On Thursday, the Biden administration issued the first of what is expected to be a series of new regulations aimed at implementing the No Surprises Act, passed by Congress last year and signed into law by President Trump, which bans so-called “surprise billing” by out-of-network providers involved in a patient’s in-network hospital visit.
The interim final rule, which takes effect in 2022, prohibits surprise billing of patients covered by employer-sponsored and individual marketplace plans, requiring providers to give advance warning if out-of-network physicians will be part of a patient’s care, limiting the amount of patient cost-sharing for bills issued by those providers, and prohibiting balance billing of patients for fees in excess of in-network reimbursement amounts.
The rule also establishes a process for determining allowable rates for out-of-network care, involving comparison to prevailing statewide rates or the involvement of a neutral arbitrator, but falls short of specifying a baseline price for arbitrators to use in determining allowable charges. That methodology, along with other details, will be part of future rulemaking, which will be issued later this year.
Of note, the rule does not include a ban on surprise billing forground ambulance services, which were excluded by Congress in the law’s final passage—even though more than half of all ambulance trips result in an out-of-network bill. Expect intense lobbying by industry interests to continue as the details of future rulemaking are worked out, as has been the case since before the law was passed.
While burdensome for patients,surprise billing has become a lucrative business model for some large, investor-owned specialist groups, who will surely look to minimize the law’s impact on their profits.
The complexity of Medicare Advantage (MA) physician networks has been well-documented, but the payment regulations that underlie these plans remain opaque, even to experts. If an MA plan enrollee sees an out-of-network doctor, how much should she expect to pay?
The answer, like much of the American healthcare system, is complicated. We’ve consulted experts and scoured nearly inscrutable government documents to try to find it. In this post we try to explain what we’ve learned in a much more accessible way.
Medicare Advantage Basics
Medicare Advantage is the private insurance alternative to traditional Medicare (TM), comprised largely of HMO and PPO options. One-third of the 60+ million Americans covered by Medicare are enrolled in MA plans. These plans, subsidized by the government, are governed by Medicare rules, but, within certain limits, are able to set their own premiums, deductibles, and service payment schedules each year.
Critically, they also determine their own network extent, choosing which physicians are in- or out-of-network. Apart from cost sharing or deductibles, the cost of care from providers that are in-network is covered by the plan. However, if an enrollee seeks care from a provider who is outside of their plan’s network, what the cost is and who bears it is much more complex.
Provider Types
To understand the MA (and enrollee) payment-to-provider pipeline, we first need to understand the types of providers that exist within the Medicare system.
Participating providers, which constitute about 97% of all physicians in the U.S., accept Medicare Fee-For-Service (FFS) rates for full payment of their services. These are the rates paid by TM. These doctors are subject to the fee schedules and regulations established by Medicare and MA plans.
Non-participating providers (about 2% of practicing physicians) can accept FFS Medicare rates for full payment if they wish (a.k.a., “take assignment”), but they generally don’t do so. When they don’t take assignment on a particular case, these providers are not limited to charging FFS rates.
Opt-out providersdon’t accept Medicare FFS payment under any circumstances. These providers, constituting only 1% of practicing physicians, can set their own charges for services and require payment directly from the patient. (Many psychiatrists fall into this category: they make up 42% of all opt-out providers. This is particularly concerning in light of studies suggesting increased rates of anxiety and depression among adults as a result of the COVID-19 pandemic).
How Out-of-Network Doctors are Paid
So, if an MA beneficiary goes to see an out-of-network doctor, by whom does the doctor get paid and how much? At the most basic level, when a Medicare Advantage HMO member willingly seeks care from an out-of-network provider, the member assumes full liability for payment.That is, neither the HMO plan nor TM will pay for services when an MA member goes out-of-network.
The price that the provider can charge for these services, though, varies, and must be disclosed to the patient before any services are administered. If the provider is participating with Medicare (in the sense defined above), they charge the patient no more than the standard Medicare FFS rate for their services. Non-participating providers that do not take assignment on the claim are limited to charging the beneficiary 115% of the Medicare FFS amount, the “limiting charge.” (Some states further restrict this. In New York State, for instance, the maximum is 105% of Medicare FFS payment.) In these cases, the provider charges the patient directly, and they are responsible for the entire amount (See Figure 1.)
Alternatively, if the provider has opted-out of Medicare, there are no limits to what they can charge for their services. The provider and patient enter into a private contract; the patient agrees to pay the full amount, out of pocket, for all services.
Figure 1: MA HMO Out-of-Network Payments
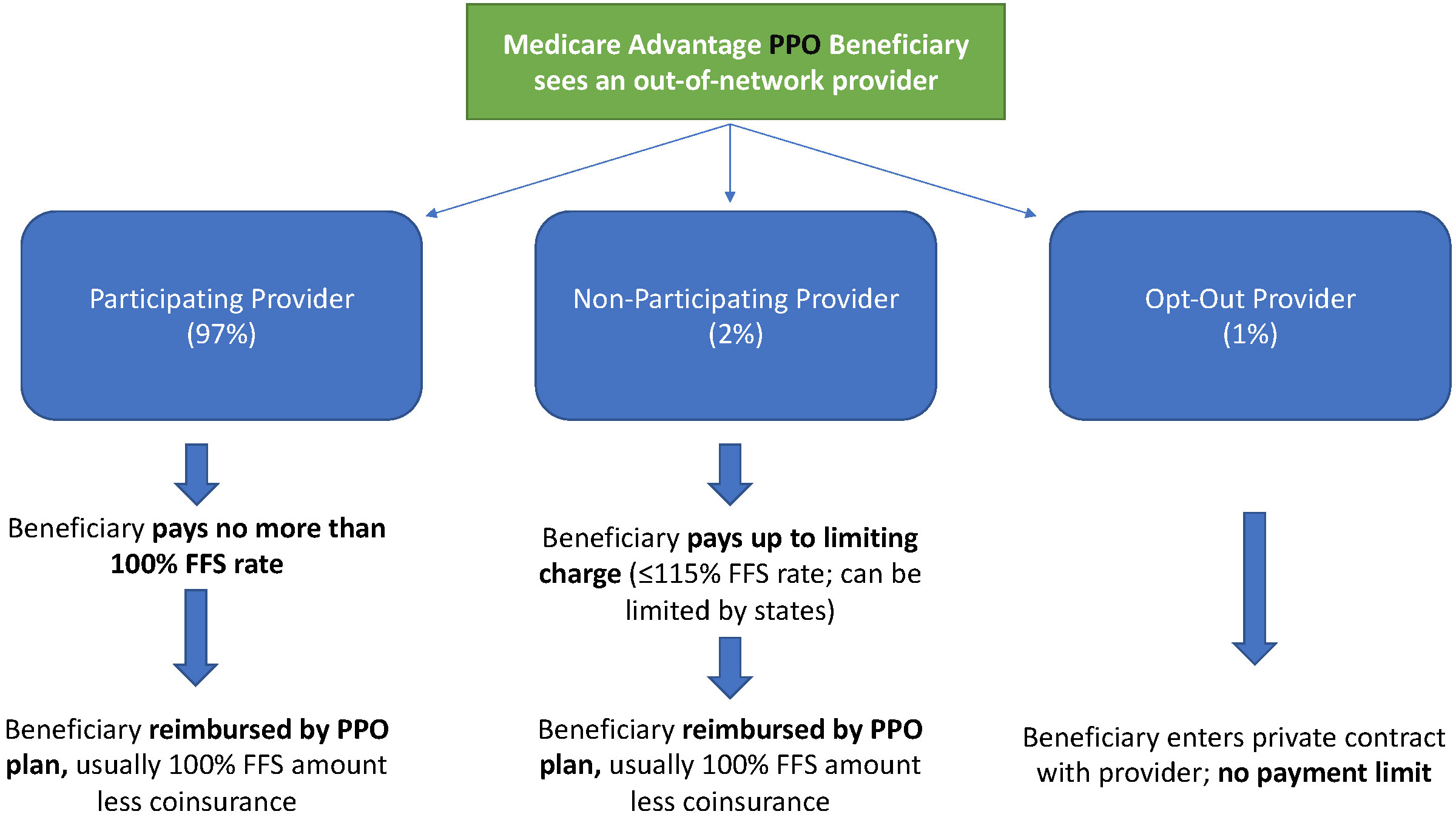
MA PPO plans operate slightly differently. By nature of the PPO plan, there are built-in benefits covering visits to out-of-network physicians (usually at the expense of higher annual deductibles and co-insurance compared to HMO plans). Like with HMO enrollees, an out-of-network Medicare-participating physician will charge the PPO enrollee no more than the standard FFS rate for their services. The PPO plan will then reimburse the enrollee 100% of this rate, less coinsurance. (See Figure 2.)
In contrast, a non-participating physician that does not take assignment is limited to charging a PPO enrollee 115% of the Medicare FFS amount, which can be further limited by state regulations. In this case, the PPO enrollee is also reimbursed by their plan up to 100% (less coinsurance) of the FFS amount for their visit. Again, opt-out physicians are exempt from these regulations and must enter private contracts with patients.
Figure 2: MA PPO Out-of-Network Payments
Some Caveats
There are two major caveats to these payment schemes (with many more nuanced and less-frequent exceptions detailed here). First, if a beneficiary seeks urgent or emergent care (as defined by Medicare) and the provider happens to be out-of-network for the MA plan (regardless of HMO/PPO status), the plan must cover the services at their established in-network emergency services rates.
The second caveat is in regard to the declared public health emergency due to COVID-19 (set to expire in April 2021, but likely to be extended). MA plans are currently required to cover all out-of-network services from providers that contract with Medicare (i.e., all but opt-out providers) and charge beneficiaries no more than the plan-established in-network rates for these services. This is being mandated by CMS to compensate for practice closures and other difficulties of finding in-network care as a result of the pandemic.
Conclusion
Outside of the pandemic and emergency situations, knowing how much you’ll need to pay for out-of-network services as a MA enrollee depends on a multitude of factors. Though the vast majority of American physicians contract with Medicare, the intersection of insurer-engineered physician networks and the complex MA payment system could lead to significant unexpected costs to the patient.
In their recent Health Affairs paper, Sungchul Park and coauthors examine rates of switching from Medicare Advantage (MA) to traditional Medicare by patient characteristics. MA plans are the private insurance alternative to traditional fee-for-service Medicare overseen by the Centers for Medicare and Medicaid Services. While enrollment in MA has doubled over the past decade, Park and coauthors find that the needs of certain enrollees are not being met by MA plans.
Park and coauthors report that rural enrollees switch from MA to traditional Medicare at an adjusted annual rate of 10.5 percent, significantly higher than metropolitan residents, who switch at a rate of 5.0 percent.
This phenomenon was more pronounced among those who required the use of costly services such as facility stays or hospitalizations, those who had poor self-reported health, and individuals who reported lower satisfaction with their access to care.
A San Francisco Superior Court judge has granted preliminary approval of the $575 million settlement agreement Sutter Health reached in the antitrust case that alleges it drove up healthcare prices in Northern California through anticompetitive practices.
A hearing for final approval of the settlement has been set for July 19, according to the judge’s order issued Tuesday.
Now, class members, or certain self-funded payers in California, will be notified of the preliminary approval and may object to part or all of the settlement agreement.
Dive Insight:
This preliminary approval comes more than a year after Sutter Health first agreed to settle the case with the plaintiffs, including California Attorney General Xavier Becerra, now nominee for HHS secretary, and a grocer’s union.
To put the settlement and all its elements in motion, it must first be approved by a judge. Tuesday’s order moves the case one step closer to final approval.
That 2019 settlement came on the eve of a court case that was supposed to lay out in open court how the regional powerhouse’s practices led to higher healthcare costs.
Even though the settlement averted a trial, it was designed to force Sutter to change some of these practices. As part of the settlement, Sutter agreed to stop “all-or-nothing” contracting and instead allow insurers and other payers to contract with some, but not all, of Sutter’s facilities.
The settlement is also designed to limit what patients pay out-of-network in an effort to shield them from exorbitant, surprise medical bills.
Sutter Health has tried to delay the $575 million antitrust settlement, citing the fallout from the novel coronavirus that has squeezed providers, including Sutter.
The health system, though battered by the pandemic’s fallout, was still able to post net income of $134 million for 2020, in part thanks to investment income. However, it did report an operating loss of $321 million as expenses outpaced revenue. Sutter said it was launching a sweeping review of its finances and operations as a result.
The litigation was first initiated in 2014 when the grocer’s union, joined by other plaintiff’s, filed suit against Sutter’s practices. It ultimately drew the attention of Becerra’s office.
The complexity of Medicare Advantage (MA) physician networks has been well-documented, but the payment regulations that underlie these plans remain opaque, even to experts. If an MA plan enrollee sees an out-of-network doctor, how much should she expect to pay?
The answer, like much of the American healthcare system, is complicated. We’ve consulted experts and scoured nearly inscrutable government documents to try to find it. In this post we try to explain what we’ve learned in a much more accessible way.
Medicare Advantage Basics
Medicare Advantage is the private insurance alternative to traditional Medicare (TM), comprised largely of HMO and PPO options. One-third of the 60+ million Americans covered by Medicare are enrolled in MA plans. These plans, subsidized by the government, are governed by Medicare rules, but, within certain limits, are able to set their own premiums, deductibles, and service payment schedules each year.
Critically, they also determine their own network extent, choosing which physicians are in- or out-of-network. Apart from cost sharing or deductibles, the cost of care from providers that are in-network is covered by the plan. However, if an enrollee seeks care from a provider who is outside of their plan’s network, what the cost is and who bears it is much more complex.
Provider Types
To understand the MA (and enrollee) payment-to-provider pipeline, we first need to understand the types of providers that exist within the Medicare system.
Participating providers, which constitute about 97% of all physicians in the U.S., accept Medicare Fee-For-Service (FFS) rates for full payment of their services. These are the rates paid by TM. These doctors are subject to the fee schedules and regulations established by Medicare and MA plans.
Non-participating providers(about 2% of practicing physicians) can accept FFS Medicare rates for full payment if they wish (a.k.a., “take assignment”), but they generally don’t do so. When they don’t take assignment on a particular case, these providers are not limited to charging FFS rates.
Opt-out providersdon’t accept Medicare FFS payment under any circumstances. These providers, constituting only 1% of practicing physicians, can set their own charges for services and require payment directly from the patient. (Many psychiatrists fall into this category: they make up 42% of all opt-out providers. This is particularly concerning in light of studies suggesting increased rates of anxiety and depression among adults as a result of the COVID-19 pandemic).
How Out-of-Network Doctors are Paid
So, if an MA beneficiary goes to see an out-of-network doctor, by whom does the doctor get paid and how much? At the most basic level, when a Medicare Advantage HMO member willingly seeks care from an out-of-network provider, the member assumes full liability for payment.That is, neither the HMO plan nor TM will pay for services when an MA member goes out-of-network.
The price that the provider can charge for these services, though, varies, and must be disclosed to the patient before any services are administered. If the provider is participating with Medicare (in the sense defined above), they charge the patient no more than the standard Medicare FFS rate for their services. Non-participating providers that do not take assignment on the claim are limited to charging the beneficiary 115% of the Medicare FFS amount, the “limiting charge.” (Some states further restrict this. In New York State, for instance, the maximum is 105% of Medicare FFS payment.) In these cases, the provider charges the patient directly, and they are responsible for the entire amount (See Figure 1.)
Alternatively, if the provider has opted-out of Medicare, there are no limits to what they can charge for their services.The provider and patient enter into a private contract; the patient agrees to pay the full amount, out of pocket, for all services.
MA PPO plans operate slightly differently. By nature of the PPO plan, there are built-in benefits covering visits to out-of-network physicians (usually at the expense of higher annual deductibles and co-insurance compared to HMO plans). Like with HMO enrollees, an out-of-network Medicare-participating physician will charge the PPO enrollee no more than the standard FFS rate for their services. The PPO plan will then reimburse the enrollee 100% of this rate, less coinsurance. (SeeFigure 2.)
In contrast, a non-participating physician that does not take assignment is limited to charging a PPO enrollee 115% of the Medicare FFS amount, which can be further limited by state regulations. In this case, the PPO enrollee is also reimbursed by their plan up to 100% (less coinsurance) of the FFS amount for their visit. Again, opt-out physicians are exempt from these regulations and must enter private contracts with patients.
Figure 2: MA PPO Out-of-Network Payments
Some Caveats
There are two major caveats to these payment schemes (with many more nuanced and less-frequent exceptions detailed here). First, if a beneficiary seeks urgent or emergent care (as defined by Medicare) and the provider happens to be out-of-network for the MA plan (regardless of HMO/PPO status), the plan must cover the services at their established in-network emergency services rates.
The second caveat is in regard to the declared public health emergency due to COVID-19 (set to expire in April 2021, but likely to be extended). MA plans are currently required to cover all out-of-network services from providers that contract with Medicare (i.e., all but opt-out providers) and charge beneficiaries no more than the plan-established in-network rates for these services. This is being mandated by CMS to compensate for practice closures and other difficulties of finding in-network care as a result of the pandemic.
Conclusion
Outside of the pandemic and emergency situations, knowing how much you’ll need to pay for out-of-network services as a MA enrollee depends on a multitude of factors. Though the vast majority of American physicians contract with Medicare, the intersection of insurer-engineered physician networks and the complex MA payment system could lead to significant unexpected costs to the patient.
Fewer than four in every 10 American adults can afford a $1,000 surprise medical bill, according to survey results released Jan. 11 by finance company Bankrate.
Bankrate surveyed 1,003 Americans about their personal finances from Dec. 8 to 13, finding a 2 percent drop from the previous year in respondents who said they could comfortably cover a $1,000 expense. The study noted that credit card finance charges can often add up to hundreds of additional dollars when surprise expenses are not paid quickly.
However, some Americans have an optimistic outlook on their financial situation going forward, with 44 percent of respondents believing their personal finances will improve in 2021.
Surprise medical bills have become a major issue for Americans, but federal legislation to protect consumers continues to stall. Is Congress getting closer to halting this practice?
Listen to the full episode below, read the transcript or scroll down for more information.
Surprise bills can occur when patients with insurance unknowingly receive care from an out-of-network provider while at an in-network facility (such as a bill from an anesthesiologist for a scheduled surgery).
That provider is not bound by a set rate negotiated with an insurer and may charge more for a service than the insurer is willing to pay, and patients can end up on the hook for the difference.
It is difficult to capture the full extent of the problem, but research shows that surprise bills, also called balance bills, occur often, and have only been increasing in frequency and size over the past few years.
42% of hospital and ER visits may come with an unexpected charge
$2,000 average size of a surprise bill for a hospital visit
66% of Americans fear surprise bills
80% of Americans support surprise bill protections
The Source: Who’s To Blame?
Physicians
Hospitals employ some physicians directly, but many also contract with speciality physician groups of surgical assistants, anesthesiologists, radiologists, emergency medicine doctors and pathologists who may not be in the same insurance networks as the hospital. This is why most surprise bills occur. Research shows that private equity firms also play an important role, buying up speciality physician groups and using surprise billing as a core part of their business model.
Insurers
Insurers often take a lot of heat for the price of health care, but they play a more limited role in surprise billing. They can create narrow networks that leave hospitals or doctors out and open the door to balance billing. Insurers also do a poor job of maintaining accurate in-network provider directories, which means patients may think they’re choosing an in-network doctor when they are not.
Hospitals
While surprise bills from hospitals are less common than from physicians, they do occur when, for instance, a hospital is not in a patient’s network, but the patient is rushed there because of an emergency.
Ambulances
Air and ground ambulances rides are another source of surprise bills. One analysis showed that air ambulances resulted in median potential surprise bills of almost $21,700.
The Fixes: The Legislation Landscape
Federal Proposals
Over the past two years, Congress has considered at least four bipartisan bills to protect patients from surprise charges, but all four have stalled. The proposals offer different approaches to determine how much insurers will pay out-of-network providers. These bills typically address the problem by adopting a payment standard,arbitration process or a hybrid of the two.
Payment Standard
Insurers reimburse providers for out-of-network bills based on a set amount. Most bills propose using established in-network rates.
Arbitration
This process requires an insurer and provider to submit payment offers to a neutral party who makes the final call.
Hybrid
This approach combines the payment standard with arbitration to resolve disputes. An insurer pays a set amount, and if the provider disagrees, it can initiate arbitration.
State Laws
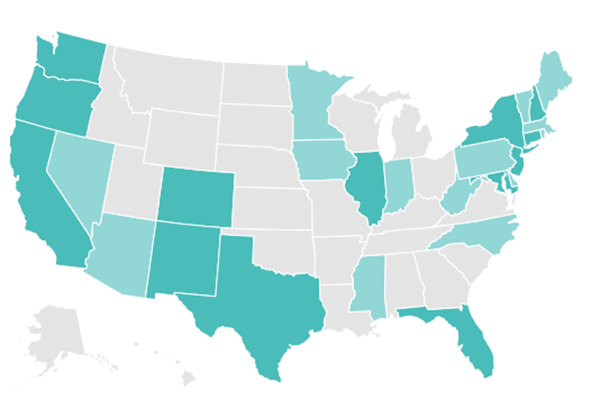
With federal solutions at a standstill, 30 states have passed varying levels of protections from surprise billing. As of July, 2020, 16 states have more comprehensive protections, which ensure that insured patients are only responsible for paying in-network costs, even when receiving care from out-of-network providers or emergency services at an out-of-network facility. Georgia was the latest state to pass such a law in July 2020. The other 14 states offer far more limited protections.
But even states with comprehensive protections cannot protect all patients from surprise medical bills. States are not able to regulate job-based coverage that falls under a federal law known as the Employee Retirement Income Security Act, which applies to most employer sponsored insurance. These patients remain vulnerable to surprise medical bills until Congress takes action to ban the practice.
Click on the map below for an interactive map from the Commonwealth Fund that details each state’s protections.
The Sticking Point: Will Congress Pass Protections?
Despite strong bipartisan support for protecting patients from surprise bills, disagreement comes over how much physician groups should charge and how much insurers should pay. Essentially, resolving this issue may mean Congress has to pick sides.
As a result, stakeholders such as hospitals and private equity-backed physician groups, in particular, have pushed back on federal legislation, arguing that banning surprise billing will cripple their bottom line. These equity-backed physician groups have powerful lobbying groups, and in 2019, spent at least $5 million to persuade lawmakers to halt the legislation.
The pandemic has increased the risk that patients will unknowingly receive care from an out-of-network provider or at an out-of-network facility. The Trump administration tried to limit surprise bills for those in need of COVID-19 treatment by banning hospitals and providers that receive money from its Provider Relief Fund from sending balance bills to patients. But this approach leaves significant gaps and has had mixed success.