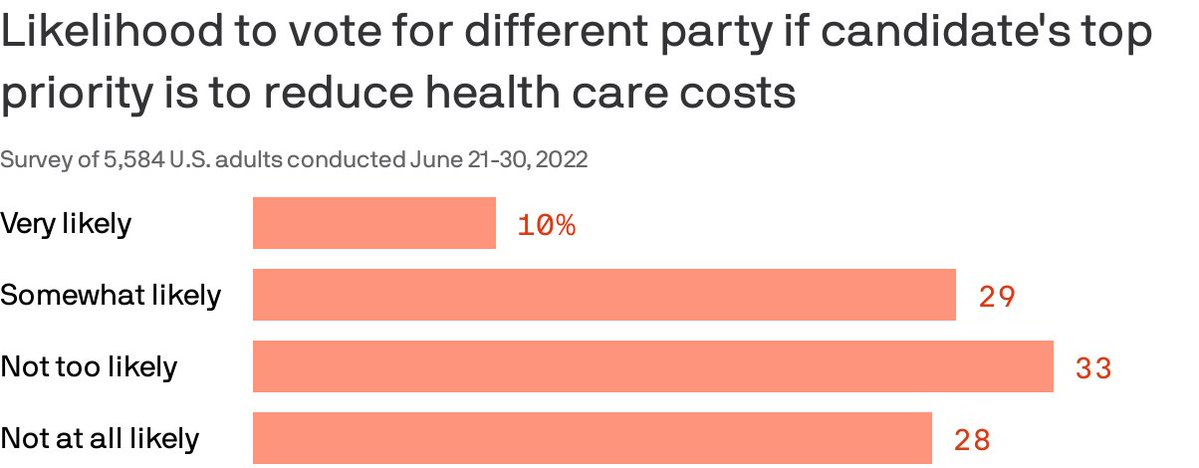
Almost 40% of Americans are willing to split their ticket and vote for a candidate from the opposing party who made a top priority of lowering health costs, according to a Gallup/West Health poll published Thursday.
Why it matters: Though candidates haven’t been talking much about medical costs in the run-up to the midterms, the issue remains enough of a priority that it could erode straight party-line voting.
By the numbers: 87% of Americans polled said a candidate’s plan to reduce the cost of health care services was very or somewhat important in casting a vote.
The issue cut across partisan lines, with 96% of Democrats and 77% of Republican respondents saying a candidate with a health care costs plan was an important factor.
86% also said a plan to lower prescription drug prices is very or somewhat important. That’s especially true for seniors.
Of note: Democratic voters were more likely than Republicans to say they would cross party lines because health costs are a top priority. Four in 10 Democrats said they were likely to do so compared to about 1 in 5 Republicans.
Before 2011, Medicare Advantage health plans absorbed a greater share of Medicare enrollment because traditional Medicare enrollees were transitioning to Medicare Advantage plans. From 2011 to 2019, Medicare Advantage enrollment continued to increase but the source changed.
The researchers used the Master Beneficiary Summary File from 2011 to 2019 to inform their study of the source of Medicare Advantage enrollment during that timeframe. These files provided over 524.4 million person-years.
Medicare Advantage still drew enrollees from traditional Medicare from 2012 to 2019, with the share of those who came from Medicare Advantage growing from 65.9 percent to 71.1 percent.
The number of enrollees that were new to Medicare who chose Medicare Advantage coverage also grew. A little over 18 percent of enrollees who did not have Medicare coverage previously transitioned into Medicare Advantage in 2012. But by 2019, that share had swelled to 24.7 percent.
Beneficiaries who switched to Medicare Advantage from traditional Medicare tended to be older. Fewer of them identified as Hispanic individuals but more of them identified as Black individuals. Additionally, they were more likely to be dually eligible and more likely to have a disability. Finally, they were more likely to die within two years of enrolling in Medicare Advantage.
“Our study is limited in that it was not designed to examine these mechanisms,” the researchers acknowledged. “As MA continues to grow, understanding the reasons for switching from TM to MA will become more important.”
Although the study did not explicitly explore the causes behind these enrollment shifts, the researchers cited three factors that might contribute to the growth and diversity of the Medicare Advantage population.
First, they noted that Medicare Advantage plans offer supplemental benefits and dental and vision coverage, which traditional Medicare does not cover.
In 2022, more Medicare Advantage plans offered more supplemental benefits, including special supplemental benefits for the chronically ill (SSBCI), expanded supplemental benefits, and traditional supplemental benefits, according to a Better Medicare Alliance brief.
Second, Medicare Advantage plans offer lower out-of-pocket healthcare spending compared to traditional Medicare.
Finally, Medicare Advantage might be more attractive due to the lower premiums.
In 2022, costs were particularly low since Medicare Advantage premiums dropped to the lowest level in 15 years, 10 percent lower than in 2021, the Better Medicare Alliance report shared.
The results corroborate separate studies that show that the Medicare Advantage population is growing and becoming more diverse.
In more than 100 congressional districts, Medicare Advantage coverage represents half or more of enrollment, according to Better Medicare Alliance research. Medicare Advantage coverage is particularly strong in Alabama, Michigan, and Florida.
Medicare Advantage plans grew 60 percent from 2013 to 2020. By 2020, Medicare Advantage plans served 25 million seniors, of which six out of ten were women. Also, more than half of all Hispanic American seniors (52 percent), 49 percent of African American seniors, and 35 percent of Asian Americans selected Medicare Advantage plans for their coverage.
The Biden Administration has released final surprise billing rules implementing the No Surprises Act, a federal law enacted in January 2021 that protects patients from out-of-network medical bills when they seek care at in-network facilities.
The new surprise billing rules detail the process for payers and providers to settle on payment for those out-of-network services. Previously, payers and providers would submit payment rates to an independent arbiter, selected by the government. The arbiter would choose the rate closest to the area’s median in-network payment for the services, otherwise known as the qualifying payment amount (QPA), while considering other factors, such as provider training and experience, the provider’s market share, and how difficult it was to provide the service, after the fact.
Provider groups have criticized the use of the QPA as the primary factor in an arbiter’s decision, arguing that the added weight to the QPA amount favors payers over providers.
Notably, the Texas Medical Association challenged the surprise billing arbitration process over the QPA issue and won. A district court vacated the requirement that arbiters select payment offers closest to the QPA unless the additional information warrants a closer review.
The American Hospital Association (AHA) and the American Medical Association (AMA) have also filed a lawsuit challenging the interim final rule implementing the dispute process, arguing that lawmakers did not intend for rules implementing the No Surprises Act to place that much emphasis on the QPA. The lawsuit is ongoing.
In light of the district court’s decision, the latest final surprise billing rules roll back the “rebuttable presumption” that favors the QPA. The rules state that arbiters are to consider the QPA “and then must consider all additional information submitted by a party to determine which offer best reflects the appropriate out-of-network rate.”
The final rules specify that arbiters “should select the offer that best represents the value of the item or service under dispute after considering the QPA and all permissible information submitted by the parties.”
The final rules also cover situations where payers have “downcoded” a claim. According to previous rulemaking, downcoding occurs when payers change service codes or change, add, or remove a modifier, which can lower the QPA for the service code or modifier billed by a provider.
The rules will create new requirements related to what information payers must share with providers when downcoding occurs. The information includes a statement that the service code or modifier was downcoded, an explanation of why the claim was downcoded, and the amount that would have been the QPA had the service code or modifier not been downcoded.
The Biden Administration—through the Departments of Labor, Health and Human Services, and Treasury, which officially released the final surprise billing rules—said that the rules “will help providers, facilities and air ambulance providers engage in more meaningful open negotiations with plans and issuers and will help inform the offers they submit to certified independent entities to resolve claim disputes.”
But whether the updated language is enough to tip the balance for providers remains to be seen. AHA said in a news release late last week that it is closely reviewing the final surprise billing rules.