While cities like New York have seen a hopeful drop in cases, upticks in other major cities and smaller communities have offset those decreases.
In New York City, the daily onslaught of death from the coronavirus has dropped to half of what it was. In Chicago, a makeshift hospital in a lakefront convention center is closing, deemed no longer needed. And in New Orleans, new cases have dwindled to a handful each day.
Yet across America, those signs of progress obscure a darker reality.
The country is still in the firm grip of a pandemic with little hope of release. For every indication of improvement in controlling the virus, new outbreaks have emerged elsewhere, leaving the nation stuck in a steady, unrelenting march of deaths and infections.
As states continue to lift restrictions meant to stop the virus, impatient Americans are freely returning to shopping, lingering in restaurants and gathering in parks. Regular new flare-ups and super-spreader events are expected to be close behind.
Any notion that the coronavirus threat is fading away appears to be magical thinking, at odds with what the latest numbers show.
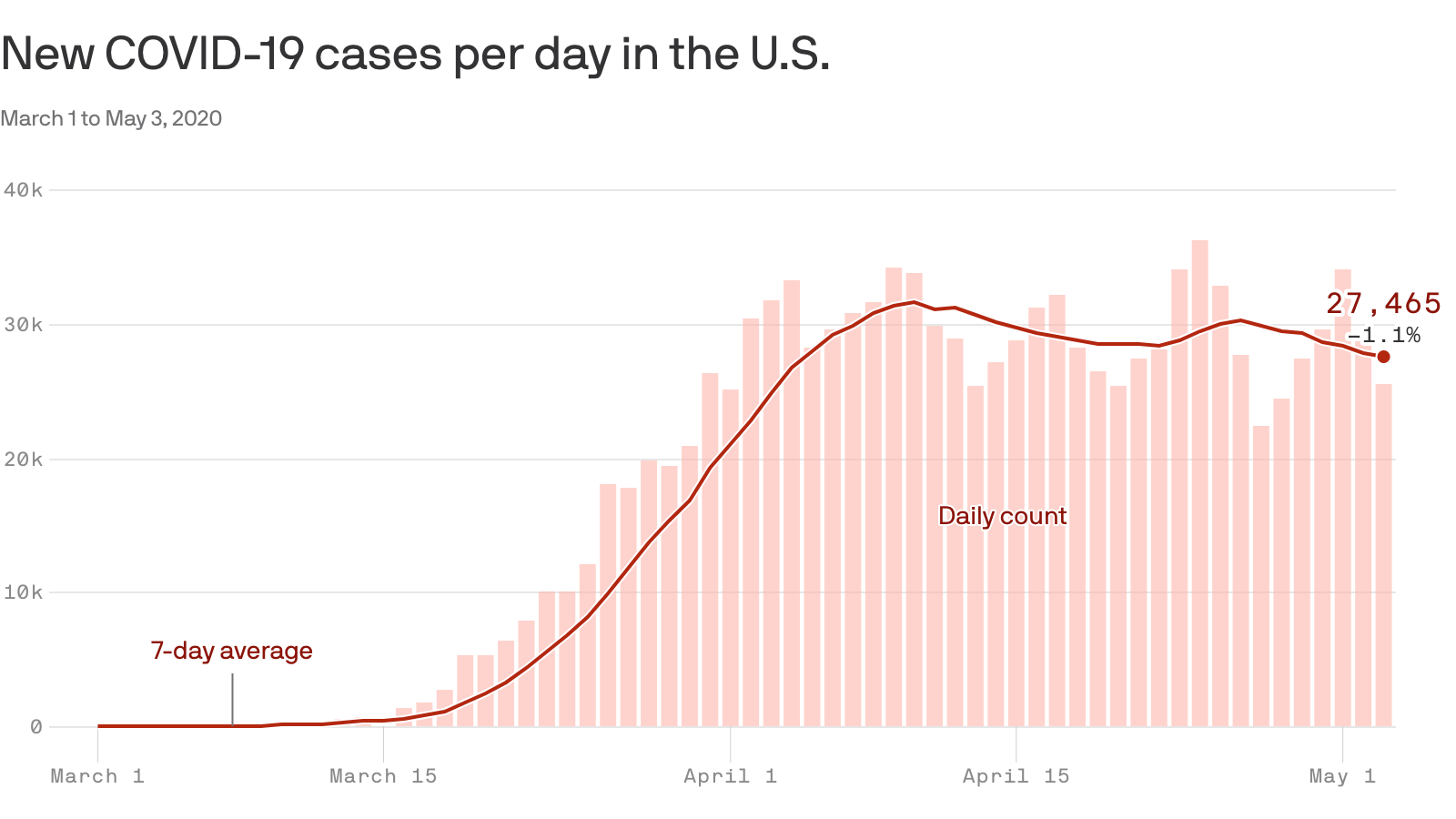
Coronavirus in America now looks like this: More than a month has passed since there was a day with fewer than 1,000 deaths from the virus. Almost every day, at least 25,000 new coronavirus cases are identified, meaning that the total in the United States — which has the highest number of known cases in the world with more than a million — is expanding by between 2 and 4 percent daily.
Rural towns that one month ago were unscathed are suddenly hot spots for the virus. It is rampaging through nursing homes, meatpacking plants and prisons, killing the medically vulnerable and the poor, and new outbreaks keep emerging in grocery stores, Walmarts or factories, an ominous harbinger of what a full reopening of the economy will bring.
While dozens of rural counties have no known coronavirus cases, a panoramic view of the country reveals a grim and distressing picture.
“If you include New York, it looks like a plateau moving down,’’ said Andrew Noymer, an associate professor of public health at the University of California, Irvine. “If you exclude New York, it’s a plateau slowly moving up.”
In early April, more than 5,000 new cases were regularly being added in New York City on a daily basis. Those numbers have dropped significantly over the last few weeks, but that progress has been largely offset by increases in other major cities.
Consider Chicago and Los Angeles, which have flattened their curves and avoided the explosive growth of New York City. Even so, coronavirus cases in their counties have more than doubled since April 18. Cook County, home to Chicago, is now sometimes adding more than 2,000 new cases in a day, and Los Angeles County has often been adding at least 1,000.
Dallas County in Texas has been adding about 100 more cases than it was a month ago, and the counties that include Boston and Indianapolis have also reported higher numbers.
It is not just the major cities. Smaller towns and rural counties in the Midwest and South have suddenly been hit hard, underscoring the capriciousness of the pandemic.
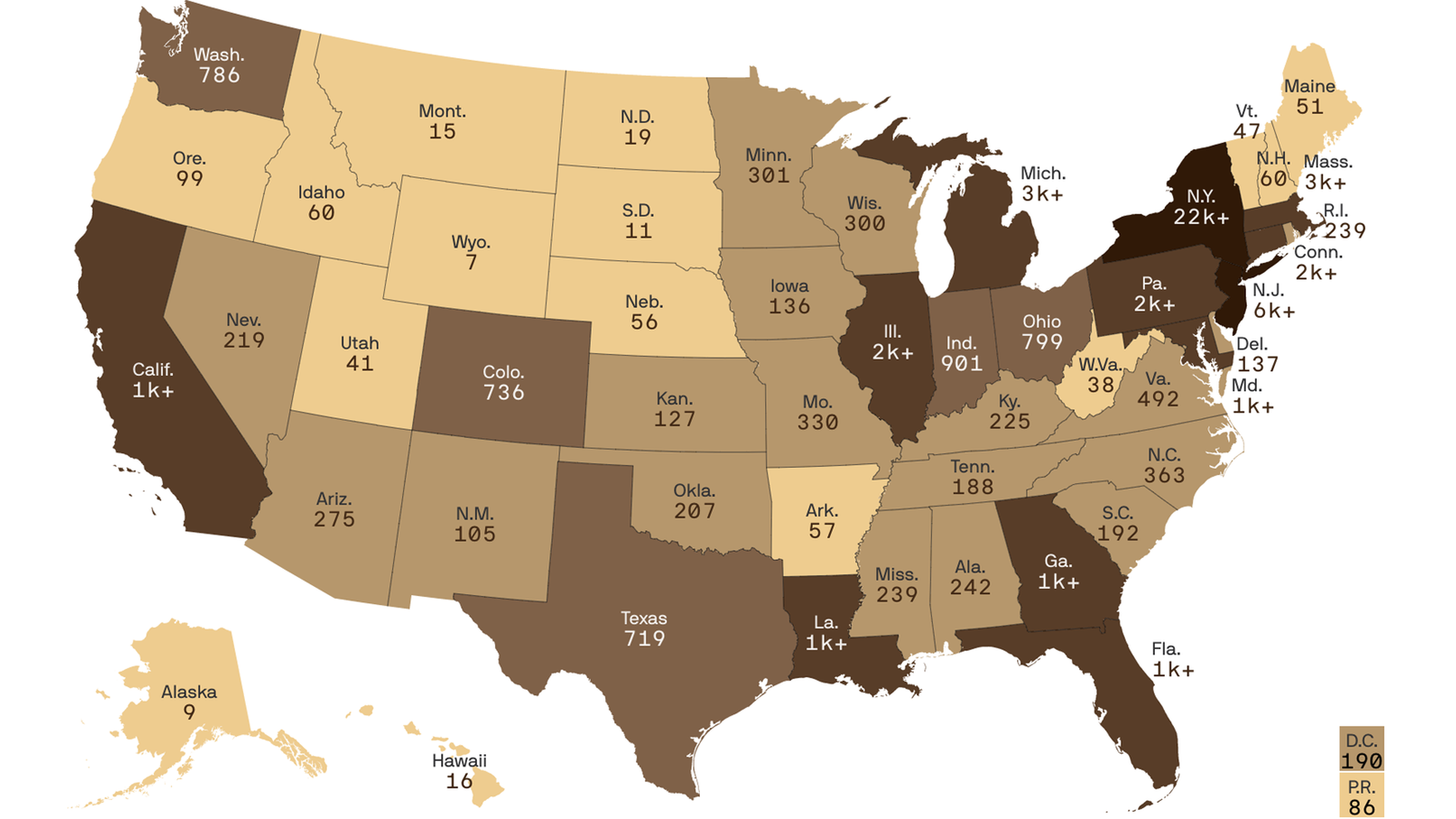
Dakota County, Neb., which has the third-most cases per capita in the country, had no known cases as recently as April 11. Now the county is a hot zone for the virus.
Dakota City is home to a major Tyson beef-processing plant, where cases have been reported. And the region, which spreads across the borders of both Iowa and South Dakota, is dotted with meat-processing plants that have been a major source of work for generations. The pattern has repeated all over: Federal authorities say that at least 4,900 meat and poultry processing workers have been infected across 19 states.
The Tyson plant in Dakota City has temporarily closed for deep cleaning. Now the workers wait, afraid to go back to work but fearful not to.
“They need money and they want to go back of course,” said Qudsia Hussein, whose husband is an imam in the area. With many businesses shuttered or suffering financially because of the pandemic, she said, “There’s no other place they can work.”
Trousdale County, Tenn., another rural area, suddenly finds itself with the nation’s highest per capita infection rate by far. A prison appears responsible for a huge spike in cases; in 10 days, this county of about 11,000 residents saw its known cases skyrocket to 1,344 from 27.
As of last week, more than half of the inmates and staff members tested at Trousdale Turner Correctional Center in Hartsville, Tenn., were positive for the virus, officials said.
“It’s been my worst nightmare since the beginning of this that this would happen,” said Dwight Jewell, chairman of the Trousdale County Commission. “I’ve been expecting this. You put that many people in a contained environment and all it takes is one.”
Everyone in town knows about the outbreak. But they are defiant: Businesses in the county are reopening this week. On Monday evening, county commissioners were scheduled to have an in-person meeting, with chairs spaced six feet apart. They have a budget to pass and other issues facing the county, Mr. Jewell said.
“We’ve got to get back to the business of the community,” he said.
Infectious-disease experts are troubled by perceptions that the United States has seen the worst of the virus, and have sought to caution against misplaced optimism.
“I don’t see why we expect large declines in daily case counts over the next month,” Trevor Bedford, a scientist at the Fred Hutchinson Cancer Research Center who has studied the spread and evolution of the virus, wrote on Twitter. He added, “There may well be cities / counties that achieve suppression locally, but nationally I expect things to be messy with flare-ups in various geographies followed by responses to these flare-ups.”
The outbreak in the United States has already killed more than 68,000 people, and epidemiologists say the nation will not see fewer than 5,000 coronavirus-related deaths a week until after June 20, according to a survey conducted by researchers at the University of Massachusetts at Amherst.
An aggregate of several models assembled by Nicholas Reich, a biostatistician at the university, predicts there will be an average of 10,000 deaths per week for the next few weeks. That is fewer than in previous weeks, but it does not mean a peak has been passed, Dr. Reich said. In the seven-day period that ended on Sunday, about 12,700 deaths tied to the virus occurred across the country.
“There’s this idea that it’s going to go up and it’s going to come down in a symmetric curve,” Dr. Reich said. “It doesn’t have to do that. It could go up and we could have several thousand deaths per week for many weeks.”
The deaths have hit few places harder than America’s nursing homes and other long-term care facilities. More than a quarter of the deaths have been linked to those facilities, and more than 118,000 residents and staff members in at least 6,800 homes have contracted the virus.
There is no escaping some basic epidemic math.
In the absence of a vaccine, stopping the spread of the virus requires about two-thirds of the population to have been infected. And some experts have argued that before what is known as herd immunity kicks in, the number of people infected nationwide could reach a staggering 90 percent if social distancing is relaxed and transmission rates climb. (It is also not clear how long immunity will last among those who have been infected.)
As testing capacity has increased, so has the number of cases being counted. But many jurisdictions are still missing cases and undercounting deaths. Many epidemiologists assume that roughly 10 times as many people have been infected with the coronavirus than the number of known cases.
Because of the time it will take for infections to spread, incubate and cause people to die, the effects of reopening states may not be known until six weeks after the fact. One model used by the Centers for Disease Control and Prevention includes an assumption that the infection rate will increase up to 20 percent in states that reopen.
Under that model, by early August, the most likely outcome is 3,000 more deaths in Georgia than the state has right now, 10,000 more each in New York and New Jersey, and around 7,000 more each in Pennsylvania, Illinois and Massachusetts. Under the model’s most likely forecast, the nation will see about 100,000 additional deaths by Aug. 4.
“Even if we’re past the first peak, that doesn’t mean the worst is behind us,” said Youyang Gu, the data scientist who created the model. “It goes up quickly but it’s a slow decline down.”