisons between the United States and Canada.22 In their 2010 review of the literature on the difference between the two countries’ health expenditures, economists Alexis Pozen and David M. Cutler looked at the sources of the gap between U.S. and Canadian health spending. They found that 62 percent of the difference between the two countries was attributable to prices and intensity of care, and 38 percent was linked to administrative costs.23Compared with Canada, the United States has 44 percent more administrative staff, and U.S. physicians dedicate about 50 percent more time on administrative tasks.24 Inflated to current dollars and today’s population, Pozen and Cutler’s estimate of per capita administrative excess in the United States, when compared with Canada, translates into a gap of $340 billion.25
Woolhandler and Himmelstein estimate that the United States currently spends $1.1 trillion on health care administration, and of that amount, $504 billion is excess.26Woolhandler and Himmelstein rely on surveys of physicians’ time use and utilized physician income data to translate the share of time physicians spend on administrative tasks into monetary value; their estimate of excess costs is the difference between U.S. and Canadian administrative spending27 Woolhandler and Himmelstein’s original 2003 article estimated that Canada spent $307 per capita on health system administration, compared with $1,059 per capita in the United States. Assuming this difference is excess requires an assumption that a Canadian-style health care system would achieve an identical level of administrative costs in the United States.
A separate criticism of the original 2003 Woolhandler and Himmelstein estimates, as articulated by Henry J. Aaron, an economist at the Brookings Institution, is that their methodology failed to account for differences in prices.28 Woolhandler and Himmelstein arrive at their national total administrative costs by tallying up costs in each country for items such as rent and salaries. As a consequence, the U.S.-Canada comparison captures not just the differences in the quantity of resources devoted to administration—such as physician time or office space—but also the differences in office rates, wages, and salaries. Taking Woolhandler and Himmelstein’s estimate of total administrative costs as a given and then making standard adjustments for price differences, Aaron argues that the two researchers exaggerated U.S. administrative spending in their 2003 report and that the true portion of excess would be about one-quarter less than what they estimated.
All estimates of administrative costs are inherently sensitive to what portion of health care spending one considers administrative.29 For example, time spent recording diagnosis or prescription information used in billing may also be vital for patient care, allowing medical teams to share up-to-date information or avoid harmful drug interactions. A recent study of an electronic health records (EHR) system estimated that on average, half of a primary care physician’s day is spent on EHR interaction, including billing, coding, ordering, and communication.30 Such tasks, however, can fall into a gray area between administrative and clinical. In a separate study, economist Julie Sakowski and her fellow researchers reported finding varying attitudes among physicians about whether interaction with electronic medical records—a subset of EHR—represented administrative or clinical time. As Sakowski and co-authors wrote, “Some felt they spent extra effort adding documentation that was needed only for billing. Others seemed to feel that nearly all of that information was needed for accurate clinical records.”31
Administrative costs for payers
Within the U.S. system, the share of expenditures that are attributable to administrative costs varies greatly by payer. The BIR costs for traditional Medicare and Medicaid hover around 2 percent to 5 percent, while those for private insurance is about 17 percent.32Some public finance experts, including Robert Book, have argued that the low levels of Medicare overhead are deceptive. Because seniors have relatively high health expenditures, the argument goes, administrative costs make up a relatively small share of their total health care spending. However, Medicare’s per capita administrative expenditures are higher than those in other forms of insurance.33 Even if one compares higher-end estimates of Medicare administrative costs to low-end estimates of costs for private insurance, the gulf between administrative costs for Medicare and private coverage is large.34 Organisation for Economic Co-operation and Development (OECD) data also show that other nations are able to achieve low levels of administrative costs while maintaining universal coverage across all ages of the population.35
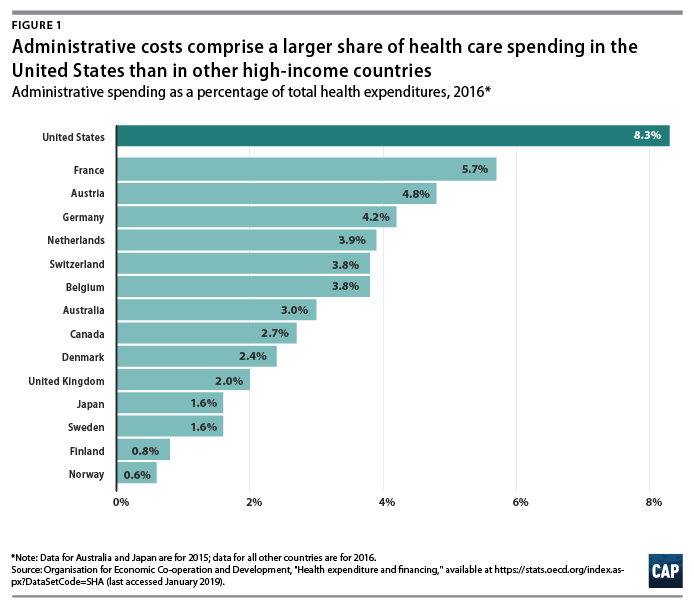
International health system data demonstrate that the United States is a clear outlier on administrative spending. And while the OECD’s definition includes administrative costs to government, public insurance funds, and private insurance, but not those borne by hospitals, physicians, and other providers, the stark difference is still informative. In 2016, administration accounted for 8.3 percent of total health care expenditures in the United States—the largest share among comparable nations. (see Figure 1) Countries with single-payer systems are among those with the lowest administrative costs. For example, administrative spending accounts for just 2.7 percent of total health care expenditures in Canada.36 OECD data also show that within a country, administrative costs are higher in private insurance than in government-run programs.37
Countries that have multipayer systems with stricter rate regulation also achieve much lower administrative costs than the United States. Administrative expenditures account for 4.8 percent of total health care expenditures in Germany, 3.9 percent in the Netherlands, 3.8 percent in Switzerland, and 1.6 percent in Japan, according to the OECD. If the United States could reduce administrative costs down to Canadian levels, it would save 68 percent of current administrative expenditures; reducing to German-level administrative costs would save 42 percent of current administrative expenditures. However, to assume that by simply adapting another country’s health care system—whether it is Canada’s single-payer Medicare, Germany’s sickness funds, or Switzerland’s heavily regulated private plans—the United States would automatically achieve the same level of administrative costs may ignore other fundamental differences between countries, including the market power of health care providers, political systems, and attitudes toward health care. Nevertheless, the experience of other multipayer systems such as those in Germany and Switzerland suggests that the United States could substantially reduce both administrative expenditures and overall health care spending by bringing down reimbursement rates and regulating insurance—even while continuing to allow multiple payers and private health care providers.
The lowest possible level of administrative spending for the U.S. health care system is not necessarily the optimal level of spending. As researchers Robert A. Berenson and Bryan E. Dowd have noted, administrative spending in Medicare may in fact be too low; the program would be more efficient with greater investment in initiatives to lower costs and improve quality.38 Many reforms that could generate overall savings require administrative resources to design and implement. Innovations such as bundled payments—the practice of paying providers a lump sum for an episode of care such as a knee replacement or childbirth rather than reimbursing each individual component—involve upfront investment in development. Increasing resources to combat fraud and abuse would also lower overall spending. While the U.S. Department of Health and Human Services (HHS) boasts that it sees a $5 return on every $1 it puts toward fraud and abuse investigations, that number indicates that the government may be underinvesting in those efforts.39
Administrative costs for health care providers
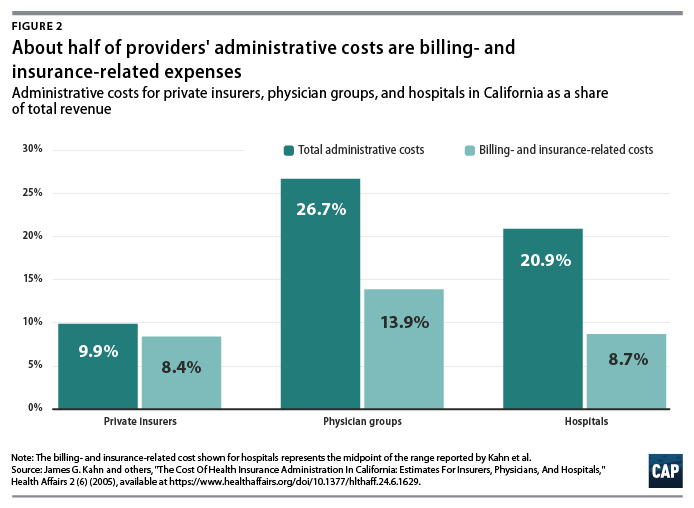
A number of studies have focused on the administrative costs borne by providers. Beyond BIR expenses, hospitals, physician practices, and other health care institutions house departments that are complementary to clinical services such as medical libraries, public relations, and accounting.40 A study of administrative costs in California found that administrative costs represented about one-quarter of physician revenue and one-fifth of hospital revenue, and BIR costs accounted for roughly half of administrative expenditures for physician and hospital services covered by private insurance.41 (see Figure 2) In a separate study, Himmelstein and others reported that one-quarter of U.S. hospital spending went toward administration; they found little difference between nonprofit hospitals and for-profit institutions, where administrative spending was 25 percent and 27.2 percent of total spending, respectively.42
On a per-encounter basis, BIR costs vary as a proportion of overall cost depending on the type of visit. In a 2018 study of an academic health care system, Phillip Tseng and others found that professional billing costs amounted to $20.49 for a primary care visit, $61.54 for an emergency department visit, and $124.26 for a general inpatient stay.43 Relative to the professional revenue associated with each encounter studied, the emergency department visit ranked the highest, with billing costs equal to 25.2 percent of revenue. Inpatient visits were the lowest, at 8 percent of a general inpatient stay and 3.1 percent for inpatient surgery.44 Encounters involving hospital care incurred additional facility-level billing costs. (see Figure 3)
In addition to the dollar cost of BIR activity, the study also reported the time spent on administration for typical encounters. The average processing time was 13 minutes for a primary care visit, 32 minutes for an emergency department visit, and 73 minutes for a general inpatient stay.45
Among other research on provider BIR costs, a 2009 study by Larry Casalino and others estimated that the cost of the time physicians spend on interactions with health plans is about $23 billion to $31 billion per year.46 A 2011 study by Dante Morra of the University of Toronto and others estimated that interaction with payers costs the equivalent of $22,205 per physician annually in Canada and $82,975 per physician annually in the United States, suggesting that the United States would save $27.6 billion annually if U.S. administrative costs could be brought down to Canadian levels.47
As with BIR costs, provider administrative costs in the United States are higher than those in other comparable countries. Hospital administrative costs in the United States far exceed those of other nations. In their comparison of hospital administrative costs among eight Western nations, Himmelstein and co-authors found that the United States had the highest levels, at 25.3 percent of total hospital expenditures.48 They conclude that in nations where hospital administrators have minimal responsibilities for procuring financing and where the hospital reimbursement system is least complex, administrative costs can be reduced to 12 percent of expenditures.49 These findings suggest that reforms that introduce global budgeting or limit the need to bargain with multiple payers could potentially bring down excess hospital administrative costs in the United States.
Lower administrative costs in single-payer and multipayer systems
Although administrative costs contribute to the high expenditures in the United States, they are not the primary reason for the health care spending gap. As economist Uwe Reinhardt and others candidly put it, “It’s the prices, stupid.”50 The United States pays more for care than other countries do—both for administrative services and for other components of health care.
Policies that target administrative costs alone would not necessarily bring overall U.S. health care expenditures in line with other countries. As economists Sherry Glied and Adam Sacarny observed, “there are very substantial variations in administrative costs among countries with universal health insurance, which do not translate directly into variations in overall costs.”51Comparative evidence from U.S. states also suggests that America’s multipayer system explains some, but by no means all, of the discrepancy between the United States and other developed nations. Harvard University researchers Joseph P. Newhouse and Anna Sinaiko observe that “there is considerable variation across the states in spending levels, with the lowest quintile of states spending approximately the same percentage as the higher spending OECD countries other than the U.S. This implies that the [United States’] pluralistic financing system may not be an important cause of the large percentage of GDP that the U.S. devotes to health care.”52
Systemwide reforms to lower administrative costs
Health care financing experts believe that changes to how Americans pay for coverage could dramatically reduce administrative costs. Researchers simulating the effects of single-payer programs have assumed that administrative costs would be brought down substantially. The Urban Institute set administrative costs at a “plausible” 6 percent of health care claims for their simulation of the single-payer plan proposed by Sen. Bernie Sanders (I-VT), noting that they “do not believe that administrative costs can fall far below this level; far too many administrative functions must be conducted.”53 In its analysis of a single-payer system for New York state, the RAND Corporation assumed administrative costs at 6 percent of total health expenditures in its base case, representing a reduction from 18 percent among commercial insurers and 7 percent in New York’s Medicaid program. RAND specified administrative costs at 13 percent and 3 percent in its alternative scenarios. 54 In a separate column, however, RAND researcher Jodi Liu cautioned that achieving the administrative expenditure levels of other countries “may be aspirational and is not guaranteed” under a single-payer system.55
Exactly how such lower costs could be achieved is another question. Reducing BIR costs requires simplifying the billing and payment process, which could be accomplished in a number of ways. Two avenues for reducing administrative costs as well as overall health costs are global budgeting and uniform rate-setting.56 These two concepts are central to health systems around the world and are also responsible for keeping administrative costs lower, whether a country has a multipayer or single-payer system. Another paperwork-reducing option would be a centralized claims clearinghouse to allow providers to submit all claims to a single entity, as they do in Germany and Japan. 57
All-payer rates and global budgeting
Setting all-payer reimbursement rates would eliminate the need for providers to negotiate rates with individual private insurers, while also giving policymakers better leverage for controlling overall health care cost growth. In the current U.S. system, providers charge different rates to different payers, and the billing process is complicated and opaque. The list prices that hospitals are now required to publish bear little connection to what individual patients—or those patients’ insurers—actually pay.58 Setting all-payer rates would simplify billing and improve transparency by establishing a single set of rates for each provider, while also giving regulators a tool to protect consumers from exorbitant rates.59
Global budgeting—the practice of paying providers revenue based on their expected costs—also holds promise for both lowering administrative spending and overall costs. As opposed to traditional fee-for-service payments, which reward providers for doing more, global budgeting incentivizes providers to deliver care more efficiently.60 Global budgeting is a feature of many countries with much lower health care administrative costs, including Scotland, Wales, and Germany.61 As Woolhandler, Campbell, and Himmelstein point out in their 2003 article, “The existence of global budgets in Canada has eliminated most billing and minimized internal cost accounting, since charges do not need to be attributed to individual patients and insurers.”62 As Germany shows, both single-payer and multipayer systems can use global budgets.
A system combining all-payer rates and global budgeting is already partially in place in the state of Maryland, where each hospital has a single set of rates it bills to Medicare, Medicaid, commercial insurers, and other payers. Maryland’s system is keeping overall cost growth lower than the national trend.63 According to RAND analysis of hospital costs, Maryland hospitals have administrative costs that are 9 percent lower than the national average and not far off from the 13 percent savings RAND assumed providers would achieve under a single-payer system. 64
Centralized claims processing
Germany and Japan both have multiple payers but centralized claims processing.65Despite having more than 3,000 health plans,66 Japan’s administrative expenditures were a stunningly low 1.6 percent of overall health care costs in 2015, one of the lowest among OECD member nations.67
In their analysis of three universal health care options for Vermont, including single payer, researchers William C. Hsiao, Steven Kappel, and Jonathan Gruber estimated substantial savings from administrative simplicity from each option. The two single-payer options they examined would result in even greater administrative savings of between 7.3 percent and 7.8 percent, depending on the rate-setting mechanism.68 The group estimated that a third scenario, which would establish a centralized claims clearinghouse while allowing multiple payers, could generate savings equal to 3.6 percent of total expenditures.69This suggests that about half of the total administrative savings from a single-payer system could be obtained within a regulated multipayer system.
Policy proposals directed at administrative costs
While major changes to the U.S. health care system have the greatest potential to bring down costs, more incremental changes could reduce administrative waste. A recent bill proposed by Sens. Bill Cassidy (R-LA) and Tina Smith (D-MN) would direct the HHS secretary to set goals to cut “unnecessary costs and administrative burdens” throughout the health care system by 50 percent over the next 10 years. It would also provide grant money for state-based efforts to bring down administrative costs.70Some possible avenues for achieving those kinds of reductions include changes to payment rules, improvements to facilitate electronic record-keeping and information exchange, and simplification of public insurance programs.
In their 2009 article in TheNew England Journal of Medicine, David Cutler, Elizabeth Wikler, and Peter Basch proposed one such package of reforms. The authors estimated that providers could save $17.9 billion to $23 billion annually with several, more incremental changes to the system, including greater adoption of EHR systems; integrated administrative and clinical systems; national and standardized reporting requirements and credentialing of providers; streamlined enrollment in public insurance programs; and greater automation.71 In a separate report, the same authors proposed additional reforms that they estimated could reduce excess administrative costs by $40 billion, or 25 percent of total health care expenditures.72
In a 2010 study published in Health Affairs, Bonnie B. Blanchfield and other Massachusetts researchers concluded that the administrative burden on physician organizations could be reduced by a “single transparent set of payment rules for a system with multiple payers.” The authors recommended that the United States adopt “a standard set of payment requirements, increased payment-rule transparency, standardized forms, and a standard set of data exchange requirements.” Doing so could save $7 billion in billing costs for physician and other clinical services, according to the authors’ estimates.73
Conclusion
Although estimates vary, a large body of evidence shows that the United States is spending about twice as much as needed on the administration of health care. Other nations enjoy world-class health care systems while spending a fraction of what the United States does on governance, billing, and insurance.
A structural overhaul of how health care is financed and priced that includes key features of other countries’ systems—whether one payer or many—would go a long way toward eliminating excess administrative costs. Simplifying the payment system should be an essential part of future health reform and would make the U.S. system work better for taxpayers and patients alike.
The former director of outreach programs at Larkin Community Hospital in South Miami, Fla., was sentenced to 15 months in prison April 3 for her role in a $1 billion healthcare fraud scheme.
Four things to know:
1. The judge handed down the sentence just over two months after Odette Barcha pleaded guilty to conspiring to defraud the federal government and paying and receiving healthcare kickbacks.
2. Ms. Barcha was one of three defendants charged in an indictment unsealed in July 2016. She allegedly had physicians at Larkin Community Hospital discharge patients to skilled nursing homes and other facilities owned by Philip Esformes, who allegedly paid kickbacks for those admissions.
3. Prosecutors allege Mr. Esformes, who operated a network of more than 30 skilled nursing homes and assisted living facilities in Florida, admitted Medicare and Medicaid beneficiaries to the facilities even if they did not qualify for skilled nursing home care or for placement in an assisted living facility. Once admitted, the patients received medically unnecessary care that was billed to Medicare and Medicaid.
4. The seven-week trial of Mr. Esformes wrapped up March 29, according to the Miami Herald. On April 5, a federal jury found Mr. Esformes guilty of various counts, including paying and receiving kickbacks, bribery, money laundering and obstruction of justice, according to Law360.
Medicare Advantage (MA) plans got a better-than-anticipated pay hike this week, as the Centers for Medicare & Medicaid Services (CMS) released its final 2020 policy and payment updates for the private coverage program for seniors. MA payments will increase by an average of 2.53 percent in 2020, higher than the 1.59 percent initially proposed by CMS earlier this year, reflecting CMS’s expectation that MA services will grow faster than it initially thought.
With the announcement, CMS is also finalizing plans to allow reimbursement for supplemental, non-clinical services covered by MA plans, such as transportation, nutrition support, and housing improvements, as long as those services are intended to improve health status. The final update also confirms CMS’s intent to continue updating its risk-adjustment methodology to more accurately reflect the intensity of services delivered to beneficiaries, a change that has been controversial among insurers, who fear the new methodology will result in lower payments from the government.
Despite these concerns, shares of MA insurers traded higher after the CMS announcement, and health plans will no doubt be pleased with yet another year of good news from CMS on MA rates. Given continued strong enrollment growth, robust rate increases, and a pipeline of millions of aging Baby Boomers poised to become eligible for Medicare, large insurers (and increasingly, providers) will view MA as their primary source of growth for the next decade or more.
CMS and other health insurers are using the program to deliver innovative and unique value to customers, both in terms of cost and quality.
Today’s Medicare Advantage plans are flourishing and the Silver Tsunami is among the reasons.
“Over the last four years, Medicare Advantage enrollment increased by more than 30 percent, while the number of people eligible for Medicare grew by about 18 percent,” said Steve Warner, vice president of Medicare Advantage Product for UnitedHealthcare Medicare and Retirement.
Other reasons for the growth: Innovative models from big insurers and upstarts alike that improve care for health plan members and drive revenue for payers as they look beyond fee-for-service.
IT STARTS WITH THE CONSUMER
Consumers are finding unique value in MA, both in terms of the quality of care and in the financial value.
Medicare Advantage, in fact, makes it easier for consumers to navigate the healthcare system and choose providers, in a way that traditional Medicare does not, said those interviewed.
“Actually it’s pretty hard to navigate the healthcare system on your own,” said Tip Kim, chief market development officer at Stanford Health Care. “Most Medicare Advantage plans have some sort of care navigation.”
Warner of UnitedHealth’s Warner added that Medicare Advantage also offers value and simplicity.
“It provides the convenience of combining all your coverage into one plan so you have just one card to carry in your wallet and one company to work with,” Warner said. “Most plans also offer prescription drug coverage and additional benefits and services not available through original Medicare, including dental, vision and fitness.”
REBRANDING FOR THE NEW ERA
MA plans did not emerge out of thin air. By another name, Medicare Advantage is managed care, a term that was the bane of healthcare during the height of HMOs in the 1980s.
“Medicare Advantage has rebranded ‘managed care’ to ‘care coordination,'” said consultant Paul Keckley of The Keckley Report. “Humana and a lot of these folks have done a pretty good job. Coordinating care is a core competence. Managed care seems to be working in this population.”
MA came along at the right time for CMS’s push to value-based care.
“I would suggest on the providers’ side, embracing Medicare Advantage is an opportunity to get off the fee-for-service mill,” said Jeff Carroll, senior vice president of Health Plans for Lumeris, which recently paired with Stanford Health Care on the Medicare Advantage plan, Stanford Health Care Advantage.
“Provider-sponsored Medicare Advantage plans are a way to put teeth into an accountable care organization,” Keckley added. “Medicare Advantage success is a silver tsunami among major tsunamis. Obviously it’s a profitable plan for seniors and profitable for underwriters. The winners in the process will get this to scale.”
MA is an innovative model that is not a government-run system, but a privately-run system essentially funded by the government.
PAYERS IN THE MA GAME
UnitedHealthcare has the largest MA market share of any one insurer. Twenty-five percent of Medicare Advantage enrollees are in a UnitedHealthcare MA plan, followed by 17 percent in Humana, 13 percent in a Blue Cross Blue Shield and 8 percent in Aetna, according to the Kaiser Family Foundation.
Numerous insurers, in fact, have gotten into the MA market, including Clover Health in San Francisco, a five-year-old startup which has Medicare Advantage as its only business.
Clover is a tech-oriented company that boasts machine learning models that can accurately predict and identify members at risk of hospitalization.
Because Clover focuses only on MA, it can do a better job at problem solving the needs of an older population, said Andrew Toy, president and CTO of Clover Health.
“The problems we face in Medicare Advantage are very different from a younger generation,” Toy said.
Forty percent of the older population is diabetic. Most seniors will be dealing with a chronic disease as they get older.
In other insurance, whether its individual or commercial, the lower cost of the healthier population offsets the cost of the sicker population. MA has no way to offset these costs. Plans can’t cherry-pick consumers or raise premiums for a percentage of the population.
What MA plans can do is design plans that fit the varying needs of the population. A plan can be designed for diabetics. For younger seniors or those not dealing with a chronic disease, a plan can be designed that includes a gym membership.
“All these plans are regulated,” Toy said. “We have the flexibility to move dollars around. We can offer a higher deductible plan, or a nutrition plan. The incentives for us in Medicare Advantage are different than the incentives in Medicare. CMS has explored giving us more leeway for benefits. Consumers have a choice while still having the guarantees of Medicare.”
Toy believes regular Medicare is more expensive because MA offers a more affordable plan based on what an individual needs.
“When you need it, we get more involved in that care,” Toy said, such as “weight control issues for diabetics.”
The drawbacks are narrower networks, though Toy said Clover offers an out-of-network cost sharing that is pretty much in line with being in-network.
UnitedHealthcare’s Medicare Advantage LPPO plans offer out-of-network access to any provider who accepts Medicare, Warner said.
UnitedHealthcare also offers a wide variety of low and even zero-dollar premium Medicare Advantage plans and annual out-of-pocket maximums, Warner said. By contrast, original Medicare generally covers about 80 percent of beneficiaries’ healthcare costs, leaving them to cover the remaining 20 percent out-of-pocket with no annual limit.
“From a consumer value proposition, it makes Medicare Advantage a better deal,” Kim said. “One is Part B, 20 percent of an unknown number. Knowing what the cost will be in a predictable manner is a preferable manner.”
Stanford Health Care launched a Medicare Advantage plan in 2013. Lumeris owned and operated its own plan, Essence Healthcare, for more than eight years. Stanford and Lumeris partnered on Stanford Health Care Advantage in northern California, using Lumeris technology to help manage value-based reimbursementand new approaches to care delivery through artificial intelligence-enabled diagnostic tools and other methods.
“We are not a traditional insurance company,” Kim said. “We’re thinking about benefits from a provider perspective. It’s a different outlook than an insurance company. By definition we’re local.”
MA MARKET STILL HAS ROOM TO GROW
While the Medicare Advantage market is competitive, it is also under-penetrated, Brian Thompson, CEO for UnitedHealthcare Medicare & Retirement, said during a 2018 earnings report.
Currently, about 33 percent of all Medicare beneficiaries are in an MA plan, he added, but UnitedHealth sees a path to over 50 percent market concentration in the next 5-10 years.
It’s a path not so subtly promoted by the Centers for Medicare and Medicaid Services.
As a way to encourage insurers to take risk and get in the market, around 2009, CMS gave MA insurers 114 percent of what it paid for fee-for-service Medicare. The agency began decreasing those payments so that by 2017, traditional Medicare and MA became about even.
MA insurers instead thrive on their ability to tailor benefits toward wellness, coordinate care and contain costs within the confines of capitated payments, the essence of value-based care.
They have received CMS support in recent rate notices that gives them the ability to offer supplemental benefits, such as being able to target care that addresses the social determinants of health. Starting in 2020, telehealth is being added to new flexibility for these plans.
WHAT THE FUTURE MAY HOLD FOR MA
Medicare Advantage plans have expanded and, in so doing, opened innovative new options for plans and their customers alike at the same time that the ranks of people eligible for Medicare continues to swell.
So where is it all going?
Medicare Advantage is changing the way healthcare is paid and delivered to the point that Keckley and Toy agreed the future may not lie in Medicare for All, but in Medicare Advantage for all.
“I think a reasonable place to end, is in some combination where the government is involved in price control, combined with the flexibility of Medicare Advantage,” Toy said. “That’s really powerful.”
Potential Medicare expansion plans would drastically impact the financial standing of health systems, though some may be more pragmatic solutions than others.
KEY TAKEAWAYS
Implementing Medicare for All as a single payer healthcare system is estimated to create a 22.1% negative impact on a mid-size regional provider’s net margin.
However, a voluntary buy-in plan, also known as ‘Medicare for more,’ might result in only a slight dip to the net margin compared to the status quo.
Regardless, some amount of legislative action regarding Medicare expansion will be necessary in the next five years, according to the study’s authors.
Fresh off the 2018 midterm elections where healthcare played a critical role in the electoral shift that saw Democrats retake the House of Representatives, 2020 presidential candidates are heralding sweeping policy proposals to expand coverage through Medicare.
While several versions of Medicare for All legislation exist, other policy proposals such as ‘Medicare for more’ or the public option have drawn consideration from lawmakers as potentially more viable or pragmatic solutions to America’s healthcare problems.
In its analysis, Navigant found a medium-sized, nonprofit, multi-hospital system with revenues of more than $1 billion and a current operating margin of 2.3% would endure vastly different financial implications under several proposed federal healthcare policy changes.
Medicare for All would reduce revenues by around $330 million, a margin drop of just over 22%, the public option proposal would cause revenue declines in the neighborhood of $153 million, a margin impact of -6.3%, and the ‘Medicare for more’ expansion plan is estimated to have a neutral impact compared to the status quo.
Still, Navigant’s study points out that if Congress does not act on Medicare expansion until after the next presidential election, hospitals could face a scenario with a financial impact comparable to the public option proposal.
Using the model health system as an example, status quo projections without any cost reduction initiatives would see the organization’s net margin decline from 2.3% to negative 6.2% from 2018 to 2023, with operating costs rising between 4.5% to 5% per year and revenues growing at 2.5% to 3% per year.
“There’s going to be a need to control hospital cost structures going forward, regardless of whether it’s in the status quo with baby boomers aging into Medicare and payer mix shifts occurring, or in a scenario that has limited expansion, moderate expansion, or robust Medicare for All,” Jeff Leibach, director at Navigant, told HealthLeaders in an interview. “There are obviously varying degrees of impact on hospitals, but all of them are going to require a level of attention and and management of revenue strategy and cost structure that I think hospital CFOs are struggling with today and will benefit from through continued focus on performance improvement and revenue strategy.”
PLANS, DETAILS, AND IMPACT:
‘Medicare for more’
Voluntary buy-in at age 50 and over
In one scenario, choice between employer coverage and Medicare
No Medicare payment relief
No reduction in revenue cycle management operations compared to the status quo
15% reduction in current disproportionate share hospital payments
Public option
All lives covered regardless of age
Choice between employer coverage and Medicare
Range from no Medicare payment relief to payments at 110% of Medicare rate
1.5% reduction in revenue cycle management operations compared to the status quo
70% reduction in current disproportionate share hospital payments
Medicare for All
All lives covered regardless of age
Single payer healthcare coverage
Range from no Medicare payment relief to payments at 120% of Medicare rate
2.5% reduction in revenue cycle management operations compared to the status quo
100% reduction in current disproportionate share hospital payments
Leibach said that the analysis arrives at the early part of the conversation surrounding widespread Medicare expansion at the federal level, which makes it difficult to gauge how health system leaders will react to Navigant’s findings.
Some may be hesistant to support plans that are projected to create such a negative material impact on their respective bottom lines, but others may be willing to consider a policy proposal that significant decreases or even eliminates bad debt costs associated with a large uninsured population.
Even before the report was released, however, the American Hospital Association declined to voice support for Medicare for All late last month.
Leibach added that he was surprised by the “nominal impact” of the voluntary buy-in plan, arguing that could hospital leaders may rally around that proposal as a compromise to expanding Medicare without fully deteriorating their financial standing.
This approach would also be the least disruptive to the commercial insurance market, according to Leibach, assuming that the Medicare for All proposal would be a true single-payer platform that eliminates private insurers.