Even as surgery and office visit volume rebounds, hospitals across the country continue to report that emergency department volume remains persistently depressed, down 10 to 20 percent compared to before the pandemic. The shift is even more drastic in pediatrics, with some pediatric hospitals and programs reporting that emergency care volume is seeing double the rate of decline.
Pediatric volume has been hit with a “double whammy”: with many schools and day cares still closed, contagious illnesses have plummeted. Fewer kids in youth sports means fewer injuries. And unlike adult hospitals, pediatric facilities haven’t filled their beds with COVID patients.“Of all our services, pediatric hospitalists have taken the greatest hit,” one children’s hospital physician leader shared. “Their service is usually full this time of the year with flu and RSV [respiratory syncytial virus]. But with kids not interacting with each other, general pediatric admissions have cratered.” Empty EDs have led some pediatric hospitals to shutter adjacent urgent care clinics: “It doesn’t make sense to operate an empty ED and an empty after-hours clinic”.
For patients, however, this can bring unexpected financial consequences, as they’ll now get an ED bill for services they would formerly have received in urgent care. But while pediatric hospitals have taken a greater volume hit, they’re also likely to see a faster rebound. Once kids are back to school and sports, the usual illnesses and injuries will likely return, and we’d guess parents won’t hesitate to seek care.
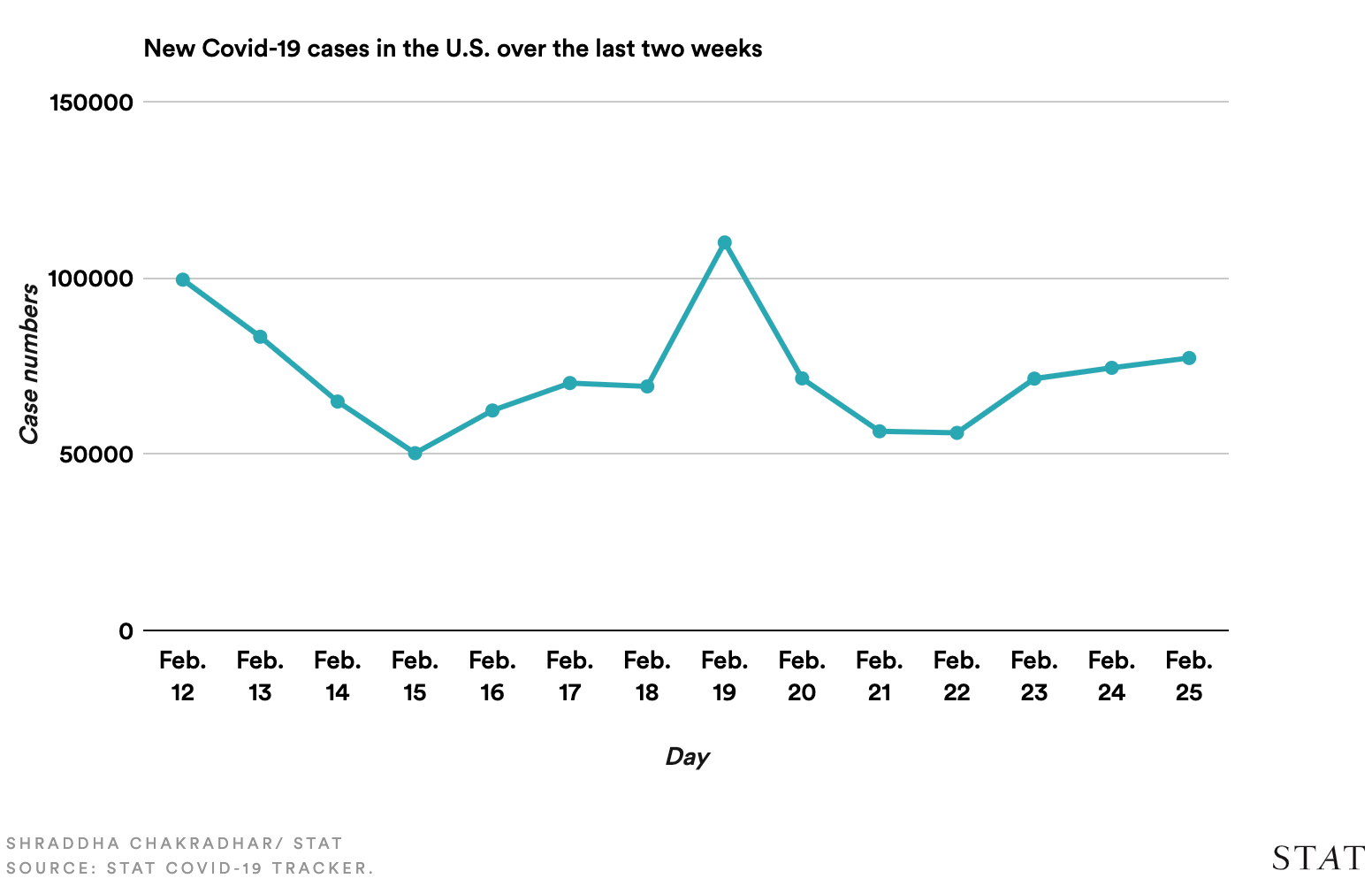
Although the nation reached a grim and long-dreaded milestone on Monday, surpassing 500,000 lives lost to COVID—more than were killed in two World Wars and the Vietnam conflict combined—the news this week was mostly good, as key indicators of the pandemic’s severity continued to rapidly improve.
Over the past two weeks, hospitalizations for COVID were down 30 percent, deaths were down 22 percent, and new cases declined by 32 percent—the lowest levels since late October. This week’s numbers declined somewhat more slowly than last week’s, leading Dr. Rachel Walensky, director of the Centers for Disease Control and Prevention, to caution people against letting their guard down just yet: “Things are tenuous. Now is not the time to relax restrictions.” Of particular concern are new variants of the coronavirus that have emerged in numerous states, including one in New York and another in California, that may be more contagious than the original virus.
The best news of the week was surely a report from the Food and Drug Administration (FDA) evaluating the new, single-shot COVID vaccine from Johnson & Johnson (J&J), showing it to be highly effective at preventing severe disease, hospitalization, and death caused by COVID, including variants. On Friday, a panel of outside experts met to assess whether to approve the J&J vaccine for emergency use, which would make it the third in the nation’s arsenal of COVID vaccines. If approved, the vaccine will be rolled out next week, according to the White House, with up to 4M doses available immediately.
The sooner the better: new data show that since vaccinations began in late December, new cases among nursing home residents have fallen more than 80 percent—a hopeful glimpse at the future that lies ahead for the general population once vaccines become widely available.
Scientists at the Food and Drug Administration said Wednesday that the single-shot Covid-19 vaccine developed by Johnson & Johnson is effective and prevents hospitalizations from the disease.
Johnson & Johnson also revealed new, encouraging data showing the vaccine may do a better-than-expected job at protecting patients against new variants of the virus that causes disease. At the same time, FDA experts said the company’s study, results of which were originally made public in a Jan. 29 press release, includes insufficient information to draw conclusions on efficacy in people older than 75.
Documents from the FDA scientists, as well as separate documents from Johnson & Johnson, were released ahead of a Friday meeting of an FDA advisory panel in which outside experts will discuss and then vote on the risks and benefits of the new vaccine. The panel, known as the Vaccines and Related Biological Products Advisory Committee, makes recommendations to the FDA; the agency is not required to follow them, but it generally does.
The J&J vaccine is the first vaccine to show efficacy given as a single dose. It also does not need to be kept frozen when being shipped, as the vaccines developed by Moderna and the team of Pfizer and BioNTech do. Both of those advantages could be profound when it comes to vaccinating as many people as possible, a key step in slowing the spread of SARS-CoV-2.
Overall in the study, the vaccine reduced cases of Covid-19 that were rated as moderate to severe by 66.1% when considering cases occurring at least 28 days after vaccination. There were 193 cases that occurred at least 28 days after vaccination in the placebo group and 66 in the vaccine group. As of Feb. 5, there were seven Covid-19 related deaths in the placebo group and none in the vaccine group.
FDA researchers conducted a new analysis of how frequently volunteers in the study were hospitalized for Covid. When researchers counted cases 28 days after vaccination, there were zero hospitalizations in the vaccine arm and 16 in the placebo arm. For the full analysis set starting with the first dose, there were six hospitalizations for those who received the vaccine and 42 for those who did not.
Johnson & Johnson and the National Institutes of Health initially announced interim results of a 44,325 study testing the vaccine’s efficacy on Jan. 29. At the time, they said the 66% efficacy varied by geography. The vaccine was 72% protective in the U.S., compared to 58% in South Africa, where a new variant of SARS-CoV-2 is circulating.
In new documents, Johnson & Johnson said that in South Africa, the vaccine reduced severe or critical Covid-19 by 81.7% starting 28 days after vaccination, but that efficacy against more moderate disease was 64%. But the company said that the vaccine efficacy was not affected by the high prevalence of another variant in Brazil.
Unexpected side effects occurred at the same rate overall among volunteers who received vaccine and placebo — about 0.5%. However, some rare conditions appeared more common with the vaccine. Blood clot-related conditions occurred in 15 volunteers who received the vaccine and 10 who received placebo. Tinnitus, a ringing in the ears, occurred in six volunteers who received the vaccine and none who received placebo. The FDA said it will recommend monitoring for thromboembolic events after an EUA is granted.
Expected side effects that are related to the vaccine’s effect were common. Nearly half of volunteers reported injection site pain, 38.9% reported headache, 38.2% fatigue, and 33% reported muscle aches.
Johnson & Johnson also conducted an analysis in 2,650 volunteers looking at whether those who received the vaccine were less likely to test positive for the SARS-CoV-2 virus, which causes Covid-19, without having symptoms. There were 50 such cases in the placebo group compared to 18 among those who received the vaccine, a 65.5% reduction.
The United States has purchased 100 million doses of the vaccine, with an option to buy another 200 million doses. The agreement, announced last August, netted J&J over $1 billion in a contract with the Biomedical Advanced Research and Development Authority and the Department of Defense.
That said, the company currently has a limited number of doses to contribute to the effort to step up the country’s vaccine rollout. It will be April before J&J begins to have substantial amounts of vaccine to feed into the distribution pipeline, Moncef Slaoui, former co-chair of Operation Warp Speed, said earlier this year.
However, the company and the NIH said the vaccine was 85% effective at preventing severe disease, with no differences seen across the eight countries included in the study.
J&J is also conducting a trial in the United States of a two-dose vaccine, with the doses given eight weeks apart.The results from that 30,000 person trial are not expected until sometime in May.
The FDA documents represent the first close look at the data released Jan. 29, and are the result of a three-week effort by FDA scientists to independently evaluate the data generated in the trial. Friday’s panel will provide a deeper look at what those data actually mean.
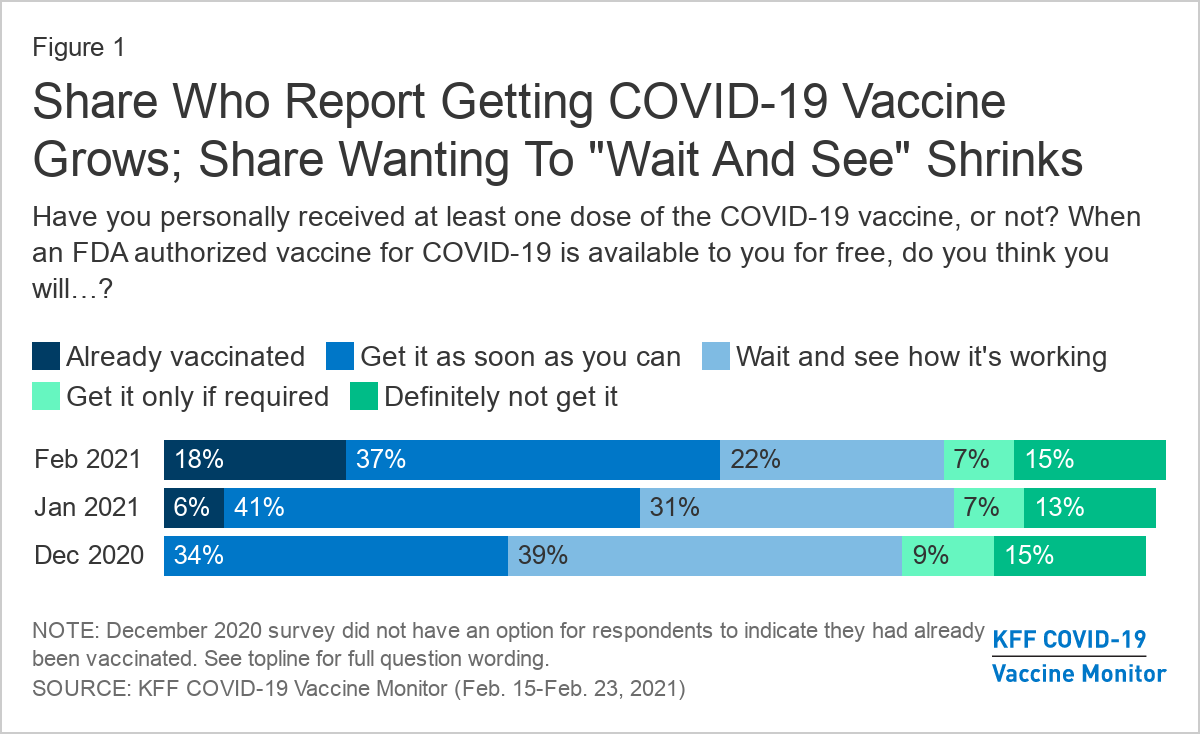
More than half of adults in the U.S. (55%) say they’ve already gotten one dose of Covid-19 vaccine or they’re eager to get one as soon as they can, an increase in acceptance from January (47%), a new poll reports. About 1 in 5 people are waiting to see how the vaccine rollout goes, but don’t rule out vaccination. Another 1 in 5 people are more reluctant: 7% would get vaccinated only if required by work, school, or some other activity, and 15% say no to vaccine under any circumstance. The increase in eagerness spans all demographic groups, but Black adults and young adults under age 30 were most likely to say they want to wait and see.
Dr. Christine Choi, 32, a medical resident at Harbor-UCLA Medical Center in Torrance, prepares to enter an isolation area for COVID-19 inpatients. Health care providers must face daily patient death and suffering.
Soon after the COVID-19 pandemic began last spring, Christine Choi, DO, a second-year medical resident at Harbor-UCLA Medical Center, volunteered to enter COVID-19 patient rooms. Since then, she has worked countless nights in the intensive care unit in full protective gear, often tasked with giving the sickest patients and their families the grim choice between intubation or near-certain death.
“I’m offering this guy two terrible options, and that’s how I feel about work: I can’t fix this for you and it sucks, and I’m sorry that the choices I’m giving you are both terrible,” Choi told the Los Angeles Times’ Soumya Karlamangla about one patient encounter.
While Choi exhibits an “almost startlingly positive attitude” in her work, it’s no match for the psychological burdens placed on her shoulders by the global pandemic, Karlamangla wrote. When an older female COVID-19 patient died in the hospital recently, her husband — in the same hospital with the same diagnosis — soon began struggling to breathe. Sensing that he had little time left, Choi held a mobile phone at his bedside so that each of his children could come on screen to tell him they loved him. “I was just bawling in my [personal protective equipment],” Choi said. “The sound of the family members crying — I probably will never forget that,” she said.
It was not the first time the young doctor helped family members say goodbye to a loved one, and it would not be the last. Health care providers like Choi have had to work through unimaginable tragedies and unprecedented circumstances because of COVID-19, with little time to dedicate to their own mental health or well-being.
It has been nearly a year since the US reported what was believed at the time to be its first coronavirus death in Washington State. Since then, the pandemic death toll has mushroomed to nearly 500,000 nationwide, including 49,000 Californians. These numbers are shocking, and yet they do not capture the immeasurable emotional weight that falls on the health care providers with the most intimate view of COVID-19’s deadly progression.“The horror of the pandemic has unfolded largely outside public view and inside hospitals, piling a disproportionate share of the trauma on the people whose work takes them inside their walls,” Karlamangla wrote.
Experts are deeply concerned about the psychological and physical burdens that providers must bear, and the fact that there is still no end in sight. “At least with a natural disaster, it happens, people get scattered all over the place, property gets damaged or flooded, but then we begin to rebuild,” Lawrence Palinkas, PhD, MA, a medical anthropologist at USC, told Karlamangla. “We’re not there yet, and we don’t know when that will actually occur.”
Sixty-eight percent of providers said they feel emotionally drained from their work, 59% feel burned out, 57% feel overworked, and 50% feel frustrated. The poll asked providers who say they feel burned out what contributes most to that viewpoint. One doctor from the Central Valley wrote:
“Short staffed due to people out with COVID. I’m seeing three times as many patients, with no time to chart or catch up. Little appreciation or contact from my bosses. I have never had an N95 [mask]. The emotional toll this pandemic is taking. Being sick myself and spreading it to my wife and young kids. Still not fully recovered but needing to be at work due to physician shortages. Lack of professional growth, and a sense of lack of appreciation at work and feeling overworked. The sadness of the COVID-related deaths and the stories that go along with the disease. That’s a lot of stuff to unpack.”
The pandemic has been especially challenging for female health providers, who compose 77% of health care workers with direct patient contact. “The pandemic exacerbated gender inequities in formal and informal work, and in the distribution of home responsibilities, and increased the risk of unemployment and domestic violence,” an international group of experts wrote in the Lancet. “While trying to fulfill their professional responsibilities, women had to meet their families’ needs, including childcare, home schooling, care for older people, and home care.”
For one female doctor from the Bay Area who responded to the CHCF survey, the extra burdens of the pandemic have been unrelenting: “Having to work more, lack of safe, affordable, available childcare while I’m working. As a single mother, working 15 hours straight, then having to care for my daughter when I get home. Just exhausted with no days off. So many Zoom meetings all day long. Miss my family and friends.”
It is unclear how the pandemic will affect the health care workforce in the long term. For now, the damage “can be measured in part by a surge of early retirements and the desperation of community hospitals struggling to hire enough workers to keep their emergency rooms running,” Andrew Jacobs reported in the New York Times.
One of the early retirements Jacobs cited was Sheetal Khedkar Rao, MD, a 42-year-old internist in suburban Chicago. Last October, she decided to stop practicing medicineafter “the emotional burden and moral injury became too much to bear,” she said. Two of the main factors driving her decision were a 30% pay cut to compensate for the decline in revenue from primary care visits and the need to spend more time at home after her two preteen children switched to remote learning.
“Everyone says doctors are heroes and they put us on a pedestal, but we also have kids and aging parents to worry about,” Rao said.
Working Through Unremitting Sickness and Death
In addition to the psychological burden, health care providers must cope with a harsh physical toll. People of color account for most COVID-19 cases and deaths among health care workers, according to a KFF issue brief. Some studies show that health care workers of color “are more likely to report reuse of or inadequate access to [personal protective equipment] and to work in clinical settings with greater exposure to patients with COVID-19.”
“Lost on the Frontline,” a collaboration of Kaiser Health News and the Guardian, has counted more than 3,400 deaths among US health care workers from COVID-19. Eighty-six percent of the workers who died were under age 60, and nurses accounted for roughly one-third of the deaths.
“Lost on the Frontline” provides the most comprehensive picture available of health care worker deaths, because the US still lacks a uniform system to collect COVID-19 morbidity and mortality data among health care workers. A year into the project, the federal government has decided to take action. Officials at the US Department of Health and Human Services cited the project when asking the National Academies of Sciences, Engineering, and Medicine for a rapid expert consultation to understand the causes of deaths among health care workers during the pandemic.
The National Academies’ report, published December 10, recommends the “adoption and use of a uniform national framework for collecting, recording, and reporting mortality and morbidity data” along with the development of national reporting standards for a core set of morbidity impacts, including mental well-being and psychological effects related to working through public health crises. Some health care experts said the data gathering could be modeled on the federal government’s World Trade Center Health Program, which provides no-cost medical monitoring and treatment for workers who responded to the 9/11 terrorist attacks 20 years ago.
“We have a great obligation to people who put their lives on the line for the nation,” Victor J. Dzau, MD, president of the National Academy of Medicine, told Jacobs.
As COVID-19 cases surged last fall, non-COVID-19 hospital admissions fell substantially, particularly in the Midwest and West, according to a new analysis by the Kaiser Family Foundation of 2020 inpatient admission data from electronic medical records through Dec. 5.
The analysis also highlights admission trends by age and sex, and found that patients 65 and over — those most at risk of complications from the novel coronavirus — delayed care at greater rates than those under 65 again in the fall. Still, the discrepancy between visits based on age was more pronounced in the spring.
On average, males and females had almost identical admission patterns throughout the entire year. Though looking at the raw numbers, women’s total admissions trended above their male counterparts, which researchers attributed to childbirth.
Dive Insight:
The latest analysis from the think tank provides a fuller picture of how the COVID-19 pandemic influenced admission trends throughout 2020.
Overall, total admissions bottomed out in April and March but have remained near normal, or above 90% of expected admissions since June, according to electronic medical record data from the Epic Health Research Network, which pools information from 20 million patients across 97 hospitals in the U.S.
However, while total admissions — which includes those sick with COVID-19 — remained near normal, the pattern differed when zeroing in on non-COVID-19 admissions, or those admitted who did not have the virus.
Non-COVID-19 admissions started to fall againin November and by Dec. 5 they fell to 80% of expected volume, which is likely to put financial pressure on hospitals, particularly those with smaller reserves of cash on hand, Kaiser noted.
The decline was steepest in the Midwest and West, dropping to about 76% of expected volume between early November and December.
Researchers fear the drop in non-COVD-19 admissions may have long-term consequences.
“The levels of non-COVID-19 admissions seen in the fall of 2020 suggest that people may be delaying care in ways that could be harmful to their long-term health,” according to the study.
Insurers observed similar patterns of depressed volume in the fourth quarter.
Humana, which largely covers seniors in Medicare plans, noted non-COVID-19 volume dropped the last two months of the quarter after previously returning to near normal. It led Humana to report a loss in the fourth quarter as COVID-19 testing and treatment accelerated. Centene, which reported a Q4 loss, echoed a similar pattern.