Cases of COVID-19 have increased during the last 14 days in 10 states and Washington, D.C., with the latest additions of the district and Illinois.
Nationwide, COVID-19 cases decreased 15 percent over the past 14 days, according to HHS data collected by The New York Times. But as the more contagious omicron subvariant BA.2 continues to spread, cases are ticking upward in 10 states and D.C. as of March 25. Cases were moving upward in nine states as of March 24, with D.C. and Illinois reporting increases a day later.
Here are the 14-day changes for cases in each state reporting an increase, according to HHS data collected by The New York Times:
New York: 44 percent
Kentucky: 35 percent
Arkansas: 23 percent
Colorado: 21 percent
Connecticut: 18 percent
Texas: 17 percent
Massachusetts: 15 percent
Vermont: 13 percent
Rhode Island: 11 percent
Washington, D.C.: 5 percent
Illinois: 1 percent
The latest variant proportion estimates from the CDC show the omicron subvariant BA.2 accounts for more than one-third of COVID-19 cases nationwide and more than half of cases in the Northeast. Rhode Island has the highest proportion of BA.2 cases of all states, according to the latest ranking of states by the subvariant’s prevalence.
“If we maintain our preparedness, an increase in cases does not need to be a cause for alarm like it once was,” Jeff Zients, White House COVID-19 response coordinator, said in a March 23 media briefing. “We know what tools we need to fight the virus. Unfortunately, because of congressional action, we’re at risk of not having these tools readily available.”
President Joe Biden signed into law March 15 a sweeping $1.5 trillion bill that funds the government through September. The legislation did not include COVID-19 funding the White House had requested from Congress due to partisan disagreement about offsetting the funding.
There is no clear path to approval of more COVID-19 funding.
The lack of funding is affecting resources for COVID-19 testing and treatment. The Health Resources and Services Administration stopped accepting providers’ claims for COVID-19 testing and treatment of the uninsured March 22 due to a lack of sufficient funds. The federal government is also cutting back shipments of monoclonal antibody treatments to states by 30 percent, and the U.S. supply of those treatments could run out as soon as May.
As parents await an approved vaccine for children under 5, Moderna said on Wednesday a study had found its two-dose pediatric vaccine to be safe for young children, toddlers and babies. Its effectiveness, however, was complicated by the spread of the coronavirus’s omicron variant. While the pediatric vaccine generated an immune response equivalent to that of young adults before the highly transmissible variant emerged, those immune defenses were less strong in the face of omicron. In children, the pediatric vaccine was about 40 percent effective, Moderna said. The company plans to submit the data to the Food and Drug Administration for consideration in the coming weeks.
The FDA also faces requests to authorize a second booster vaccine dose for adults. But even if they are authorized, Biden administration officials said they lack the funds to purchase those shots. They said they’ve bought enough doses for Americans age 65 and older, as well as the potential initial regimen for children under 5, but can’t buy more doses for people in other age groups unless Congress passes a delayed $15 billion funding package. It’s not yet clear whether additional doses for adults will be necessary, but officials said placing orders for doses ahead of time has been an important lesson of the pandemic. White House officials have expressed worry that vaccine manufacturers will prioritize orders placed by other countries.
That concern comes as omicron’s BA.2 subvariant of the coronavirus now amounts to as much as 70 percent of new infections in much of the United States, according to the genomic surveillance company Helix. That version of the virus has prompted a surge of cases in Europe and fear that the United States will experience its own wave, similarly to how it has mirrored Europe in the past. A broad increase in cases has so far not happened in the United States, and disease experts don’t know for sure whether it will. If it does, it’s unclear whether the pandemic policies of the Biden administration and private institutions would substantially change.
A program to ensure global vaccine equity was doomed from the beginning to fall short, a Washington Post analysis found. The initiative, called Covax, was meant to convince wealthy and poor countries to combine their money to order vaccine doses in advance and then share them in a way that would protect the most vulnerable people first. But the program’s supporters underestimated the desperation of the wealthier countries, which snatched up doses from manufacturers for their own residents. Covax was also slow to adapt as nations declined to participate. Now, more than one-third of the world has not received a vaccine dose — a result that not only is inequitable, but also makes it easier for new variants to emerge.
In a study published Monday, people who had covid-19 had a 46 percent higher risk of developing Type 2 diabetes or being prescribed medication to control their blood sugar within a year than those who had not had the coronavirus. Greater severity of covid symptoms was associated with a higher chance of developing diabetes, but even people with less severe or asymptomatic infection had an increased risk, according to the study of more than 181,000 Department of Veterans Affairs patients. The study did not prove cause and effect but did show a strong association between covid-19 and diabetes.
Other important news
Omicron’s BA.2 subvariant has become the world’s dominant form of the coronavirus. The Post created a map and several charts to help you visualize how it’s spreading around the world.
White House press secretary Jen Psaki said Tuesday that she had tested positive for the coronavirus a second time. She had been scheduled to travel to Europe with President Biden and other administration officials, but canceled her trip.
A new omicron subvariant of the virus that causes COVID-19, BA.2, is quickly becoming the predominant source of infections amid rising cases around the world. Immunologists Prakash Nagarkatti and Mitzi Nagarkatti of the University of South Carolina explain what makes it different from previous variants, whether there will be another surge in the U.S. and how best to protect yourself.
What is BA.2, and how is it related to omicron?
BA.2 is the latest subvariant of omicron, the dominant strain of the SARS-CoV-2 virus that causes COVID-19. While the origin of BA.2 is still unclear, it has quickly become the dominant strain in many countries, including India, Denmark and South Africa. It is continuing to spread in Europe, Asia and many parts of the world.
The first omicron subvariant, BA.1, is unique in the number of alterations it has compared to the original version of the virus – it has over 30 mutations in the spike protein that helps it enter cells. Spike protein mutations are of high concern to scientists and public health officials because they affect how infectious a particular variant is and whether it is able to escape the protective antibodies that the body produces after vaccination or a prior COVID-19 infection.
BA.2 has eight unique mutations not found in BA.1, and lacks 13 mutations that BA.1 does have. BA.2 does, however, share around 30 mutations with BA.1. Because of its relative genetic similarity, it is considered a subvariant of omicron as opposed to a completely new variant.
While standard PCR tests are still able to detect the BA.2 variant, they might not be able to tell it apart from the delta variant.
Is it more infectious and lethal than other variants?
BA.2 is considered to be more transmissible but not more virulant than BA.1. This means that while BA.2 can spread faster than BA.1, it might not make people sicker.
Does previous infection with BA.1 provide protection against BA.2?
Yes! A recent study suggested that people previously infected with the original BA.1 subvariant have robust protection against BA.2.
Because BA.1 caused widespread infections across the world, it is likely that a significant percentage of the population has protective immunity against BA.2. This is why some scientists predict that BA.2 will be less likely to cause another major wave
However, while the natural immunity gained after COVID-19 infection may provide strong protection against reinfection from earlier variants, it weakens against omicron.
How effective are vaccines against BA.2?
A recent preliminary study that has not yet been peer reviewed of over 1 million individuals in Qatar suggests that two doses of either the Pfizer–BioNTech or Moderna COVID-19 vaccines protect against symptomatic infection from BA.1 and BA.2 for several months before waning to around 10%. A booster shot, however, was able to elevate protection again close to original levels.
Importantly, both vaccines were 70% to 80% effective at preventing hospitalization or death, and this effectiveness increased to over 90% after a booster dose.
How worried does the US need to be about BA.2?
The rise in BA.2 in certain parts of the world is most likely due to a combination of its higher transmissibility, people’s waning immunity and relaxation of COVID-19 restrictions.
CDC data suggests that BA.2 cases are rising steadily, making up 23% of all cases in the U.S. as of early March. Scientists are still debating whether BA.2 will cause another surge in the U.S.
Though there may be an uptick of BA.2 infections in the coming months, protective immunity from vaccination or previous infection provides defense against severe disease. This may make it less likely that BA.2 will cause a significant increase in hospitalization and deaths. The U.S., however, lags behind other countries when it comes to vaccination, and falls even further behind on boosters.
Whether there will be another devastating surge depends on how many people are vaccinated or have been previously infected with BA.1. It’s safer to generate immunity from a vaccine, however, than from getting an infection. Getting vaccinated and boosted and taking precautions like wearing an N95 mask and social distancing are the best ways to protect yourself from BA.2 and other variants.
Over the next few weeks, the U.S. should expect an increase in cases from the BA.2 variant, Dr. Anthony Fauci told ABC News, but it may not lead to as severe a surge in hospitalizations or deaths.
“I would not be surprised if in the next few weeks we see somewhat of either a flattening of our diminution or maybe even an increase,” Fauci told ABC News’ Brad Mielke on the podcast “Start Here.”
His prediction is based on conversations with colleagues in the U.K., which is currently seeing a “blip” in cases, Fauci said. The pandemic trajectory in the U.S. has often followed the U.K. by about three weeks.
However, he added, “Their intensive care bed usage is not going up, which means they’re not seeing a blip up of severe disease.”
The BA.2 variant, a more transmissible strain of omicron, now represents around 23% of all cases in the U.S., according to the latest data from the Centers for Disease Control and Prevention.
And while Fauci predicted that the BA.2 variant will eventually overtake omicron as the most dominant variant, it’s not yet clear how much of a problem that will be.
“Whether or not that is going to lead to another surge, a mini surge or maybe even a moderate surge, is very unclear because there are a lot of other things that are going on right now,” Fauci said.
Similar to the U.K., much of the U.S. has recently relaxed mitigation efforts like mask mandates and requirements for proof of vaccination. At the same time, people who were vaccinated over six months ago and still haven’t gotten a booster shot, which is about half of vaccinated Americans, according to the CDC, are facing continuously waning immunity.
It’s also not yet clear how long immunity from prior infection will last, Fauci said.
Taken together, it’s why Fauci and other experts, including CDC Director Rochelle Walensky, have increasingly predicted that elderly people will need a second booster shot soon. The Food and Drug Administration began reviewing data from Pfizer on the safety and efficacy this week, and its advisory panel will debate if and when the additional booster shot is necessary in the coming weeks.
At the same time, Fauci urged Americans who haven’t yet gotten their first booster, which would be their third shot in a Pfizer or Moderna series, to do so.
A resurgence of cases could also mean Americans are asked to wear masks again, which Fauci predicted would be an uphill battle.
“From what I know about human nature, which I think is pretty much a lot, people are kind of done with COVID,” Fauci said.
Still, he defended the CDC decision to loosen its mask recommendations earlier this month by shifting to a strategy that focused more on severe outcomes, like hospitalizations and deaths, rather than on daily case spread.
“You can go ahead and continue to tiptoe towards normality, which is what we’re doing, but at the same time, be aware that you may have to reverse,” Fauci said.
And if the U.S. does continue to make its way back toward normal times, Fauci himself has a personal choice to consider. At 81 years old, the director of the National Institute of Allergy and Infectious Diseases is “certainly” thinking about retirement.
“I have said that I would stay in what I’m doing until we get out of the pandemic phase and I think we might be there already, if we can stay in this,” Fauci said, referring to the falling cases and hospitalizations in the U.S.
“I can’t stay at this job forever. Unless my staff is gonna find me slumped over my desk one day. I’d rather not do that,” he said, laughing.
While he doesn’t currently have retirement plans, the recent hire of Dr. Ashish Jha, dean of the Brown University School of Public Health, to be White House coronavirus coordinator, could alleviate some of his pandemic response duties and give him a window.
But Fauci, who has dedicated his career to public health, primarily studying HIV and AIDS, and worked under seven U.S. presidents, said he doesn’t have any particular hobbies waiting for him in retirement.
“I, unfortunately, am somewhat of a unidimensional physician, scientist, public health person. When I do decide I’m going to step down, whenever that is, I’m going to have to figure out what it is I’m going to do,” he said.
“I’d love to spend more time with my wife and family. That would really be good.”
A surge in coronavirus infections in Western Europe has experts and health authorities on alert for another wave of the pandemic in the United States, even as most of the country has done away with restrictions after a sharp decline in cases.
Infectious-disease experts are closely watching the subvariant of omicron known as BA.2, which appears to be more transmissible than the original strain, BA.1, and is fueling the outbreak overseas.
In all, about a dozen nations are seeing spikes in coronavirus infections caused by BA.2, a cousin of the BA.1 form of the virus that tore through the United States over the past three months.
In the past two years, a widespread outbreak like the one now being seen in Europe has been followed by a similar surge in the United States some weeks later. Many, but not all, experts interviewed for this story predicted that is likely to happen. China and Hong Kong, on the other hand, are experiencing rapid and severe outbreaks, but the strict “zero covid” policies they have enforced make them less similar to the United States than Western Europe.
A number of variables — including relaxed precautions against viral transmission, vaccination rates, the availability of antiviral medications and natural immunity acquired by previous infection — may affect the course of any surge in the United States, experts said.
Most importantly, it is unclear at this point how many people will become severely ill, stressing hospitals and the health-care system as BA.1 did.
Another surge also may test the public’s appetite for returning to widespread mask-wearing, mandates and other measures that many have eagerly abandoned as the latest surge fades and spring approaches, experts said.
“It’s picking up steam. It’s across at least 12 countries … from Finland to Greece,” said Eric Topol, director of the Scripps Research Translational Institute in San Diego, who recently posted charts of the outbreak on Twitter. “There’s no question there’s a significant wave there.”
Topol noted that hospitalizations for covid-19, the disease caused by the virus, are rising in some places as well, despite the superior vaccination rates of many Western European countries.
At a briefing Monday, White House press secretary Jen Psaki said about 35,000 cases of BA.2 have been reported in the United States to date. But she offered confidence that “the tools we have — including mRNA vaccines, therapeutics and tests — are all effective tools against the virus. And we know because it’s been in the country.”
Kristen Nordlund, a spokeswoman for the Centers for Disease Control and Prevention, said in an email Tuesday that “although the BA.2 variant has increased in the United States over the past several weeks, it is not the dominant variant, and we are not seeing an increase in the severity of disease.”
The seven-day average of cases in the United States fell 17.9 percent in the past week, according to data tracked by The Washington Post, while the number of deaths dropped 17.2 percent and hospitalizations declined 23.2 percent.
Predicting the future course of the virus has proved difficult throughout the pandemic, and the current circumstances in Europe elicited a range of opinions from people who have closely tracked the pathogen and the disease it causes.
In the United States, just 65.3 percent of the population, 216.8 million people, are fully vaccinated, and only 96.1 million have received a booster shot, according to data tracked by The Post. In Germany, nearly 76 percent are fully vaccinated, according to the Johns Hopkins data, and the United Kingdom has fully vaccinated 73.6 percent.
That lower vaccination rate is very likely to matter as BA.2 spreads further in the United States, especially in regions where it is significantly lower than the national rate, several experts said. And even for people who are fully vaccinated and have received a booster shot, research data is showing that immunity to the virus fades over time. Vaccine-makers Pfizer and BioNTech asked the Food and Drug Administration on Tuesday for emergency authorization to offer a fourth shot to people 65 and older.
“Any place you have relatively lower vaccination rates, especially among the elderly, is where you’re going to see a bump in hospitalizations and deaths from this,” said Céline Gounder, an infectious-diseases physician and editor at large for public health at Kaiser Health News.
Similarly, as the public sheds masks — every state has dropped its mask mandate or announced plans to do so — another layer of protection is disappearing, several people tracking the situation said.
“Why wouldn’t it come here? Are we vaccinated enough? I don’t know,” said Kimberly Prather, a professor of atmospheric chemistry and an expert on aerosol transmission at the University of California at San Diego.
“So I’m wearing my mask still. … I am the only person indoors, and people look at me funny, and I don’t care.”
Yet BA.2 appears to be spreading more slowly in the United States than it has overseas, for reasons that aren’t entirely clear, Debbie Dowell, chief medical officer for the CDC’s covid-19 response, said in a briefing Saturday for clinicians sponsored by the Infectious Diseases Society of America.
“The speculation I’ve seen is that it may extend the curve going down, case rates from omicron, but is unlikely to cause another surge that we saw initially with omicron,” Dowell said.
One reason for that may be the immunity that millions of people acquired recently when they were infected with the BA.1 variant, which generally caused less-severe illness than previous variants. Yet no one really knows whether infection with BA.1 offers protection from BA.2.
“That’s the question,” said Jeffrey Shaman, an epidemiologist at the Columbia University Mailman School of Public Health. “Better yet, how long does it provide protection?”
Topol said the United States needs to improve its vaccination and booster rates immediately to protect more of the population against any coming surge.
“We have got to get the United States protected better. We have an abundance of these shots. We have to get them into people,” he said.
Biden administration officials said that whatever the further spread of BA.2 brings to the United States, the next critical step is to provide the $15.6 billion in emergency funding that Congress stripped from a deal to fund the government last week. That money was slated to pay for coronavirus tests, more vaccines and antiviral medications.
“That means that some programs, if we don’t get funding, could abruptly end or need to be pared back, Psaki said at Monday’s briefing. “And that could impact how we are able to respond to any variant.”
As the US approaches the grim statistic of one million deaths from COVID, journalist Ed Yong’s latest piece in The Atlantic takes a sobering look at how numb we’ve become to that astronomically high toll. In the early days of the pandemic, predictions of a few hundred thousand American deaths seemed shocking, but recent milestones of 800K and 900K lives lost have ticked by with little public attention.
Yong blames the invisibility of the virus: its worst impacts have been disproportionately concentrated among the disadvantaged—making it possible for COVID to more easily “disappear” from the lives of the healthy and economically advantaged. Case in point: while three percent of Americans have lost a close family member to COVID-19, the virus has taken a much larger toll on people of color, the elderly, and those with underlying health conditions.
The Gist:The pandemic has rendered us numb to the ongoing tragic loss of life, leading us to accept over 1,500 COVID deaths each day as “normal”.
As Yong points out, it’s hard to imagine we could turn a blind eye to this number of Americans perishing every day, compared to the number who perish from hurricanes or other weather disasters, for example. While permanent memorials are built for soldiers and victims of terror attacks, they are rarely erected for victims or medical heroes of pandemics, despite the far greater death toll.
While the pandemic is still far from over, we must ensure the difficult lessons learned are not forgotten by future generations—as has been the case with previous pandemics.
Congress cut billions of dollars in COVID-related funding from the broader government spending bill it just passed, jeopardizing President Biden’s plans for covering the costs of COVID testing and treatments, and making antiviral drugs available for free at pharmacies for those who test positive through the “test to treat” initiative.
However, a variety of other healthcare funding made it into the final package, including a five-month extension of COVID-era telehealth flexibilities for Medicare beneficiaries, and funds for pandemic preparedness. Congressional Democrats now plan to pass a separate COVID funding bill, although that effort will likely face stiff opposition from Senate Republicans.
The Gist: Removing COVID funding from the final spending package may signal the beginning of the end of federal pandemic relief spending, and could render the “test to treat” initiative, which has been praised by public health experts, dead on arrival.
Pharmacists, who have taken on a larger role in patient care during the pandemic, assisting with testing and vaccination of millions of Americans, have pushed for the ability to prescribe new antiviral therapies, but the American Medical Association criticized the initiative, maintaining that physicians should control the prescribing. Although the drug interactions and side effects cited by the AMA are important to manage, pharmacy-based “test to treat”would reduce time to treatment for those with COVID, and provide a sustainable mechanism for managing future surges of the disease.
The House passed a sweeping spending bill last night that omitted billions in Covid-19 aid. Biden administration officials had said the funds were urgently needed to maintain supplies of essential treatments and support further vaccine development, but Republicans disagreed. Some public health experts have expressed dismay that the pandemic relief money was cut, given the likelihood that new variants will continue to emerge. After all, viruses keep evolving until they run out of hosts to infect, and there are billions of people around the world—and millions in the US—who haven’t been vaccinated against Covid-19.
Cases continue to decline in the US, and a number of top voices in public health recently put out a report mapping when and how the country can transition out of the pandemic. Their recommendations include vaccinating at least 85 percent of the US population by 2023, improving indoor air quality in public buildings, and allocating additional funding for Covid-19 response and to prepare for future pandemics.
Welcome to Friday’s Health 202, where today we have a special spotlight on the pandemic two years in.
🚨 The federal government is about to be funded. The Senate sent the long-term spending bill to President Biden’s desk last night after months of intense negotiations.
Two years since the WHO declared a pandemic, what health-care system changes are here to stay?
Nurses screened patients at a drive-through testing site in March 2020. (Win McNamee/Getty Images)
Exactly two years ago, the World Health Organizationdeclared the coronavirus a pandemic and much of American life began grinding to a halt.
That’s when the health-care system, which has never been known for its quickness, sped up. The industry was forced to adapt, delivering virtual care and services outside of hospitals on the fly. Yet, the years-long pandemic has exposed decades-old cracks in the system, and galvanized efforts to fix them.
Today, as coronavirus cases plummet and President Biden says Americans can begin resuming their normal lives, we explore how the pandemic could fundamentally alter the health-care system for good. What changes are here to stay — and what barriers are standing in the way?
A telehealth boom
What happened: Telehealth services skyrocketed as doctors’ offices limited in-person visits amid the pandemic. The official declaration of a public health emergency eased long-standing restrictions on these virtual services, vastly expanding Medicare coverage.
But will it stick? Some of these changes go away whenever the Biden administration decides not to renew the public health emergency (PHE). The government funding bill passed yesterday extends key services roughly five months after the PHE ends, such as letting those on Medicare access telehealth services even if they live outside a rural area.
But some lobbyists and lawmakers are pushing hard to make such changes permanent. Though the issue is bipartisan and popular, it could be challenging to pass unless the measures are attached to a must-pass piece of legislation.
“Even just talking to colleagues, I used to have to spend three or four minutes while they were trying desperately not to stare at their phone and explain to them what telehealth was … remote patient monitoring, originating sites, and all this wonky stuff,”said Sen. Brian Schatz (D-Hawaii), a longtime proponent of telehealth.
“Now I can go up to them and say, ‘So telehealth is great, right?’ And they say, ‘yes, it is.’ ”
A new spotlight on in-home care
What happened: The infectious virus tore through nursing homes, where often fragile residents share rooms and depend on caregivers for daily tasks. Ultimately, nearly 152,000 residents died from covid-19.
The devastation has sparked a rethinking of where older adults live and how they get the services they need — particularly inside their own homes.
“That is clearly what people prefer,” said Gail Wilensky, an economist at Project HOPE who directed the Medicare and Medicaid programs under President George H.W. Bush. “The challenge is whether or not it’s economically feasible to have that happen.”
More money, please: Finding in-home care — and paying for it — is still a struggle for many Americans. Meanwhile, many states have lengthy waitlists for such services under Medicaid.
Experts say an infusion of federal funds is needed to give seniors and those with disabilities more options for care outside of nursing homes and assisted-living facilities.
For instance, Biden’s massive social spending bill included tens of billions of dollars for such services. But the effort has languished on Capitol Hill, making it unclear when and whether additional investments will come.
A reckoning on racial disparities
What happened: Hispanic, Black, and American Indian and Alaska Native people are about twice as likely to die from covid-19 than White people. That’s according to age-adjusted data from a recent Kaiser Family Foundation report.
In short, the coronavirus exposed the glaring inequities in the health-care system.
“The first thing to deal with any problem is awareness,” said Georges Benjamin, the executive director of the American Public Health Association. “Nobody can say that they’re not aware of it anymore, that it doesn’t exist.”
But will change come? Health experts say they hope the country has reached a tipping point in the last two years. And yet, any real systemic change will likely take time. But, Benjamin said, it can start with increasing the number of practitioners from diverse communities, making office practices more welcoming and understanding biases.
We need to, as a matter of course, ask ourselves who’s advantaged and who’s disadvantaged” when crafting new initiatives, like drive-through testing sites, Benjamin said. “And then how do we create systems so that the people that are disadvantaged have the same opportunity.”
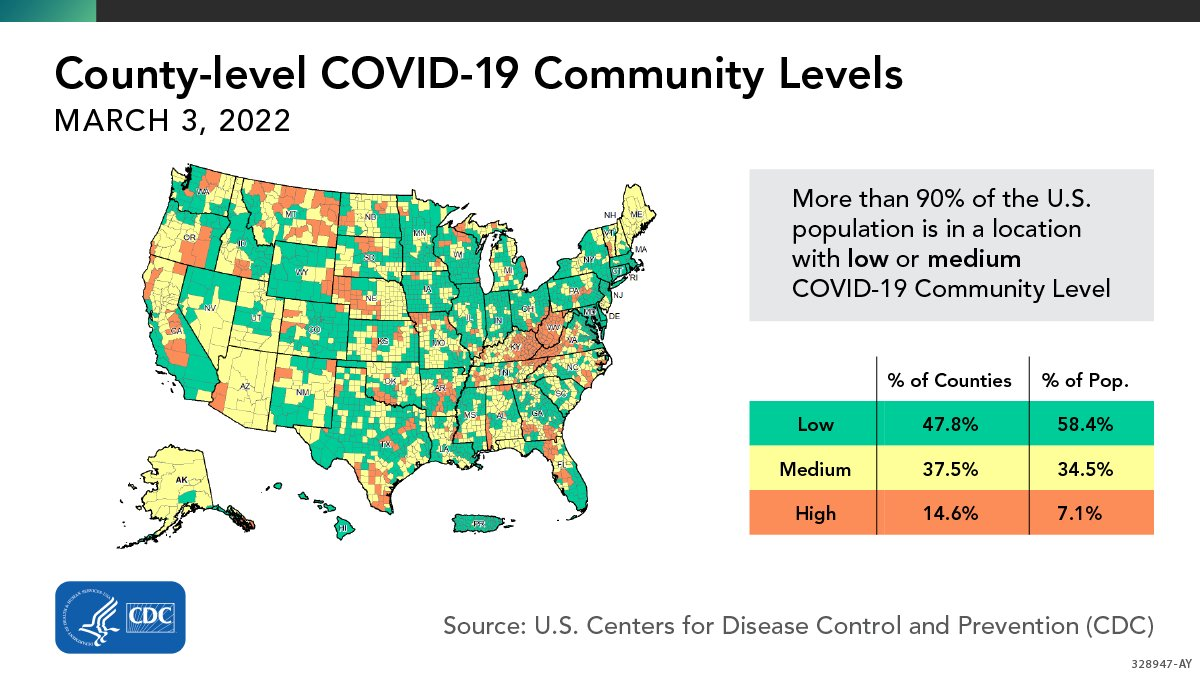
More than 90% of the U.S. population lives in an area with a “low” or “medium” risk of COVID-19, the U.S. Centers for Disease Control and Prevention (CDC) announced yesterday. Last week, the CDC changed the way it assesses county-level COVID-19 risk, using data on hospitalizations and health care capacity in addition to case counts. The CDC now recommends universal indoor masking only for counties that are at “high” risk under this system—which means that the vast majority of Americans are not currently advised to wear masks inside.