The drugstore retailer faces debt maturities, while the upending of some strategies introduces new uncertainties, analysts said.
S&P Global Ratings analysts have downgraded Walgreens Boot Alliance by two notches, to ‘BB’ from ‘BBB-’, which puts the drugstore company into speculative-grade territory.
Analysts Diya Iyer and Hanna Zhang cited guidance for the year “notably below” their expectations, and said “material strategic changes, limited cash flow generation, and large maturities in coming years are key risks to the business.”
The company is struggling in its retail business as well as its pharmacy operations, they said in a Friday client note. In the U.S., margins are taking a hit on the pharmacy side from reimbursement pressure and on the retail side from declining sales volume and higher shrink. They expect Walgreens’ S&P Global Ratings-adjusted EBITDA margin to decline more than 100 basis points this fiscal year, dipping below 5%, from 6% last year, though the company’s cost cuts will counter that somewhat.
Walgreens’ debt and its need to refinance much of it represent another “key risk,” they said. This November, Walgreens faces $1.4 billion in maturities, mostly U.S. bonds. Another $2.8 billion comes due in fiscal 2026 and $1.8 billion in fiscal 2027. The analysts called Walgreens’ move to consolidate cash “prudent” in case refinancing isn’t possible.
“We will be monitoring how Walgreens’ new management addresses this large debt load closely amid its persistently weak performance and higher interest rates,” Iyer and Zhang said.
Beyond those financial realities, though, are strategic weaknesses. Ex-Cigna executive Tim Wentworth took over as CEO last fall and this year has overseen a strategic review that has entailed more layoffs and store closures.
Walgreens has also upended some of its plans to expand its medical care operations, divesting of or shrinking many of its original investments and plans. Last month, for example, the company announced it would reduce its stake in value-based medical chain VillageMD, saying it will no longer be the company’s majority owner, after closing dozens of the clinics last year. The company first poured $1 billion into VillageMD in 2020 and more than doubled its stake for another $5.2 billion the following year, but the banner’s waning value helped drive a $6 billion loss in Q2.
Despite such moves, Iyer and Zhang said they continue to see the VillageMD banner as “a significant drag on profitability due to the rising cost of labor, pressures from reimbursement, and lower volumes.”
Walgreens’ acquisition streak led the S&P analysts to believe that it would divest of its Boots U.K. business, which could have helped pay down $8 billion to $10 billion in debt. But the company called off the idea about two years ago.
“We believe these frequent and large changes to the company’s strategic plans diminish management’s credibility to execute on a sustainable and cohesive operating model for Walgreens in both the near and long term,” Iyer and Zhang said.
Gains that Walgreens has managed to eke from its medical operations haven’t managed to offset declines on the retail said, they also said, adding that they are closely watching what it does next with its massive footprint. The company last year announced that it would close 150 stores in the U.S. and 300 in the U.K. and just last month said it was reviewing 25% of its current footprint, with plans to shutter a “significant portion” of its roughly 8,700 stores.
“Our ratings continue to reflect Walgreens’ large scale and its efforts to address its credit metric profile. With almost $140 billion in sales in fiscal 2023 and a diverse array of global businesses, Walgreens remains prominent in the drugstore space,” they said. “However, we think its scale is providing less protection to profitability at least partly due to inconsistent strategic direction.”
Medicare Advantage provides health coverage to more than half of the nation’s seniors, but some hospitals and health systems are opting to end their contracts with MA plans over administrative challenges.
Among the most commonly cited reasons are excessive prior authorization denial rates and slow payments from insurers.
In 2023, Becker’s began reporting on hospitals and health systems nationwide that dropped some or all of their Medicare Advantage contracts.
In January, the Healthcare Financial Management Association released a survey of 135 health system CFOs, which found that 16% of systems are planning to stop accepting one or more MA plans in the next two years. Another 45% said they are considering the same but have not made a final decision. The report also found that 62% of CFOs believe collecting from MA is “significantly more difficult” than it was two years ago.
Fifteen health systems dropping Medicare Advantage plans in 2024:
1. Canton, Ohio-based Aultman Health System‘s hospitals will no longer be in network with Humana Medicare Advantage after July 1, and its physicians will no longer be in network after Aug. 1.
3. Munster, Ind.-based Powers Health (formerly Community Healthcare System) went out of network with Humana and Aetna’s Medicare Advantage plans on June 1.
6. York, Pa.-based WellSpan Health stopped accepting Humana Medicare Advantage and UnitedHealthcare Medicare Advantage plans on Jan. 1. UnitedHealthcare D-SNP plans in some locations are still accepted.
7. Newark, Del.-based ChristianaCare is out of network with Humana’s Medicare Advantage plans as of Jan. 1, with the exception of home health services.
8. Greenville, N.C.-based ECU Health stopped accepting Humana’s Medicare Advantage plans in January.
9. Zanesville, Ohio-based Genesis Healthcare System dropped Anthem BCBS and Humana Medicare Advantage plans in January.
10. Corvallis, Ore.-based Samaritan Health Services’ hospitals went out of network with UnitedHealthcare’s Medicare Advantage plans on Jan. 9. Samaritan’s physicians and provider services will be out of network on Nov. 1.
Regular readers of HEALTH CARE un-covered know that I write frequently about the huge amounts of money the health insurance industry’s pharmacy benefit managers (PBMs) extract from the prescription drug supply chain. I also submitted a comment letter to the Federal Trade Commission two and a half years ago urging it to launch an investigation into PBM business practices that have contributed to the closure of hundreds of independent pharmacies across the country and to millions of Americans walking away from the pharmacy counter without their medications.
On a bipartisan basis, the FTC did launch an inquiry into the PBM business, and today the Commission issued a damning interim report that confirmed what industry critics, including me, have been saying:
Just six companies now control 95% of the pharmacy benefit market, and these Big Insurance-owned middlemen “profit at the expense of patients by inflating drug costs and squeezing Main Street pharmacies.” Below you’ll find the commission’s statement on its preliminary findings.
Last year, we also published a profile of one of the industry’s most vocal critics in Congress, Rep. Earl L. “Buddy” Carter (R-Ga.), a pharmacist by trade who has seen PBM’s profiteering firsthand. In a press release this morning, Carter said:
Since day one in Congress, I’ve been calling on the FTC to investigate PBMs, which use deceptive and anti-competitive practices to line their own pockets while reducing patients’ access to affordable, quality health care. I’m proud that the FTC launched a bipartisan investigation into these shadowy middlemen, and its preliminary findings prove yet again that it’s time to bust up the PBM monopoly. We are losing more than one pharmacy per day in this country, causing pharmacy deserts and taking the most accessible health care professionals in America out of people’s communities. I am calling on the FTC to promptly complete its investigation and begin enforcement actions if – and when – it uncovers illegal and anti-competitive PBM practices.
Carter and several other members of Congress have introduced bipartisan bills to rein in PBMs. The House has passed PBM reform legislation but the Senate has not yet done so, but there is growing support in both chambers to enact one or more bills by the end of the year. The FTC’s interim report should make that more likely to happen.
Read the FTC’s full press release below:
FTC Releases Interim Staff Report on Prescription Drug Middlemen
Report details how prescription drug middleman profit at the expense of patients by inflating drug costs and squeezing Main Street pharmacies
The Federal Trade Commission today published an interim report on the prescription drug middleman industry that underscores the impact pharmacy benefit managers (PBMs) have on the accessibility and affordability of prescription drugs.
The interim staff report, which is part of an ongoing inquiry launched in 2022 by the FTC, details how increasing vertical integration and concentration has enabled the six largest PBMs to manage nearly 95 percent of all prescriptions filled in the United States.
This vertically integrated and concentrated market structure has allowed PBMs to profit at the expense of patients and independent pharmacists, the report details.
“The FTC’s interim report lays out how dominant pharmacy benefit managers can hike the cost of drugs—including overcharging patients for cancer drugs,” said FTC Chair Lina M. Khan. “The report also details how PBMs can squeeze independent pharmacies that many Americans—especially those in rural communities—depend on for essential care. The FTC will continue to use all our tools and authorities to scrutinize dominant players across healthcare markets and ensure that Americans can access affordable healthcare.”
The report finds that PBMs wield enormous power over patients’ ability to access and afford their prescription drugs, allowing PBMs to significantly influence what drugs are available and at what price. This can have dire consequences, with nearly 30 percent of Americans surveyed reporting rationing or even skipping doses of their prescribed medicines due to high costs, the report states.
The interim report also finds that PBMs hold substantial influence over independent pharmacies by imposing unfair, arbitrary, and harmful contractual terms that can impact independent pharmacies’ ability to stay in business and serve their communities.
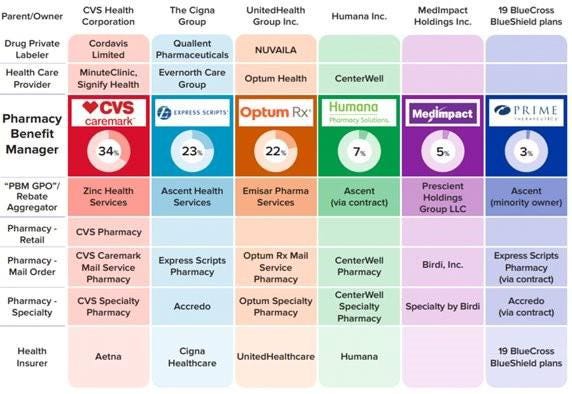
The Commission’s interim report stems from special orders the FTC issued in 2022, under Section 6(b) of the FTC Act, to the six largest PBMs—Caremark Rx, LLC; Express Scripts, Inc.; OptumRx, Inc.; Humana Pharmacy Solutions, Inc.; Prime Therapeutics LLC; and MedImpact Healthcare Systems, Inc. In 2023, the FTC issued additional orders to Zinc Health Services, LLC, Ascent Health Services, LLC, and Emisar Pharma Services LLC, which are each rebate aggregating entities, also known as “group purchasing organizations,” that negotiate drug rebates on behalf of PBMs.
PBMs are part of complex vertically integrated health care conglomerates, and the PBM industry is highly concentrated. As shown in the below image, this concentration and integration gives them significant power over the pharmaceutical supply chain. The percentages reflect the amount of prescriptions filled in the United States.
The interim report highlights several key insights gathered from documents and data obtained from the FTC’s orders, as well as from publicly available information:
Concentration and vertical integration: The market for pharmacy benefit management services has become highly concentrated, and the largest PBMs are now also vertically integrated with the nation’s largest health insurers and specialty and retail pharmacies.
The top three PBMs processed nearly 80 percent of the approximately 6.6 billion prescriptions dispensed by U.S. pharmacies in 2023, while the top six PBMs processed more than 90 percent.
Pharmacies affiliated with the three largest PBMs now account for nearly 70 percent of all specialty drug revenue.
Significant power and influence: As a result of this high degree of consolidation and vertical integration, the leading PBMs now exercise significant power over Americans’ ability to access and afford their prescription drugs.
The largest PBMs often exercise significant control over what drugs are available and at what price, and which pharmacies patients can use to access their prescribed medications.
PBMs oversee these critical decisions about access to and affordability of life-saving medications, without transparency or accountability to the public.
Self-preferencing: Vertically integrated PBMs appear to have the ability and incentive to prefer their own affiliated businesses, creating conflicts of interest that can disadvantage unaffiliated pharmacies and increase prescription drug costs.
PBMs may be steering patients to their affiliated pharmacies and away from smaller, independent pharmacies.
These practices have allowed pharmacies affiliated with the three largest PBMs to retain high levels of dispensing revenue in excess of their estimated drug acquisition costs, including nearly $1.6 billion in excess revenue on just two cancer drugs in under three years.
Unfair contract terms: Evidence suggests that increased concentration gives the leading PBMs leverage to enter contractual relationships that disadvantage smaller, unaffiliated pharmacies.
The rates in PBM contracts with independent pharmacies often do not clearly reflect the ultimate total payment amounts, making it difficult or impossible for pharmacists to ascertain how much they will be compensated.
Efforts to limit access to low-cost competitors: PBMs and brand drug manufacturers negotiate prescription drug rebates some of which are expressly conditioned on limiting access to potentially lower-cost generic and biosimilar competitors.
Evidence suggests that PBMs and brand pharmaceutical manufacturers sometimes enter agreements to exclude lower-cost competitor drugs from the PBM’s formulary in exchange for increased rebates from manufacturers.
The report notes that several of the PBMs that were issued orders have not been forthcoming and timely in their responses, and they still have not completed their required submissions, which has hindered the Commission’s ability to perform its statutory mission. FTC staff have demanded that the companies finalize their productions required by the 6(b) orders promptly. If, however, any of the companies fail to fully comply with the 6(b) orders or engage in further delay tactics, the FTC can take them to district court to compel compliance.
The FTC remains committed to providing timely updates as the Commission receives and reviews additional information.
The Commission voted 4-1 to allow staff to issue the interim report, with Commissioner Melissa Holyoak voting no. Chair Lina M. Khan issued a statement joined by Commissioners Rebecca Kelly Slaughter and Alvaro Bedoya. Commissioners Andrew N. Ferguson and Melissa Holyoak each issued separate statements. The Federal Trade Commission develops policy initiatives on issues that affect competition, consumers, and the U.S. economy. The FTC will never demand money, make threats, tell you to transfer money, or promise you a prize. Follow the FTC on social media, read consumer alerts and the business blog, and sign up to get the latest FTC news and alerts.
Medicare Advantage plans received $50 billion in payments between 2018 and 2021 for diagnoses insurers added to medical records, a Wall Street Journal investigation published July 8 has found.
The Journal investigated billions of Medicare Advantage records and found that some conditions were diagnosed at a much higher rate among Medicare Advantage beneficiaries than among traditional Medicare beneficiaries. For example, diabetic cataracts were diagnosed much more often among Medicare Advantage beneficiaries than among traditional Medicare beneficiaries, the Journal found.
The federal government pays Medicare Advantage plans a rate per beneficiary based on their diagnoses.
CMS does not reimburse MA plans for beneficiaries with non-diabetic cataracts, a common condition among older adults, according to the Journal. The government does reimburse for diabetic cataracts. CMS paid Medicare Advantage plans more than $700 million for diabetic cataracts diagnoses between 2018 and 2021, the investigation found.
A spokesperson for UnitedHealth, the largest Medicare Advantage insurer, told the Journal its analysis was “inaccurate and biased.” Medicare Advantage plans code diagnoses more completely and ensure diseases are caught earlier, the spokesperson told the outlet.
The Journal’s investigation also found some Medicare Advantage beneficiaries were diagnosed with serious diseases in their medical records, but no evidence of treatment for the disease appeared in these patients’ records. Among beneficiaries who had a diagnosis of HIV added to their record by their insurer, just 17% received treatment for the disease, according to the investigation. Among beneficiaries who were diagnosed with HIV by their physician, 92% received treatment.
The Journal’s investigation is the latest examining upcoding by MA plans. A 2022 report in The New York Times alleged some insurers incentivized employees or physicians to add diagnoses to patients’ reports. Nearly every major payer has been accused of overbilling by a whistleblower, the federal government or an investigation by HHS’ Office of Inspector General.
MedPAC, which advises the government on Medicare issues, estimates the federal government will spend $83 billion more on Medicare Advantage beneficiaries than if they were enrolled in fee-for-service Medicare. Coding intensity in MA will be 20% higher than in fee-for-service in 2024, according to the commission.
UnitedHealth Group’s Optum, the largest employer of physicians in the U.S., is expanding its reach in behavioral health.
The company added 45,000 therapists, psychiatrists and behavioral health providers to its network in 2023, and it has more than 430,000 behavioral health clinicians in its network overall.
Here are five things to know about Optum’s behavioral health offerings:
The company is acquiring behavioral health clinics. Optum recently picked up Care Counseling, which employs more than 200 clinicians at 10 clinics in the Minneapolis area. In 2022, Optum acquired Refresh Mental Health, which operates more than 300 outpatient sites in 37 states.
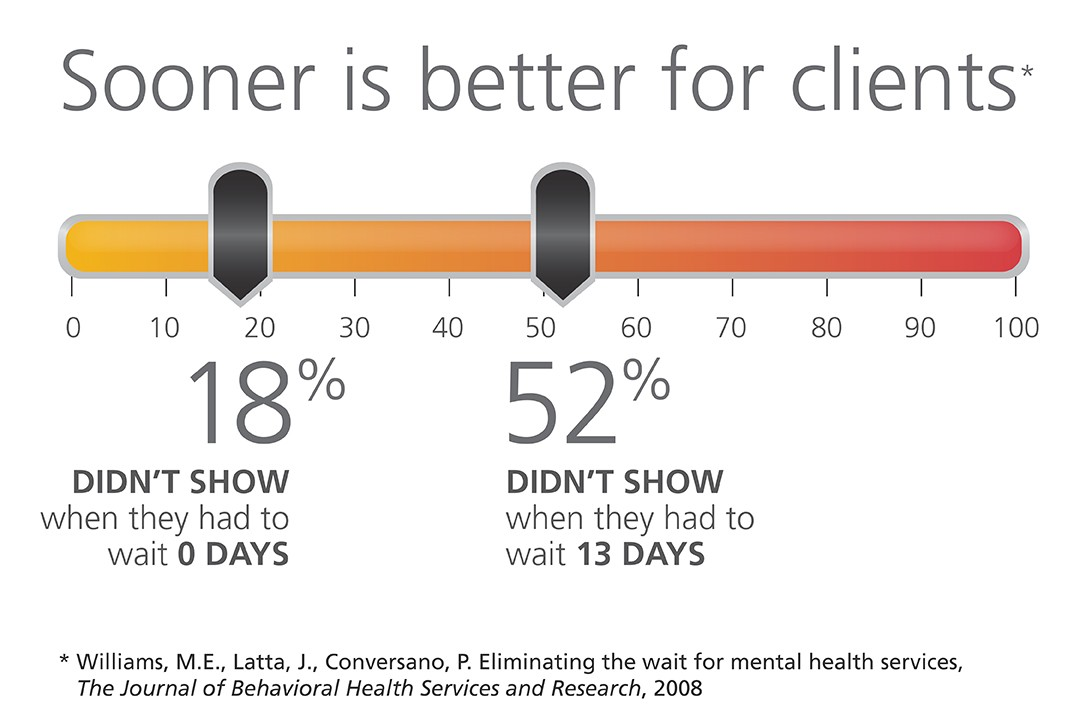
Optum’s acquisitions of behavioral health providers have helped cut wait times for patients, Optum CEO Heather Cianfrocco said in May.
“On average it takes over 50 to 60 days to get an appointment for high-quality behavioral care,” she said. “We started acquiring our own behavioral providers to be able to reduce that access issue.”
The company is also targeting in-home behavioral care. In December 2023, Amar Desai, MD, CEO of Optum Health, said the company had integrated behavioral care into its home health offerings.
“As a practicing physician, I am particularly excited that we are becoming the practice and partner of choice in the marketplace,” Dr. Desai said of the business.
Optum also administers behavioral health benefits systems for states, though it recently lost contracts to manage programs in Maryland and Idaho.
OptumRx, a pharmaceutical benefit manager, provides medication management for behavioral health, substance use disorder and other complex drugs for more than 1 million people each year.