Employers face a brutal increase in health-insurance premiums for 2023, Axios’ Arielle Dreher writes from a Kaiser Family Foundation report out this morning.
Why it matters: Premiums stayed relatively flat this year, even as wages and inflation surged. That reprieve was because many 2022 premiums were finalized last fall, before inflation took off.
“Employers are already concerned about what they pay for health premiums,” KFF president and CEO Drew Altman said.
“[B]ut this could be the calm before the storm … Given the tight labor market and rising wages, it will be tough for employers to shift costs onto workers when costs spike.”
🧠 What’s happening: Nearly 159 million Americans get health coverage through work — and coverage costs and benefits have become a critical factor in a tight labor market.
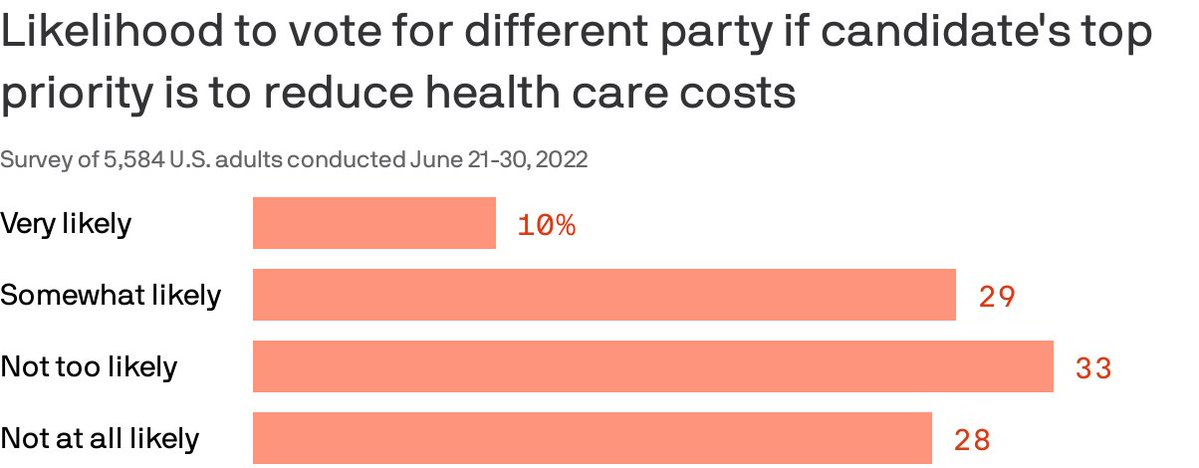
Almost 40% of Americans are willing to split their ticket and vote for a candidate from the opposing party who made a top priority of lowering health costs, according to a Gallup/West Health poll published Thursday.
Why it matters: Though candidates haven’t been talking much about medical costs in the run-up to the midterms, the issue remains enough of a priority that it could erode straight party-line voting.
By the numbers: 87% of Americans polled said a candidate’s plan to reduce the cost of health care services was very or somewhat important in casting a vote.
The issue cut across partisan lines, with 96% of Democrats and 77% of Republican respondents saying a candidate with a health care costs plan was an important factor.
86% also said a plan to lower prescription drug prices is very or somewhat important. That’s especially true for seniors.
Of note: Democratic voters were more likely than Republicans to say they would cross party lines because health costs are a top priority. Four in 10 Democrats said they were likely to do so compared to about 1 in 5 Republicans.
Amid new price transparency laws and growing consumer demand, more hospitals are adding cash pay options for certain health care services instead of just accepting insurance, Nora Tepper writes for Modern Healthcare—and some hospital officials say these offerings are “only going to go up” in the future.
How an ‘anomaly’ is becoming more common
Providers advertising cash pay rates for their services used to be considered an “anomaly,” Tepper writes. Now, the No Surprises Act, the federal price transparency law, and changing consumer expectations may make cash-only payments for health care services more common.
“The market is going there,” said Larry Van Horn, associate professor of management, law, and health policy and executive director of health affairs at Vanderbilt University. “You’ve got direct primary care, you’ve got physicians going and moving into cash pay. You’re gonna have to sit there at some point and say, ‘Wait a minute, they’re taking my business.'”
Although some hospitals and health systems that serve certain populations—such as Pomerene Hospital in Ohio with Amish and Anabaptist patients and the University of Texas MD Anderson Cancer Center with medical tourists—have long had cash-pay systems, it is still a relatively new concept for most providers in the United States.
According to data from Medscape, which surveyed more than 17,000 clinicians, just 17% of clinicians used cash-only, concierge, or direct-pay primary care models in 2020. Primary care providers (PCPs) made up the largest proportion of providers accepting cash pay, with 10% of practices charging patients a flat monthly fee for unlimited services.
“[S]ome providers embracing the cash pay revolution say their bottom line benefits from faster reimbursement, lower administration costs and higher patient retention,” Tepper writes.
In a 2020 report from the Society of Actuaries, almost all PCPs who operated under self-pay models reported “better or much better” personal and professional satisfaction compared to those under a traditional fee-for-service system. In addition, 34% of respondents reported “better or much better” earnings under a direct payment model.
How patients could benefit from cash-pay systems
According to Tepper, hospitals generally offer self-paying patients, who have typically been uninsured individuals or those with high-deductible health plans, lower rates for services compared to commercial insurers since they don’t have to handle administrative work or collections.
In a 2021 study published in JAMA Network Open, researchers analyzed rates for “shoppable” services at 922 hospitals and found that the proportion of hospitals that had lower cash prices than their median commercial negotiated rate ranged from 38.4% for liver tests to 68.5% for C-sections.
During the pandemic, more insured patients began to inquire about what services they could pay cash for, leading some health systems to create new payment models for certain procedures.
For example, Deaconess Health System launched an in-house bundled payment program, which includes cardiology, radiology, and urgent care services, in July 2020. The first year, the health system sold 130 bundled services, which increased to 351 in 2021, and 489 as of August 2022.
For any services not covered by the program, Deaconess offers a 50% discount on cash payments compared to its insurer rate. However, self-paying patients are required to pay the full cost of a procedure upfront.
“The patient has decided to take a bet on themselves,” said Steve Russell, VP and chief revenue cycle officer at Deaconess. “They have a high deductible, they don’t think they’re going to reach that threshold and their thought is, ‘If I don’t use my insurance, what kind of discount can you give me?'”
Separately, CommonSpirit Health‘s Catholic Health Initiatives (CHI) launched its own bundled cash price program in 2018 after noticing that many patients with high-deductible plans would defer care due to affordability concerns. The health system also advertises and sells its services on MDsave, an online marketplace that allows consumers to shop for health care procedures.
“With the No Surprises Act and the price transparency regulations, this has to be something that we offer,” said Jeanette Wojtalewicz, SVP and CFO at CHI Health’s Midwest division. “You’ll see more of this coming.”
The future of cash-pay systems in hospitals
According to Aaron Miri, SVP and chief digital and information officer at Baptist Health South Florida, although few patients are currently paying directly for health care services, the industry is heading towards that direction, which means health systems need to be prepared to meet the demand.
“When you look at the directionality of demand, this is only going to go up,” Miri said. “Patients are going to start seeing their total estimated bill and say, ‘I want to spend my $500 at a health system that was really transparent with me, and made me feel comfortable, versus the health system down the road that I’ve always gone to, but that simply can’t tell me what my actual amount due is.”
To make it easier for patients to directly pay for procedures, some health systems, including Baptist Health, have updated their payment options by adding Apple Pay, Google Pay, or other online payment systems instead of just accepting payment in-person or by phone.
However, even as direct payment models become more common, some insurers are “using their leverage to slow adoption of cash pay,” Tepper writes.
Kimberly Scaccia, VP of revenue management at MercyHealth, said some of the health system’s contracts with insurers prohibit it from offering cash discounts to insured patients.
“Some of the smaller payers, they’re fine with removing [cash pay restrictions],” Scaccia said. “Some of the very, very large payers, they simply will not allow it.”
In addition, Matthew Fiedler, a senior fellow of economic studies at the USC-Brookings Schaeffer Initiative for Health Policy, said clinicians may also be concerned about insurers asking to pay the lower cash rate during contract renewals or jeopardizing a provider’s network position.
“An insurer could say, ‘We’re gonna put this provider out-of-network, but we’re gonna put them in a preferred out-of-network position in our benefit design, where the cost-sharing is not that onerous, because we know they have this really good cash price,'” Fiedler said.
From the spring of 2021 through June of this year, the U.S. has been in a period of high and rising economywide price inflation. Pressures such as labor scarcities, global energy interruptions, and supply chain disruptions have made everything from consumer goods to business services more expensive. Yet, in our ongoing series of Health Sector Economic Indicators (HSEI) briefs, we have been detailing data that find, quite surprisingly, overall inflation for the health care sector—as measured by the aggregate Health Care Price Index (HCPI)—has remained in a very tight and modest range, rarely exceeding three percent year-over-year growth or falling beneath two percent growth. In our monthly briefs, we have explored how factors such as the time it takes for new contracts and reimbursement rates to take effect and recent policy changes restraining public health care costs have kept overall health care inflation well below economywide rates. As these factors continue to play out, the recently-released July price data are revealing what may be a key inflection point in Medicare and private insurance prices for health care services.
In July, the prices paid for many types of health care from these two major payer types diverged substantially. Medicare prices fell by nearly a full percentage point, putting overall Medicare services prices below the levels seen back in January 2021 (Exhibit 1). These declining Medicare prices are due to two major factors: very low or no increases in the statutory reimbursement rates for hospital care and physician services in the calendar year 2022 and the re-institution of the mandated sequestration cuts for Medicare provider payments in April and July of this year. These sequestration cuts, which had been postponed for many years since they were updated in 2011, are having a meaningful impact as seen in the chart below (click on link above). The impact of the two sequestration cuts can be seen clearly in the data, pulling down Medicare prices between March and April and then between June and July across all three major settings of care as first a 1% and then a 2% cut were put in place. Due to the fact that physician services received relatively smaller baseline increases in new Medicare rates for 2022, the sequestration cuts have pulled those price levels the lowest, down by 2.2% since January 2021. Medicare price changes for nursing homes care fall in between hospitals and physician services, down by 1.0% since January 2021.
At the same time Medicare prices are falling, the prices for similar types of care paid by private insurance increased substantially in July, up a full percentage point from the previous month and 5.4% higher than the price levels in January 2021 (Exhibit 2). We believe many of these increases are occurring as new contracts or updated rates are slowly taking effect, and further expect there may be a noticeable discrete jump in private prices beginning in 2023, as recent comments from providers and insurers are stating 2023 negotiations are generally favoring providers. We can see in the data that it appears hospitals are experiencing much higher private price growth than other components (up 7.2% since January 2021) and faster recent growth, with price levels increasing by nearly a full percentage point in each of the past three months. Physician services are the next fastest growing component, while nursing home private prices have barely moved since the beginning of 2021. Faster increases in hospital prices may indicate stronger negotiating positions for those providers, particularly given ongoing consolidation in the industry over the past ten years.
When looking at the HCPI in aggregate, these two diverging trends have been cancelling out, leading to overall moderate growth in health care prices. Yet, these detailed, by-payer data indicate that significant trends in health care prices are occurring underneath, with the long-expected increases in private prices beginning to follow overall economywide inflation trends. All else equal, these price increases in care paid by private insurance will further exacerbate an already wide gap between public and private prices. This is especially true for hospital care, where the disparity between Medicare and private prices diverged by a whopping 7.2 percentage points in the last eighteen months. The most important factors driving the trends going forward for private prices will be the extent to which overall economywide inflation slows and who has the balance of power in insurer/provider contract negotiations. For public prices, government policy decisions will continue to be most important influencer of their growth. We expect to follow all these factors and the overall impact of the diverging data on overall health sector inflation in our ongoing series of HSEI briefs through the rest of the year and into 2023.
Despite the hype, accountable care organizations (ACOs) and other Medicare-driven payment reform programs intended to improve quality and lower healthcare spending haven’t bent the cost curve to the extent many had hoped.
A recent and provocative opinion piece in STAT News, from health policy researcher Kip Sullivan and two single-payer healthcare advocates, calls for pressing pause on value-based payment experimentation. The authors argue that current attempts to pay for value have ill-defined goals and hard-to-measure quality metrics that incentivize reducing care and upcoding, rather than improving outcomes.
The Gist: We agree with the authors that current value-based care experiments have been disappointing.
The intention is good, but the execution has been bogged down by entrenched industry dynamics and slow-to-move incumbents. One fair criticism: ACOs and other “total cost management” reforms largely focus on the wrong problem. They address utilization, rather than excessive price.
But we’re having a price problem in the US, not a utilization problem.Europeans, for example, have more physician visits each year than Americans, yet spend less per-person on healthcare. It’s our high prices—for everything from physician visits to hospital stays to prescription drugs—that drive high healthcare spending.
The root cause: our third-party payer structure actively discourages real efforts to lower price—every player in the value chain, including providers, brokers, and insurers, does better economically as prices increase. That’s why price control measures like reference pricing or price caps have been nonstarters among industry participants.
Recent reforms that increase price transparency, while not the entire solution, at least shine a light on the real challenges our healthcare system faces.
After a few years of relatively unchanged monthly premiums, a Kaiser Family Foundation analysis of 72 rate filings for 2023 finds a median 10 percent increase. Insurers say the biggest driver is rising medical costs, driven by higher rates for provider services and pharmaceuticals, as well as a return to pre-pandemic utilization levels. Insurers aren’t expecting COVID-19 or federal policy changes—including a potential extension of enhanced subsidies—to have much of an impact on rates.
The Gist:High inflation and the growing wage-price spiral have left providers with much higher costs, which is sure to drive up the overall cost of healthcare. Where provider systems have the leverage to demand higher rates from insurers, this will inevitably drive up premiums—an effect that is already starting to show up in the individual insurance market.
If Congressional Democrats are able to extend ACA subsidies, most ACA enrollees won’t actually feel these premium increases, but as contracts in the group market come up for renewal, we’d expect inflation in employer-sponsored premiums as well. Given the cost-sharing now built into most benefit plans, individual consumers will likely see healthcare join gas, food, and housing as household costs that are experiencing unsustainable inflationary increases.
Healthcare costs are becoming an increasing source of stress for older Americans, leading to some paring back on treatment, medicines or other spending on food and utilities — or skipping them altogether — to cover medical costs, according to new research conducted by Gallup in partnership with West Health.
The survey of U.S. adults released Wednesday found that almost half of adults aged 50 to 64 and more than a third of adults 65 and older are concerned they won’t be able to pay for needed healthcare services in the next year. That’s nearly 50 million older Americans.
About 80 million adults above age 50 see healthcare costs as a financial burden. Becoming eligible for Medicare seems to assuage those worries slightly, however: 24% of adults aged 50 to 64, who are not yet eligible for the federal health insurance, said health costs were a major burden. That percentage fell to 15% for those aged 65 and above.
Dive Insight:
The West Health-Gallup survey, conducted in September and October of 2021, is the latest vignette of how exorbitant healthcare costs in the U.S. are increasingly impacting the financial stability of Americans, especially those of retirement age who are more likely to have expensive medical needs.
Out-of-pocket healthcare expenses for adults aged 65 and older increased 41% from 2009 to 2019, according to HHS data. That population spends on average almost double their total expenditures on healthcare costs compared with the general population, despite Medicare coverage.
That cost problem is only likely to worsen amid surging inflation raising the cost of groceries, gas and other needed items. Additionally, U.S. demographics shifts are an added stressor. By 2030, the percentage of Americans 65 years and older will outweigh those under the age of 18, a first in the country’s history, according to Census Bureau projections.
“As sizable numbers of Americans 65 and older face tangible tradeoffs to pay for healthcare, many more Americans in the next decade will incur health and financial consequences because of high costs,” researchers wrote in the report.
The West Health-Gallup poll found about one in four adults aged 65 and above cut back on food, utilities, clothing or medication to cover healthcare costs. That’s compared to three in 10 for adults aged 50 to 64.
Older women and Black adults were more likely to forgo basic necessities to pay for healthcare than other demographics.
More than 20 million Americans aged 50 years and above said there was a time within the last three months when they or a family member was sick, but didn’t seek treatment due to cost.
More than 15 million Americans said they or a family member skipped a pill or dose of prescribed medicine in order to save money.
Researchers urged policymakers to act to improve efficiency and reduce the costs of medical care and prescription drugs in the U.S. Congress has yet to take meaningful action to lower medical costs, despite rising support for government intervention and high-profile proposals from the Biden administration.
Private insurers pay high and rising prices to hospitals. But whether this is “good” or “bad” depends on what’s behind this phenomenon. Do high prices reflect investments in quality? Or do they instead reflect issues like lack of competition due to hospital consolidation? The answer matters for efforts to reduce health care spending.
In a new paper in the Journal of Health Economics, Craig Garthwaite, Christopher Ody and Amanda Starc investigated whether the prospect of financial rewards drove differences in hospital quality measures — including things like mortality rates, patient experience, technology adoption and emergency department wait times. Specifically, the authors’ examined whether hospitals are more likely to invest in quality if they will be rewarded through higher prices. This is more feasible if they’re serving lots of commercially insured patients, since private insurers may pay higher rates if patients value those hospitals. But that strategy may not be successful in areas with large shares of the population on Medicare and Medicaid, which do not negotiate prices.
The researchers found that:
Hospitals in areas with more privately insured patients had higher quality scores compared to hospitals with more publicly insured patients.
Hospitals targeting more privately insured patients also had higher costs than those relying more on payers like Medicare and Medicaid.
These results suggest hospitals make strategic investments in quality to attract privately insured patients. This is consistent with what one might expect from market competition and the results of other recent research. These findings do not, however, imply that prices are “optimal.” Prices also reflect factors like provider consolidation that have little observable effects on quality. Indeed, hospital prices likely reflect a mix of valuable and wasteful spending.
The analysis does have limitations. The authors used the demographics of the areas around the hospital instead of each hospital’s actual potential mix of patients. In addition, it is possible that some quality differences across hospitals actually reflect differences between patients with private and public insurance which aren’t easy to capture in data. However, the authors’ results were similar across several quality measures, including those where this is less of a concern.
These results can help better inform efforts to reduce health care costs. Policymakers interested in reducing hospital prices should be aware that doing so might reduce investments in quality. This suggests placing a greater emphasis on policies that target prices stemming from clear sources of inefficiencies, like consolidation, since such tradeoffs are likely smaller.