There are a lot of eye-popping statistics that capture the burden high health care costs put on so many Americans. Nearly three in 10 adults say they have problems paying medical bills. More than 40% say they skip medications because of the cost.
The stat that always stops me in my tracks is the fact that Americans have nearly $200 billion in unpaid medical bills in collections,according to one recent estimate. The average consumer facing collections in 2020 had more medical debt than all other sources of debt — credit cards, phone, utilities — combined.
“If a debt collector is calling you up or is knocking on your door, more than half of the time, it’s for medical debt,” said Neale Mahoney, a Stanford University economist and one of the nation’s leading scholars on medical debt.
Mahoney has spent two decades studying the scale of the country’s medical debt problem, as well as the effectiveness of policies intended to relieve people’s medical debt. From 2022-2023, he worked in the Biden administration on regulations to remove unpaid medical bills from people’s credit reports.
We talked with Mahoney about the fate of those regulations under the Trump administration, and what we’ve learned about the best way to protect people from getting medical debt in the first place.
Here are a few of the takeaways:
The Trump administration is rolling back Biden’s regulation of medical debt. Credit agencies sued to prevent the federal government from banning overdue medical bills from credit reports, and the White House declined to defend it. New guidance under Trump also challenged state protections for medical debt.
Nonprofits — and some local governments — have paid off medical debt for millions of Americans, in hopes of easing stress and improving people’s health. Mahoney’s research points to bigger improvements in health outcomes for patients who got debt relief sooner rather than later. One recent study showed patients who got their bills cleared within a few weeks of getting care were more likely to get diagnosed and treated for heart disease and diabetes than those who didn’t get help. However, an analysis of people who had their debts wiped after carrying them for years found no improvements to self-reported physical or mental health.
Mahoney believes helping patients avoid medical debt through health insurance or hospital financial assistance, which wipes out some or all of a patient’s bill, is the most effective approach. Many people, however, struggle to take advantage of either due to obstacles like restrictions from insurers and extensive applications to get help from hospitals. Patients caught up in what Mahoney has dubbed “the annoyance economy” often end up in money-losing fights. “For too many of us, navigating the U.S. health care system can feel like a second job,” Mahoney said, “at the precise moment when we don’t have the time and energy to take on a second job.”
One promising option to prevent people from falling into medical debt, Mahoney said, is for hospitals to auto-enroll eligible patients for financial assistance — a process known as “presumptive eligibility.” California, Illinois, Oregon and North Carolina have adopted auto-enrollment requirements for hospitals, and more states are considering it. “I would be eager to see hospitals working on this and sharing best practices,” Mahoney said, “so that we can provide relief to people who need it while still recovering payments from people who can afford it.”
One of those reasons is the growing number of states looking to require hospitals to auto-enroll patients in financial assistance programs. I’ve been reporting on this idea of presumptive eligibility for years, and for the last few months, I’ve been working on a special series diving deep into the pros and cons of forcing hospitals to provide more charity care. Those stories will drop this fall.
The Federal IDR Operations final rule introduces vital changes to fees, batching, and eligibility, but a lack of federal enforcement leaves providers battling payers for post-decision payments.
KEY TAKEAWAYS
The final rule slashes administrative fees and relaxes batching constraints to make pursuing lower-dollar claims much more financially viable for providers.
Payers must now provide essential claim details upfront to streamline eligibility determinations and reduce administrative friction.
Revenue cycle leaders should advocate for legislative action to hold payers accountable because the new rule lacks mechanisms to enforce post-decision payments.
While there is a significant administrative lift that comes with navigating the Federal Independent Dispute Resolution (IDR) process comes with a heavy administrative lift, the system has proven to be a significant driver of recovered revenue for providers.
To address operational friction for all parties, federal regulators have finalized the Federal IDR Operations rule. This update includes adjustments designed to standardize data, clarify timelines, and streamline the process.
For revenue cycle leaders, understanding these updates is essential to maintaining compliance and optimizing cash flow without adding unnecessary overhead.
Open Negotiation and Communication
The final rule mandates that all parties use the federal open negotiation portal to initiate the dispute process.
This requires providers to submit standardized data elements, creating a uniform communication channel. By centralizing the exchange, regulators aim to move away from the chaotic web of emails and spreadsheets that have often complicated early-stage resolutions.
Clarifying Eligibility
Determining IDR eligibility has been a time-consuming step for revenue cycle teams, but the final rule shifts more responsibility to payers.
Payers must now provide essential claim details at the time of the initial payment or denial. This includes the Qualifying Payment Amount (QPA) and specific remittance codes indicating whether a claim falls under state or federal jurisdiction. This upfront transparency allows providers to accurately assess eligibility before committing resources to a dispute.
Reducing IDR Fees
Perhaps most notably, the final rule reduces the non-refundable administrative fee to just $15 per party, per dispute. This represents an 85% drop from the previous $115 rate.
While the final rule establishes that these fees will now be collected earlier in the workflow to maintain system capacity, the lower financial barrier to entry makes it far more viable for providers to pursue arbitration for lower-dollar claims. Ultimately, this allows revenue cycle teams to seek out-of-network reimbursements without the fear that the administrative cost of the dispute will eclipse the potential recovery.
Revamped Batching Rules
New batching rules will help providers to more efficiently manage IDR costs and consolidate efforts by relaxing previous constraints and offering clearer guidelines for grouping claims.
Providers can now batch items and services billed under the same or similar service codes. To qualify, these claims must involve the same provider and the same payer, and they must have occurred within a specified 30-day window.
Enforcing the Cooling-Off Period
The NSA originally established a 90-day cooling-off period following a final determination to help manage dispute volumes.
The final rule explicitly clarifies how this timeline is triggered and applied. Providers cannot continuously submit the same disputed item or service code for the same payer once a determination is made. Revenue cycle teams will need to refine their internal tracking processes to ensure compliance with the cooling-off window and avoid administrative dismissals.
Will Payers Play Nice?
While the final rule clarifies details of the IDR process, it neglected to address comments from providers calling for an enforcement mechanism. Health systems are increasingly winning their IDR cases, only to find that payers are simply refusing to remit the owed amounts, according to Kathy Stull, manager of revenue cycle and analytics for HFMA.
“Instead of even getting the incorrect payment, they’re not going to pay anything,” Stull noted during the recent HFMA Region 1 Annual Conference.
If payers fail to make post-decision payments, revenue cycle leaders and health system government relations teams should advocate for H.R. 4710, a proposed bill that would impose civil monetary penalties on insurers for every instance they fail to pay following an IDR loss.
Hospital monopolies get the headlines – but new research shows health insurance markets are highly concentrated in every state, giving insurers more pricing power than most policymakers realize.
Hospital consolidation dominates the discussion on health care costs – with good reason. There is overwhelming evidence that it raises prices. But every hospital must ultimately negotiate rates with insurers, yet the consolidation story in the health insurer market has only gotten a tiny fraction of the attention. This is a mistake. While the insurer market is not as highly consolidated as the hospital market, it is still highly concentrated by any reasonable antitrust standard, and a major (and under-estimated) driver of cost growth.
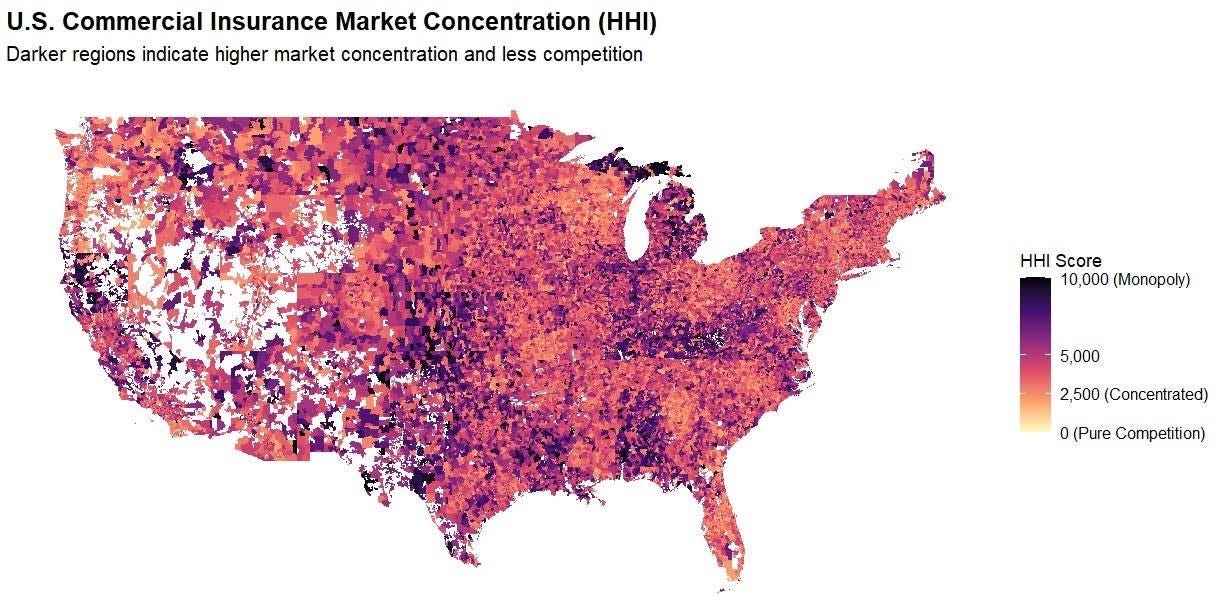
The Department of Justice (DOJ) and Federal Trade Commission (FTC) use the Herfindahl Hirschman Index (HHI) to measure market concentration, where >1,800 is highly concentrated, 5,000-7,500 is where a few firms hold substantial market power, and >7,500 is a near monopoly, where a single firm holds absolute (or near absolute) price-setting autonomy. The hospital market is heavily concentrated and has an average HHI score of 5,273, with 97% of markets being at least heavily concentrated and 64% being near or complete monopolies.
By comparison, our recent work similarly shows a high degree of consolidation among insurers. (Figure 1) We found that the state-level average HHI score in the commercial insurance market was 4,458, with 50 of 50 states (100%) at least heavily concentrated, comparable to hospital markets. This means that in almost every state, health insurers hold pronounced power in price-setting, a key component of the health care cost crisis roiling the country. The most competitive states (although still very highly concentrated) were Oregon (2,870), New York (3,203), and Georgia (3,222), whereas Kentucky (6,752) and Alabama (6,988) are near monopolies.
We find that insurers are even more consolidated than previously reported by the American Medical Association (AMA). Yet the market power of insurers, in combination with hospitals, is a vastly under-appreciated and under-studied driver of costs.
There are several reasons why it is important.
1. Vertical integration
Vertical integration is rapidly accelerating the ability of insurers to consolidate power and redefining what an insurer even is (UnitedHealth/Optum, CVS/Aetna, Cigna/Express Scripts, Elevance/Carelon, BCBSA/Ascendiun). This means that traditional plan-level data (such as that used by researchers and the DOJ/FTC) underestimates the true market power of insurers, and the shadowy network of MSOs, banks, and vendors makes it very difficult to quantify, absent new reporting or regulatory requirements
2. Geography
Where you live is important since it determines where you receive care and buy insurance. In some states, the average competition tells the story, e.g. Louisiana, Kentucky, Alabama, since certain insurers dominate the metro areas and everything in between. In others, the reassuring state averages (CA, NY) mask the variance, and hide the pockets of very uncompetitive markets, particularly in rural areas. Understanding this issue at a market level is important for creating transparency and accountability, to ensure that everyone has options and access to affordable health insurance.
3. Competition
Competition among insurers and hospitals matters, as power asymmetry and/or collusion create dysfunctional markets where costs are “optimized” for the purposes of power and profits, not to make health care more affordable for consumers. It is also important to look at competition among insurers. Market dominance confers advantages that have little to do with delivering better care, such as leverage over providers, captive employer relationships, and pricing power insulated from competition.
While insurer markets aren’t as concentrated as hospital markets, they’re concentrated enough to matter, and the structure of that concentration makes it a distinct and important part of the cost problem. In our next piece, we will show which carriers hold dominant positions and where, and why the answer surprised us.
This research was made possible by the support of Arnold Ventures.
Data from Clarivate Managed Market Surveyor dataset. Includes FI/SI/HMO/PPO/POS/ACA plans.
HHI scores weighted according to zip-level and policy volume. Concentration levels: Red – Extreme; Orange – Severe; and Yellow – Very High.
A Trump administration plan to overhaul wage levels for visa holders is jolting hospitals and long-term care facilities that are heavily reliant on foreign-born workers.
Why it matters:
It’s the latest immigration-related policy change to loom over the health care workforce, coming after President Trump’s $100,000 H-1B visa fee and the suspension of certain immigrants’ work authorization renewals.
The latest move could further drive up costs for providers already struggling with staffing shortages, thin margins and growing patient demand, because many health jobs can’t be outsourced or automated.
Driving the news:
The Department of Labor wants to change the formula for calculating what it considers “fair minimum pay” for workers on certain visas, like H-1Bs, and green card sponsorship jobs.
The administration says the change would make it harder for companies to use visa programs to obtain cheaper labor and undercut American workers.
But the rule could have an outsized effect on health systems, testing labs, nursing homes and research institutions that sponsor foreign-trained workers.
There’s special concern about rural health providers that rely heavily on foreign-born clinicians to fill gaps in care in underserved areas.
Critics say the changewon’t adequately account for regional wage differences or experience levels.
They also warn a higher wage requirement will force employers to raise pay for U.S. workers to comply with labor laws — and make it unsustainable to hire foreign-born talent.
The big picture:
The U.S. health care system is heavily dependent on a foreign-born workforce. Immigrants make up about 16% of registered nurses nationwide, per a KFF analysis.
They make up 28% of the U.S. long-term care workforce, KFF found.
“This has the potential to significantly limit the sector’s ability to provide timely and quality health care services to those in need, both now and in the future,” Dana Ritchie, associate vice president of the American Health Care Association and National Center for Assisted Living, wrote in public comments on the proposal.
Zoom in:
Lynn Bruder, the CEO of staffing firm Nucleus Healthcare, said wage rates for visa-holding nurses on the lower end of the pay scale could jump 25% to 35% in certain markets, or from about $40 an hour to more than $50 an hour.
“The likely outcome is continued reliance on significantly more expensive agency staffing solutions and reduced ability for hospitals to build stable, long term workforce pipelines,” Bruder wrote in comments about the rule.
The other side:
The Department of Labor declined to comment. But visa programs have long been criticized for suppressing wages across many industries.
The changes would force employers to pay an estimated $6.5 billion in additional wages and increase the average certified wage by approximately $14,000 per year, according to the proposed rule.
“These proposed revisions aim to better align prevailing wage levels with the wages paid to U.S. workers,” the Labor Department wrote.
The window for public comments on the proposal closed this week.
The bottom line:
Health care providers say the administration is treating hospitals and nursing homes like any other employer, even though the workforce is being squeezed by an aging population and rising demand for care.
“Larger hospital systems may be able to absorb this increase, but you’ll see employers who are much smaller or mid-sized won’t,” Ann-Rose Johnson-Lewis, director of legal services at WorldWide HealthStaff Solutions, told Axios.
“You’ll see rural heath care systems not be able to absorb that. We’ll see a reduction in the workforce, fewer new hires and, ultimately, the broader economy will see the consequence of that.”
Try making a doctor’s appointment at your primary care provider’s office or an urgent care clinic, and often, it won’t be with an MD or DO. As more people need more care—and as more types of preventative care are available—offices are increasingly relying on nurse practitioners (NPs) and physician assistants (PAs) to see patients and save costs.
That’s not necessarily a bad thing; though they don’t have as extensive training as an MD or DO, both nurse practitioners and physician assistants can deal with many of the complaints someone would have at their primary care office.
“An experienced PA or NP can do most of what a primary care physician does,” says Perri Morgan, a professor in family medicine and community health at Duke University School of Medicine who focuses on PAs and NPs in the health care work force. “And many practices find them to be a welcome addition to the bottom line” because they cost less to employ than physicians.
Nurse practitioners and physician assistants are paid less than doctors are, but in some states they can generate nearly as much income for practices because they can bill at the same rate as doctors, says Dr. David Chan, a professor at the University of California, Berkeley who studies health economics. Doctors make, on average, $239,200 a year, according to the Bureau of Labor Statistics—nearly double what physician assistants and nurse practitioners make.
In 2023, the most recent year for which data are available, there were 340,319 primary care physicians in the U.S., according to the National Center for Health Workforce Analysis. By contrast, there were an estimated 374,970 nurse practitioners and 29,433 physician assistants working in primary care in 2024.
Estimates suggest that in a decade, there will be many more NPs and PAs than MDs and DOs across medicine. While the number of physicians in the U.S. is projected to grow by just 3% between 2024 and 2034, according to the Bureau of Labor Statistics, the number of physician assistants is expected to grow by 20%, and the number of nurse anesthetists, nurse midwives, and nurse practitioners is expected to grow by 35% over that time.
In some states, nurse practitioners and physician assistants must be supervised by a physician to practice. But groups that represent the interests of NPs and PAs are advocating for more independence. They have persuaded many states to pass legislation that allows them to operate without a supervising physician. The American Medical Association, however, has worked to defeat such bills, calling the practice “scope creep” and arguing that it makes patients less safe.
Here’s what patients should know about PAs, NPs, and what you might get from one type of provider vs. another.
What is a nurse practitioner (NP)?
The technical name for a nurse practitioner is an advanced practice registered nurse, or APRN. There are four main types of APRNs: nurse practitioners, certified registered nurse anesthetists, certified nurse-midwives, and clinical nurse specialists.
Nurse practitioners can diagnose and treat illnesses, prescribe medications, manage chronic conditions, order and interpret diagnostic tests, and provide preventative care, says Valerie J. Fuller, president of the American Association of Nurse Practitioners (AANP). Fuller says NPs are unique because they are trained in nursing and so are extremely patient-centered. “I think patients who choose a nurse practitioner are really looking for a clinician who can diagnose, treat, manage their health needs, but who also takes the time to listen,” she says.
To become a nurse practitioner, you need an undergraduate nursing degree and a registered nurse license. Then you must go back to school to pursue a graduate degree: either a master of science in nursing or a doctor of nursing practice. After your graduate degree, you must pass a national certifying exam; only then can you receive an APRN license. (Not all states issue a specific APRN license; some issue similar authorization but call it a certification or registry.)
Nurse practitioners have what’s called full practice authority in 27 states, meaning they can practice without being supervised by a physician. That’s up from just 14 states in 2010. And although some states have passed legislation that requires visits with nurse practitioners to be compensated at the same rate as physicians, that’s not the case in all states. Medicare reimburses nurse practitioners at 85% of what they reimburse for physicians, Fuller says.
Fuller argues that allowing NPs to practice without a physician’s supervision encourages them to open up practices, helping close gaps in care. When Arizona allowed full practice authority, she says, the nurse-practitioner workforce grew by more than 50%. Millions of Americans don’t have access to basic primary care services, she says, and nurse practitioners can step up to help if they’re allowed.
What is a physician assistant (PA)?
Physician assistants came about in the wake of the Vietnam War, when thousands of medics were returning from overseas and looking for a place to fit in the medical field, says Morgan, of Duke. Today, to recognize their independence, the American Academy of Physician Associates (AAPA) is advocating for PAs to be referred to as “physician associates” rather than “physician assistants.”
PAs help fill gaps in medical care, just like NPs do. “They are trained as core generalists,” says Chantell Taylor, head of advocacy at AAPA. “They’re attractive to employers looking to lower wait times and increase patient access, particularly in rural and underserved areas.”
To start a PA program, students must have a bachelor’s degree, complete prerequisite coursework, and enter PA school with more than 3,000 hours of patient-contact experience, Taylor says. PA programs usually last three academic years that include more than 2,000 hours of clinical experience.
That clinical experience includes rotations in family medicine, emergency medicine, surgery, pediatrics, and other specialties, and prepares graduates to evaluate, diagnose, and treat patients across a broad range of medical specialties and practice settings. PAs graduate with a master’s degree—usually a Master of Science in physician assistant studies or a Master of Clinical Health Services—and then must pass the physician assistant certifying exam to receive national certification and obtain a state license.
Some PAs practice in primary care, but others specialize in surgery, oncology, and other areas, assisting doctors and making them more productive, says Morgan. A PA could prep patients for surgery and close a patient up after surgery, for instance, allowing the surgeon to see more patients, she says. “PAs in specialties add at least as much value as ones in primary care,” she says.
The AAPA is advocating for states to lift the requirement that PAs be supervised by a physician; so far, nine states have done so. Five states have passed legislation to change the title of PA from physician assistant to physician associate.
Are NPs and PAs as effective as MDs and DOs?
Patients may be hesitant to see a NP or PA because they have less education and medical training than a doctor. There have been recent reports of poorly trained NPs missing key indicators of illness, most notably in a Bloomberg series about the rising numbers of nurse practitioners.
Both AAPA and AANP say that PAs and NPs are essential to provide care in rural and underserved areas with physician shortages, and that having more non-physicians providing care helps increase access for all Americans. The American Medical Association, on the other hand, says that while it supports the role of non-physicians, “they are not a substitute for physicians,” and that numerous studies show that patients want care led by physicians.
The training differences are stark. Physicians complete four years of medical school plus a three-to-seven year residency program, which can include 12,000 to 16,000 hours of clinical training. Nurse practitioners do not have a residency requirement and have about 500-720 hours of clinical training, and PAs are required to have about 2,000 hours of supervised clinical practice.
“The country is facing a health care workforce shortage, including shortages of both physicians and nurses,” the American Medical Association said in a statement provided to TIME. “One way to alleviate this shortage is by supporting physician-led care teams that leverage the skills of non-physician practitioners while ensuring that all members of the care team work together, under the direction of a physician, toward optimal care for patients.”
What does the research show about the effectiveness of each type of provider? It depends on the study, says Chan of UC Berkeley, who has examined the difference between NPs and physicians in an emergency-room setting. In one study, Chan looked at what happened in emergency rooms when the Veterans Health Administration began allowing nurse practitioners to practice without physician supervision in 2016. His work suggested that NPs ordered more external tests than did physicians, had more patients returning to the ER with infections than did physicians, and were more likely than physicians to prescribe antibiotics. But “the evidence is still kind of limited,” Chan says. Some doctors will have better patient outcomes than some nurse practitioners, but the reverse is true, too.
Other research suggests that both NPs and PAs can be as effective as doctors at taking care of chronic conditions in medically complex patients—and that they can help save money. One study of patients with diabetes seen at the VA found no clinically significant differences in diabetes outcomes of patients seen by a NP, PA, or physician.
Another study of VA patients with diabetes found that the health care costs were about 7% lower for NP and PA patients than patients who saw a physician, because patients who saw a doctor were more likely to use the emergency room and inpatient services. Morgan of Duke, the lead author of that study, speculates that this is because it might be easier for patients to reach their PA or NP than their physician, allowing their provider to help them address concerns or adjust medications quickly without having to go to the emergency room.
What’s most important, experts say, is that NPs and PAs work together with physicians to help fill care gaps and treat patients. Exactly how that team works together is still up for debate. Taylor, of the AAPA, calls the physician-led model “outdated” and argues that it “doesn’t fully leverage all provider types.” The AMA, on the other hand, argues that physician-led, team-based care is higher quality and more cost effective. And both have a number of studies to point to that prove their point.
“Increasingly, health care is about teams,” Chan says. “So the next question is: How do we best organize teams with NPs and doctors and others?”
Presbyterian Healthcare Services’ decision to exit most Medicare Advantage plans and eliminate 150 positions underscores a growing reality for provider-sponsored health plans.
KEY TAKEAWAYS
Rising utilization, reimbursement pressure and regulatory scrutiny are forcing organizations to reassess participation in Medicare Advantage.
Presbyterian’s move reflects a decision to prioritize care delivery and long-term financial stability over maintaining an unprofitable business line.
Financial flexibility and access to capital increasingly depend on demonstrating disciplined balance-sheet management.
Albuquerque-based Presbyterian Healthcare Services has announced it will discontinue most of its Medicare Advantage (MA) offerings beginning in 2027, affecting roughly 30,000 members, while laying off approximately 150 health plan and administrative employees. The system will continue operating its Dual Plus Special Needs Plan serving Medicare-Medicaid beneficiaries. According to Presbyterian, remaining in the broader MA market would limit its ability to invest in care delivery, workforce development and access initiatives across New Mexico. The move is another indication that provider-sponsored health plans are facing mounting pressure as MA margins tighten nationwide.
Many health systems entered Medicare Advantage to create integrated delivery models, diversify revenue streams and capture greater value from population health initiatives. However, elevated medical utilization, changing reimbursement dynamics and increased regulatory oversight have altered the financial equation. Presbyterian’s decision suggests leadership determined that the returns no longer justified the capital and operational resources required to compete effectively in the market.
The regional implications are significant. Presbyterian is one of New Mexico’s largest healthcare organizations, operating hospitals, clinics, physician practices and a health plan across the state. While the layoffs are concentrated in health plan and administrative roles, the exit removes a major local MA option and will require thousands of seniors to seek alternative coverage. At the same time, Presbyterian argues the move will allow it to redirect resources toward direct patient care and workforce investments, potentially strengthening healthcare delivery capacity over the long term.
There’s a larger lesson centered on strategic focus. Organizations often face pressure to maintain market presence across multiple business lines, even when margins deteriorate. Presbyterian’s action demonstrates the importance of regularly evaluating whether each service line advances the system’s long-term mission and financial objectives. Exiting a business can be difficult, but preserving capital for higher-value investments may ultimately create greater organizational resilience.
The decision also highlights why credit ratings deserve ongoing executive attention. Strong ratings are not simply a borrowing metric; they influence an organization’s ability to finance facilities, technology modernization, workforce initiatives and strategic growth. Rating agencies increasingly scrutinize operating performance, liquidity, leverage, governance and management’s willingness to make difficult strategic decisions when market conditions change. Fitch continues to maintain coverage on Presbyterian Healthcare Services, underscoring the importance of external evaluation of health system financial strength.
Healthcare organizations that delay corrective action risk eroding margins, weakening liquidity and increasing borrowing costs. Conversely, systems that demonstrate disciplined portfolio management often preserve stronger credit profiles and maintain greater access to capital during periods of industry disruption.
Presbyterian’s Medicare Advantage could signal a move towards strategic capital allocation, a growing priority in today’s environment. As reimbursement uncertainty and utilization pressures continue across healthcare, CFOs should view the announcement as a reminder that financial sustainability sometimes requires difficult choices today to preserve organizational strength tomorrow.
Issue: The 2025 budget reconciliation law (the One Big Beautiful Bill Act, or H.R. 1) reduces federal funding for Medicaid, Affordable Care Act (ACA) marketplaces, and the Supplemental Nutrition Assistance Program (SNAP) by about $1.3 trillion but adds $50 billion for the new Rural Health Transformation Program (RHTP). Additionally, the ACA enhanced premium tax credits expired on January 1, 2026.
Goal: To estimate the impact of H.R. 1 and the expiration of enhanced premium tax credits on state economies and employment levels, and state and local tax revenues in 2026, the first year of implementation, and 2029, when the legislation is fully implemented.
Methods: We estimate federal funding changes for the RHTP, ACA marketplaces, Medicaid, and SNAP, and use the IMPLAN modeling system to project economic and employment impacts.
Key Findings and Conclusions: We project that in 2026, the RHTP’s modest economic gains will be overshadowed by losses from budgetary cutbacks. The predicted combined national impact is 229,000 job losses, primarily affecting larger and more urban states. By 2029, 1.65 million jobs could be lost nationally, a 1.0 percentage point increase in the unemployment rate. Every state would experience substantial economic and employment losses, driven primarily by large Medicaid cuts.
Introduction
The Rural Health Transformation Program (RHTP), which provides five years of federal funding to help states improve health care access and quality in rural areas, was created through the 2025 federal budget reconciliation law known as H.R. 1 or the One Big Beautiful Bill Act. The law also made sweeping cuts to Medicaid, Affordable Care Act (ACA) health insurance marketplaces, and the Supplemental Nutrition Assistance Program (SNAP).1 Although the net result is deep reductions in health and nutrition funding, the federal deficit will rise by over $3 trillion because of large tax cuts also included in the law.2 H.R. 1 is expected to cause more than 10 million Americans to lose their health insurance due to the ACA and Medicaid reductions, 3 million people to lose food assistance because of SNAP cutbacks, and a potential 51,000 preventable deaths due to Medicaid cuts.3 On January 1, 2026, months after H.R. 1 was signed into law, enhanced premium tax credits for the ACA marketplaces expired, causing ACA premiums to rise steeply and leading to rapid coverage losses.
This brief estimates the economic impacts of these sweeping changes to the health care landscape. Using the IMPLAN economic modeling system, we examine the combined effects of H.R. 1 and the expiration of the ACA tax credits on every state’s economy and employment in 2026, the first year of implementation, and 2029, when the law’s changes are fully implemented (see “How We Conducted This Study”). It builds on earlier briefs that have examined the potential economic effects of the U.S. House of Representatives version of the H.R. 1 legislation and the expiration of the ACA subsidies.4
Timeline and Scale of H.R. 1 Cuts and Expansions
The Congressional Budget Office (CBO) estimated that H.R. 1 will reduce federal Medicaid spending by more than $900 billion between the 2025 and 2034 fiscal years, while federal funding for the ACA marketplaces and SNAP will each be cut by almost $200 billion over the next decade. The RHTP adds $50 billion in funding over the decade.5 The expiration of ACA enhanced premium tax credits means federal funding is about $335 billion lower over a decade compared to if they were extended.6
H.R. 1 changes are phased in, as illustrated in cumulative dollar changes in Exhibit 1 and percentage changes in Exhibit 2. While the RHTP began on January 1, 2026, alongside the expiration of ACA tax credits, Medicaid and SNAP cuts will largely be implemented later. By 2034, cumulative federal Medicaid reductions will total $904 billion, exceeding cumulative reductions in ACA marketplace and SNAP outlays. However, although the dollar amounts lost from Medicaid are much greater, the ACA marketplace and SNAP cuts are deeper when measured as a percentage of their annual baseline expenditures. In 2029, for example, federal Medicaid funding will be cut by 12.7 percent, while ACA marketplace funding will fall by 23.4 percent and SNAP funding by 19.7 percent. Additional losses from the expiration of the ACA enhanced premium tax credits means the combined impacts on the ACA marketplaces are even larger than shown in the exhibit. Key policies changes are summarized in Exhibit 3.
Economic Consequences in 2026: Funding Losses Eclipse Modest Economic Gains
In 2026, we project the RHTP launch and the expiration of ACA tax credits — both beginning in January of this year — to have a largely net negative impact on state economies, jobs, and tax revenues.
Rural Health Transformation Program. Ten billion dollars in RHTP funds have been distributed across 50 states, ranging from $281 million and $272 million for Texas and Alaska to $147 million for New Jersey. State economies, as measured by their gross domestic product (GDP), will be $13.8 billion higher as a result (see Appendix 1). The number of new jobs across the country will likely rise by 110,100, of which 51,600 are health-related, and economic gains will contribute to $847 million in additional state and local tax revenues. Relative gains will be higher in smaller rural states.
ACA health insurance marketplace. In 2026, the expiration of the enhanced premium tax credits and other H.R. 1–related changes will see federal funding for the ACA marketplace fall by $31 billion. State GDPs will fall even more, by $40.7 billion (Appendix 2), while state and local tax revenues will fall by $2.5 billion. This will lead to the loss of 339,100 jobs, of which 154,200 are health-related. Southern states, which generally did not expand Medicaid eligibility, tend to be more reliant on the ACA marketplaces. For example, the ACA cuts will lead to 83,400 jobs lost in Texas and 57,500 in Florida, both nonexpansion states. In comparison, Medicaid expansion states California and Louisiana are expected to lose 20,300 and 7,000 jobs, respectively. Overall, the average expected job loss is approximately 2,800 in expansion states, compared with 22,300 in nonexpansion states.
One potential economic effect not captured in our analysis: those who continue to get coverage through the ACA marketplaces will have to pay hundreds or thousands of dollars more for coverage or shift to ACA plans with higher cost sharing, undermining their financial security and reducing spending power on other goods and services.7
Combined Economic Impacts in 2026
While the infusion of $10 billion into state economies for rural health contributes to some economic growth, it is overshadowed by the $31 billion in federal funding cuts to ACA marketplaces.
Exhibit 4 presents combined national estimates for 2026, including the states with the largest employment losses and the largest employment gains. States with the greatest losses — Georgia, Texas, Florida, South Carolina, Mississippi, Alabama, Tennessee, and Louisiana — are Southern states that rely more on the ACA marketplace. Georgia, Texas, and Florida lose between 30,700 and 79,500 jobs, equivalent to a 0.5 percent to 0.6 percent decline in the employment rate. States with job losses also have substantial reductions in their GDP and state and local tax revenues. States with the largest job increases — Alaska, Vermont, Wyoming, Montana, North Dakota, Rhode Island, Hawaii, and Maine — gain 900 to 2,000 jobs each, equivalent to a 0.3 percent to 0.6 percent increase in the employment rate. States with job gains also will have GDP gains and increased state and local tax revenues (Appendix 3 shows detail for all states in 2026).
Exhibit 5 presents the national map of states gaining and losing jobs. Our analysis indicates that 22 smaller and rural states will have net positive gains and job growth, while the District of Columbia and 28 states, generally larger and more urban, will have net federal funding losses and lose jobs in 2026. Many of the states losing jobs are Southern states that did not expand Medicaid.
Economic, Employment, and Tax Consequences in 2029: All States Will Lose
In 2029, when H.R. 1 provisions are fully implemented, we project that all states will lose federal funding and suffer substantial economic and employment losses.
Medicaid. In 2029, federal Medicaid funding will drop by $90.9 billion, causing state GDPs to fall by $118.5 billion (Appendix 4). Medicaid cuts also mean 996,000 fewer jobs nationwide in 2029, half of which will be health-related, including in hospitals, clinics, pharmacies, or nursing homes. States with the largest job losses include California, New York, Pennsylvania, Illinois, Texas, Arizona, Ohio, and Michigan, which lose between 150,200 and 36,600 jobs. States that expanded Medicaid eligibility under the ACA will likely face deeper losses because H.R. 1 targeted them with policies like Medicaid work requirements, restrictive enrollment procedures, and higher cost sharing only in expansion states. Individual and business income losses will cause state and local tax revenues to fall by $8.8 billion nationwide.
SNAP. Federal SNAP funding will be cut by $21.8 billion in 2029, causing state GDPs to decline by an estimated $18.3 billion (Appendix 5). The SNAP cutbacks will cause 135,500 jobs to be lost in 2029, of which about 75,000 are food-related jobs. Other research has examined SNAP’s importance in supporting revenues and jobs at grocery stores that feed all Americans.8 States with the greatest job losses due to the SNAP budget reductions include California, New York, Texas, Florida, Illinois, Pennsylvania, Michigan, Georgia, and North Carolina, which will lose between 23,000 and 4,200 jobs. Under H.R. 1, states with higher over- and underpayment error rates must pay 5 percent to 15 percent of SNAP benefit costs, leading to drastic reductions in federal payments. The expansion of SNAP work requirements and the halving of federal funding for administrative costs will likely make it harder for states to implement operational changes to lower their error rates.9 State and local tax revenues will decline by approximately $1.9 billion nationwide because of cuts to SNAP.
Combined Economic Impacts in 2029
Exhibit 6 summarizes key results for the combined economic impact of the RHTP and ACA marketplace, Medicaid, and SNAP funding changes. In 2029, RHTP is expected to continue providing $10 billion in federal funding to states, but it will be eclipsed by ACA marketplace losses amounting to over $57 billion. Federal funding for Medicaid will drop by almost $91 billion and SNAP funding by almost $22 billion. Combined, these cuts will total $160 billion (Appendix 6 presents more detail for all states.) Our IMPLAN analyses indicate that these changes will reduce state GDPs by $197 billion in 2029, about 23 percent more than the federal savings due to funding cuts being magnified by the “multiplier effect.”
Overall, there will be 1.65 million fewer jobs in 2029 — almost half of which will be in health care — roughly equivalent to a 1.0 percentage point reduction in the national employment rate. State and local tax revenues will be more than $14 billion lower in 2029.
To illustrate relative losses, Exhibit 6 shows job losses as a percentage of state employment in the eight hardest-hit states, all of which have expanded Medicaid eligibility. The exhibit also highlights states with the largest number, rather than percentage, of jobs lost, ranging from 207,100 in California to 51,000 in Ohio.
Over the next decade, funding cuts and changes to Medicaid, the Supplemental Nutrition Assistance Program, and Affordable Care Act marketplaces through H.R. 1, and the expiration of the ACA enhanced premium tax credits, have the potential to reshape the U.S. economy and health system. The $50 billion funding increase through the Rural Health Transformation Program will not offset the much larger losses in health insurance coverage, decreased access to care, and increased hunger caused by H.R. 1 cuts.
We focused on two years in this brief: 2026, the first year of the law’s implementation, and 2029, when the law’s changes are fully implemented. Economic and employment impacts across states will also occur in 2027 and 2028, though those interim years are not presented here. By 2029, federal funding cuts will total $160 billion, triggering 1.65 million job losses. Slightly less than half of the jobs lost would be in health care, the leading sector for job growth in recent years.10 Research suggests these cuts also could reduce the capacity of hospitals and community health centers to provide care.11 The RHTP might offset a small portion of these losses through 2030, but it will be eclipsed by larger losses, particularly in urban areas where most Americans live. The economic repercussions of jobs lost in other areas, including grocery stores and food-related industries, will likely ripple to sectors such as retail, real estate, and construction across the nation.
Under H.R. 1, cuts to health and nutrition programs largely harm Americans with lower incomes, while tax cuts primarily benefit those with higher incomes. The CBO estimates that Americans in with lowest 10 percent of incomes will lose about $1,200 per year (3.1% of their incomes), while those with the top 10 percent of incomes will gain $13,600 per year (2.7% of their incomes).12 Other analyses reached similar conclusions.13
This brief illuminates another aspect of the budget cuts: how they harm state economies. While the budget cuts create $160 billion in savings for the federal government in 2029, state economic losses will outstrip those savings: we project state GDPs will decline by $197 billion, or about 23 percent more than the federal savings.
Cuts to Medicaid and SNAP will directly shift costs from the federal government to states. However, H.R. 1 will also lower state and local tax revenues by around $14 billion in 2029, making it harder for states to offset lost funds. Federal funding and tax revenue losses will likely force states to make further cuts to assistance programs and other public services like education. Though not directly required by H.R. 1, states could be forced to scale back programs such as home and community-based services for disabled and elderly populations.14
Proponents of the law explained that the budget cuts were intended to exclude “undeserving” populations from accessing benefits, such as able-bodied people who choose to not work, claiming these changes would ultimately help them gain jobs and incomes.15 But evidence indicates that work requirement programs do little to increase employment because they fail to address underlying reasons for unemployment.16 Moreover, by reducing the number of jobs in low-income communities, the new law could make it even harder for people to find jobs.
How We Conducted This Study
Estimating State-Level Federal Funding Changes
An important element of this analysis is estimating changes in federal funding for each state, based on the many sections of the bill. We began by estimating state “baseline” federal benefit expenditures for each state, using state estimates of Medicaid expenditures for fiscal year 2025 and actual SNAP expenditures for fiscal year 2024. These were then inflated to 2029 levels, based on Congressional Budget Office baselines, using data and methods described previously.17 For the Affordable Care Act marketplace, we used data about state-level ACA premium tax credits in 2024 and inflated these to 2026 and 2029 levels.
To estimate the reductions in federal funding that would occur at state levels we relied on the following sources:
We used Centers for Medicare and Medicaid Services Rural Health Transformation Program federal allocations to the 50 states in 2026.18 The total level of federal funding ($10 billion) will be the same in 2027 to 2030, although state allocations may differ slightly in future years. We assume that all $10 billion allocated in 2026 is spent that year; if actual outlays are lower, then the economic gains in that year will be reduced.
For the ACA marketplace analyses, we relied on the Urban Institute’s estimates of the state-level effects of the expiration of the ACA subsidies, H.R. 1 policies, and the value of ACA subsidies.19
State-level Medicaid funding reductions were based on detailed analyses published by KFF of the final version of H.R. 1, which included estimates related to the effect of work requirements, changes in provider taxes and state-directed payments, and shortened certification periods.20
State-level Supplemental Nutrition Assistance Program funding reductions were based on a combination of estimates of the impact of expanded work requirements by the Urban Institute21 and SNAP payment error rates for 2024 (to predict state matching requirements).22 Adjustments were made to accommodate final compromises in the legislation, such as potential adjustments for states with very high error rates and for work requirements in noncontiguous states.
Finally, all these state-level estimates were aligned with the CBO’s estimates of changes in federal funding for each of these programs based on the enacted version of H.R. 1, adjusting for programmatic budget interactions.23
Despite our efforts to use the best estimates available, we recognize that all projections are uncertain and that actual impacts may differ due to changing economic circumstances or state policy actions. Nonetheless, the analyses in this brief should provide conservative estimates of the approximate impact on federal funding levels and economic and employment effects.
Estimating Economic, Employment, and Tax Impacts
Our estimates of the economic, employment, and tax effects of reduced federal funding are produced using IMPLAN, a widely used input-output economic impact software system.24 The underlying logic of our analyses is that funding changes have “multiplier effects” that are felt initially in the health care and food sectors but soon spread out to other economic and employment sectors as well.
IMPLAN enables us to estimate three key impacts for states, their businesses, and residents: 1) changes in state gross domestic products (GDPs) caused by the reduction in federal funding; 2) changes in the number of jobs in the state, which are categorized as direct (health or food), indirect (other sectors) and total employment; and 3) changes in state and local tax revenues caused by the changes in household and business incomes. The definitions of these metrics were described previously.25
For Medicaid, we partitioned each state’s Medicaid loss in four health care sectors: hospital, ambulatory care, pharmaceuticals, and long-term care, based on estimated Medicaid spending in these sectors.26 The analysis of ACA marketplace changes was similar, although it did not include the long-term care sector, which is not covered by ACA plans. Our IMPLAN-based analysis of the cuts in SNAP funding was similar but focused on changes in food-related expenditures. As described in an earlier brief, households must blend SNAP benefits and their own income to purchase enough food; research shows that SNAP induces a marginal propensity to purchase more food. Thus, we allocated each state’s share of SNAP reductions in two parts: a 30 percent reduction in food purchases and a 70 percent reduction in other consumer goods purchased by low-income households.
Data about the types of organizations that will receive RHTP funding within states is not yet known, although CMS issued some guidelines for states, such as no more than 10 percent allocated for administration.27 Using the IMPLAN industry categories, we allocated each state’s allocation into funding for state health departments, hospitals, and ambulatory health clinics. In many cases, allocations may initially go to nonprofit organizations or businesses to help with health care staffing or health information technology; in the end we expect that the funds will ultimately be received by health care organizations.
All these analyses use IMPLAN’s Multi-Region Input-Output (MRIO) methodology to account for cross-state effects of the policies (sometimes called “leakages”).28 For example, some of the food purchased in Georgia may have been grown in Kansas or processed in Tennessee, so lower grocery purchases in one state may trigger losses in other states. For example, a nurse who loses her job in a Louisiana clinic might reside in Texas; thus, a job lost in one state could create economic losses in another.
How the Multiplier Effect Works
The figure below illustrates how the multiplier effect works for Medicaid and SNAP. For Medicaid, the reduction in federal Medicaid funds lead to reductions in state Medicaid programs’ budgets. In turn, the loss of insurance coverage lowers revenue to health care providers, like hospitals, clinics, pharmacies, and nursing homes. These are the direct effects.
In turn, health care providers must compensate for revenue losses by reducing how much they spend on staff and on goods and services from vendors (such as medical supplies, equipment, rent, and IT services). These businesses also must reduce spending on labor, goods, and services; the reductions in labor expenses means health providers and other businesses must lay off staff and reduce compensation. These are the indirect impacts of the policy change.
Finally, as employees lose income, they purchase fewer consumer goods and services (such as retail goods, transportation, groceries or rent). These are known as induced losses, which in turn lead to economic and employment losses. Falling personal and business income also lowers state and local revenue from income, sales, and other taxes, such as real estate taxes.
These principles also apply to the loss of federal SNAP funding. Although SNAP is administered by state agencies and benefits are distributed to recipients, the SNAP funds flow directly to grocery stores for food purchases, although as described above, economists recognize that consumers redeploy their available household income to purchase other goods and services. Parallel to the Medicaid example, these effects can be viewed as direct, indirect, and induced effects.
We focus on the effects of changes in federal funding because they are exogenous changes (“shocks”) in the resources available to each state and its residents caused solely by the federal policy changes. States, businesses, or individuals may compensate for the reduction in federal funding by shifting resources away from other uses (for example, cutting services or raising taxes) which have similar economic repercussions. Focusing on the federal budgetary changes makes our estimates more conservative. Also, some economic multiplier studies report the effects on a broader measure of economic activity, sometimes called output, which may double-count losses in production, wholesale, and retail sectors. We present estimates of changes in state GDPs, based on the value added (or lost) within a state; these are much more conservative and consistent with standard approaches for measuring state economies.
Medicaid, ACA, and SNAP cutbacks could have other harmful effects on health, nutrition, and well-being. A large body of research has demonstrated how the expansion of Medicaid coverage under the ACA led to improved health access, better health, and greater financial and mental well-being.29 SNAP has also been associated with better health and lower financial strain.30 For example, one report estimated H.R. 1 could cause medical debt to rise by as much as $50 billion,31 while another estimated 51,000 preventable deaths.32 The loss of health and nutrition benefits could impair health or mental well-being, leading to additional losses in productivity or higher health care costs. Our analyses do not account for these other health and social costs; they are based entirely on the economic repercussions of federal funding reductions on state economies and employment.
Summer is here and its first week is in the books. Like politics, the economy and life in general, it brought the good, bad and ugly attention to healthcare in the U.S.
The good:
At the American Society of Clinical Oncology (ASCO) meeting in Chicago, attendees heard about a breakthrough medication that dramatically improved results in pancreatic cancer patients (Revolution Medicine) and a gene editing tool capable of permanently lowering cholesterol (Lilly) with Chinese ascendence in the biotech science race a clear takeaway.
The American Hospital Association issued a statement accepting responsibility—in part—for healthcare affordability concerns mounting nationwide, calling for collaboration with insurers, drug companies and others to pursue solutions. In tandem, AHA released “Making Health Care More Affordable: A Blueprint to Lower Costs, Improve Access and Enhance Quality.” which recommends 5 core strategies and 24 actions to address affordability in a broader context of its systemic reform.
And the Bureau of Labor’s May jobs report brought a surprise: the labor market rebounded in May adding 179,000 jobs prompting speculation new Fed Chair Kevin Warsh might consider interest rate hikes to slow inflation (a policy that would encounter disfavor in the White House as Campaign 2026 looms).
The bad:
The House Appropriations Committee mark-up of its FY27 budget Friday included a 4% cut to FY27 HHS’ funding—less than the 12.5% President Trump proposed in his proposed budget but no less sobering.
The S&P 500 (-2.64%) and Nasdaq (-4.18%) each had their worst single-day drops of the year yesterday after the stronger-than-expected jobs report (BLS May) triggered a market selloff.Stocks fell across a broad range of sectors. The Dow Jones Industrial Average fell more than 1%, and the S&P 500 fell more than 2%. The tech-heavy Nasdaq composite sank more than 4%.
And the ugly:
Last Monday, CMS issued its work requirement directive to the 40 Medicaid expansion states detailing two new requirements they must meet to verify enrollment that begins in January: 1-
States must use unspecified data that’s not more than a year old to make the eligibility determinations as much as possible.
Starting Jan. 1, 2028, states must provide documentation proving medical frailty i.e. proof people have conditions that impair their ability to meet the requirements.
And these new stipulations come on top of administrative filing requirements that start at the end of this month and mandated twice/year eligibility verification oversight starting next year.
Per the CBO, the intensified policing of the Marketplaces (a legacy of the Affordable Care Act) is likely to shrink enrollment by 25% or more—that’s the point. The administration holds a view that states are ineffective in managing health programs like Medicaid, CHIP, the Marketplaces et al. contributing to un-attended fraud, waste and abuse.
Neither of the new stipulations from CMS is clear nor was either anticipated. They were an ugly surprise and none of 40 states is prepared.
My take
The promising breakthroughs in diagnostics and therapeutics like last week’s are the reasons most individuals in the U.S.—legal residents or not—believe our health system seeks to do no harm and provides dependable high-quality care, state of the art care (especially if you have insurance). They acknowledge it’s complex and expensive, but they accept it’s what we have for now.
But the bad and ugly news about healthcare seems to dominate media coverage, especially in social media where fact-checking is often shortcut.
For me, the highlight of the week was AHA’s statement committing itself to the pursuit affordability across the system by marshalling its peers to create meaningful solutions. Sign me up. Collaboration is the starting point. Transparency in its deliberations will be necessary to building trust in this process. Inclusion of all proposed solutions subjected to objective review will be its necessary start. And timing is key: election season tends to distort messaging and draw critics. The urgency of direction is no less key: ideally, meaningful direction and substantive recommendations should follow soon after but be independent of Campaign 2026 results in state and federal elections.
Paul
PS I am in DC this weekend celebrating HFMA’s 80th Anniversary at National Harbor. Now living away after 15 years in the nation’s capital, visits like this are bittersweet. There’s no doubt healthcare’s impacted by the laws, rules, administrative actions, executive orders, SCOTUS decisions and appropriations that originate here, but I’ve come to appreciate three realities since leaving here years ago:
1-U.S. healthcare is decreasingly controlled by DC-originated actions and activities. The corrosive impact of partisan brinksmanship in our elective politics has eroded faith and confidence in its purpose and intent, especially in federal government.
2 Changes to the system are increasingly the result of states forced to cope with health & social services programs and private capital seeking shareholder gain. How these align (or not) will be keys to U.S. healthcare’s future. Today, there’s more dissonance than consonance in their directions.
3-Only a few are planning for healthcare’s long-term future. The agenda for most in this industry-including the majority attending HFMA this week- is short-term survival and sustainability. Long-range strategic planning and meaningful assessment of future state scenarios are luxuries for most. Clearly, issues like affordability did not surface overnight.
In the United States, laws that define how our health system operates have evolved over our 250-year history. They’re built on allopathic medical pedagogy borrowed from our European roots and evolve around clinical innovations and technologies that improve outcomes and extend life.
Historically, federal agencies oversaw its evolution: the Departments of Health and Human Services (providers, insurers, drugs) Justice (antitrust), Federal Trade Commission i(interstate commerce, marketing practices) were primary actors with Agriculture (food supply) and Interior (natural resources) playing support roles. And the federal court system adjudicates challenges. But that’s changing: states are playing a bigger role. State attorneys general and Supreme Courts are pulled in more frequently.
Since the Supreme Court’s 2022 ruling in Dobbs v. Jackson Women’s Health Organization that overturned Roe v. Wade, healthcare issues have become more prominent in state lawmaking. That decision essentially delegated abortion rights to states to handle. And, in HR1 (One Big Beautiful Bill Act 2025), Congress cut federal Medicaid funding by almost $900 billion over 10 years essentially forcing states to find different ways to manage it. Today, Medicaid is 30.7% of the average state’s expenditures with half sourced from state general funds. OB3 will add fiscal pressure to every state.
In Campaign 2026, healthcare referenda will appear alongside candidates match-ups on many state ballots. Candidates in the 36 Gubernatorial/Territorial races and every Congressional race face questions about how they’ll “fix” healthcare. The combination of the public’s discontent with Congress and its dissatisfaction with the health system will prompt states to address a widening range of healthcare issues of consequence to their citizens. For some issues, Governors will issue Executive Orders, for others, referenda will appear on voter ballots and in others, legislation will be approved by their legislatures. The list is long…
Expansion of price transparency (PT) requirements for hospitals, insurers and (likely) physician services: Increased stipulations to increase awareness and use of pricing tools beyond current regulations.
Limitations on private equity ownership: States may require disclosures of private equity investments and many will seek modification of carried interest, clinical autonomy and governance structures.
Scope of practice expansion: States are expanding clinical responsibilities for advanced practice nurses, pharmacists and others to enable access to primary and preventive health services.
Prior authorization and payment integrity: States will require insurers to adopt business practices that reduce enrollee and provider challenges, financial shortfalls and disputes. In tandem, states will expand payment integrity alignment with evidence-based practices that reduce unnecessary care.
Implementation of site neutral payment policies: Despite federal pushback, states will align with employers and insurers to expand site neutral payment policies opposed by hospitals.
Re-calculation of community benefits and limitations on tax exemptions: Large, NFP systems will face state and federal regulatory pressure to forego/limit tax exemptions.
Price controls on prescription drugs (above and beyond most favored nation stipulations): States will enact legislation creating Drug Price Control Commissions to limit drug price escalation. In some, importation and restrictive formulary strategies will be enacted/expanded.
State constraints on PBM and GPO activity: States will advance business practice restrictions on PBMs and GPOs geared to consumer protections, greater transparency and increased competition.
Relief of Stark, Physician Self-Referral Limitations: Some states will expand physician ownership arrangements and enable physicians to compete with hospitals and other providers.
Integration of social services with local delivery systems: States will facilitate delivery systems in which public health and provider services are fully integrated and population health management improvement is optimized.
The bottom line:
Total state spending on for healthcare services increased 5.7% to $3.2 trillion in 2025 slightly more than the 38-year average of 5.6%. In fiscal 2025 federal funds to states rose 5.5% following three consecutive years of decreases from fiscal 2022 to fiscal 2024. Thus, states were forced to provide more funding for their healthcare programs even as the U.S. economy sputtered and, most recently, as affordability issues mounted for voters.
Healthcare’s future in the U.S. will continue to be framed by federal policies and the political system from which its laws originate, but its transformational changes will increasingly originate in states where affordability, funding and system effectiveness issues are tackled head-on.
As financial challenges persist and clinical labor remains difficult to replace, many hospitals are turning to restructuring for cost savings.
KEY TAKEAWAYS
Care New England, Washington Regional Medical System, and Intermountain Health all announced layoffs that prominently affected administrative functions.
Hospitals are increasingly embracing “The Great Flattening,” consolidating nonclinical roles to reduce overhead while preserving frontline care capacity.
While leaner organizational structures may improve efficiency and speed decision-making, reducing leadership layers can also create operational strain and place added burden on remaining staff.
Three notable health systems announced layoffs in recent days, and in all three cases, management and leadership roles were largely affected. Even as labor costs continue to climb, clinical talent remains scarce, making administrative jobs often the primary target of workforce reductions.
Healthcare, and hospitals specifically, are not immune to “The Great Flattening” impacting corporate America. Companies across industries have spent recent years trimming down middle management, if not outright eliminating those positions, for the purpose of creating leaner workforce structures and cutting overhead.
In the case of hospitals, many have taken the step to consolidate functions that aren’t directly tied to delivering patient care.
The trend became particularly visible over the past week with Care New England, Washington Regional Medical System, and Intermountain Health all initiating reductions.
Providence, Rhode Island-based Care New England eliminated more than 30 leadership and nonclinical positions as part of a restructuring to address financial pressures and help close an estimated $20 million budget gap for fiscal year 2026. System president and CEO Michael Wagner said in a statement that “current financial conditions have made additional cost-saving measures unavoidable.”
Elsewhere, Washington Regional Medical System announced a restructuring plan that included 86 job cuts through consolidation of management and support functions. “By restructuring our management operations and consolidating roles, Washington Regional will reduce redundancies and optimize efficiency while still providing the high-quality care our community has come to expect,” Lucas Campbell, president and CEO of Washington Regional, said in the announcement.
At Intermountain Health, the 93 positions that were eliminated amid clinic closures and operational changes in Colorado and Montana looked a little different. While clinical roles were affected as part of the restructuring, the organization also pointed to leadership and administrative consolidation to improve efficiency and better align resources.
Though the circumstances surrounding the three systems differed, the overlap across the layoffs was the emphasis on leadership restructuring and administrative streamlining.
The logic behind these restructurings is straightforward: clinical workers are difficult to replace, whereas administrative costs often represent one of the few areas where organizations can still reduce spending relatively quickly.
According to Kaufman Hall’s latest National Hospital Flash Report for March, hospitals are operating more efficiently, but financial performance is still being weighed down by rising expenses. Length of stay, for example, was down 3% year-over-year, indicative of improved throughput. However, that clinical efficiency requires adequate staffing, and that labor is costly, as seen in a 4% rise in labor expense per calendar day year-over-year.
To just maintain their thin margins, hospitals are being forced to cut costs in areas that won’t directly hinder patient flow. That’s why administrative restructuring is often viewed as a less disruptive path toward reducing overhead while sustaining operational efficiency.
The result can also be a faster decision-making structure, allowing organizations to be strategically nimbler during a time when moving slow can leave hospitals behind the curve.
Still, the benefits come at a price. The loss of leadership and management may not be felt in financial performance immediately, but over time, it can create operational strain and place additional burden on remaining leaders and frontline staff.
For hospital executives, the question they must answer is how far their organization can streamline before efficiency gains start to create new organizational pressures.