America’s coronavirus outbreak has surpassed Europe’s.
Why it matters: It wasn’t long ago that public health experts were pointing to Europe as a warning sign for the U.S. But the U.S. now has a higher per capita caseload than the EU ever has during its recent surge.
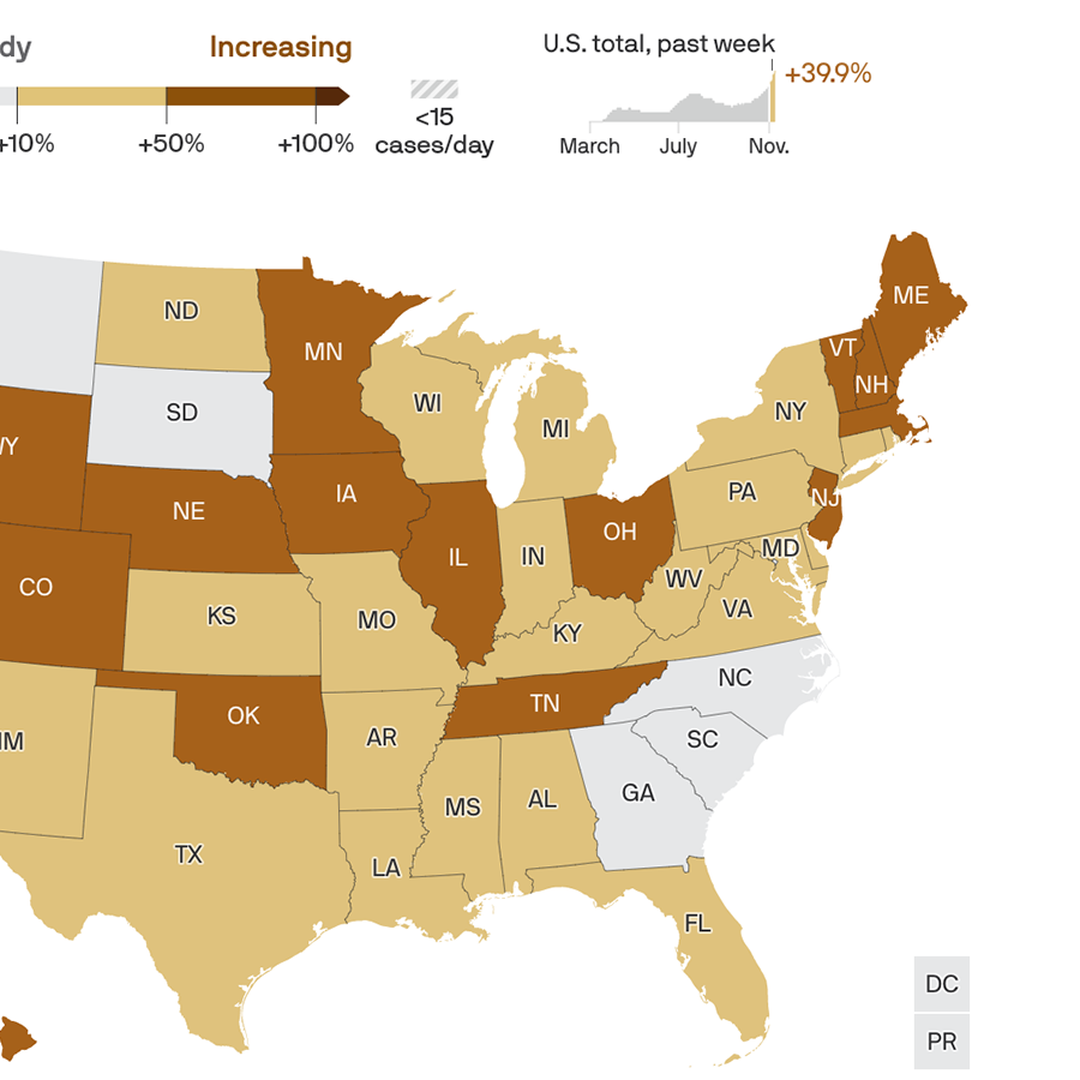
By the numbers: As of Saturday, 15 states had higher per capita caseloads, averaged over seven days, than the European country with the highest caseload — Luxembourg.
The U.S. overall saw 52.4 cases per 100,000 people. The EU saw 37.6 per 100,000 on Saturday, and peaked at 46.7 cases per 100,000 on Nov. 8.
The big picture: Europe’s steady rise in coronavirus cases over the last couple of months prompted many countries to bring back lockdowns or other strict behavioral restrictions.
Meanwhile, in the U.S., some of the hardest-hit states — like Iowa — are just now adopting mask mandates, and airports over the weekend were packed with people traveling for Thanksgiving.
Yes, but: Cases in the hardest-hit states are starting to trend down, a sign that people are modifying their behavior on their own.
What we’re watching: There’s no sign that the number of U.S. cases nationally is going to stop rising anytime soon, especially in the absence of strong federal or state restrictions.
Hospitalizations and deaths lag behind cases by a few weeks. That means that Europe likely has easier days ahead, while America’s dark days are just getting started.
In the U.S., today’s overwhelmed hospitals will continue to keep getting hit with ever-growing caseloads for awhile.
Cleveland Clinic has about 1,000 employees away from work due to COVID-19, the health system told Becker’s Nov. 23.
The count includes 925 workers in Ohio and other workers across the health system, which also has locations in Florida and Las Vegas. It is an increase from about 800 Cleveland Clinic employees in Ohio reported sidelined as of Nov. 16.
Cleveland Clinic spokesperson Andrea Pacetti said the increase in the number of employees affected by COVID-19 reflects more spreading of the virus in the community and in Ohio, and most affected employees are contracting the virus in the community.
Due to a surge in cases, Cleveland Clinic has taken steps to ensure enough staffing to meet patients’ needs, said Ms. Pacetti. This includes shifting some employees to different areas of the health system to enable Cleveland Clinic to expand bed capacity for COVID-19 patients.
“We are also evaluating our surgical schedule weekly based on hospital occupancy and admissions of patients with COVID-19,” Ms. Pacetti said. “Our leadership meets every day and reviews our staffing to ensure we can provide the highest quality care to all our patients.”
Cleveland Clinic also urges the public to help reduce the spread of the virus so the health system can continue to care for COVID-19 patients and patients who need care but who don’t have the coronavirus.
“This isn’t just a Cleveland Clinic issue, but true for the whole state. We are asking the community to follow guidelines — wear masks, social distance and wash your hands — so we can keep our medical teams healthy,” Ms. Pacetti said.
Cleveland Clinic has about 50,000 employees in Ohio.
As record numbers of coronavirus cases overwhelm hospitals across the United States, there is something strikingly different from the surge that inundated cities in the spring: No one is clamoring for ventilators.
The sophisticated breathing machines, used to sustain the most critically ill patients, are far more plentiful than they were eight months ago, when New York, New Jersey and other hard-hit states were desperate to obtain more of the devices, and hospitals were reviewing triage protocols for rationing care. Now, many hot spots face a different problem: They have enough ventilators, but not nearly enough respiratory therapists, pulmonologists and critical care doctors who have the training to operate the machines and provide round-the-clock care for patients who cannot breathe on their own.
Since the spring, American medical device makers have radically ramped up the country’s ventilator capacity by producing more than 200,000 critical care ventilators, with 155,000 of them going to the Strategic National Stockpile. At the same time, doctors have figured out other ways to deliver oxygen to some patients struggling to breathe — including using inexpensive sleep apnea machines or simple nasal cannulas that force air into the lungs through plastic tubes.
But with new cases approaching 200,000 per day and a flood of patients straining hospitals across the country, public health experts warn that the ample supply of available ventilators may not be enough to save many critically ill patients.
“We’re now at a dangerous precipice,” said Dr. Lewis Kaplan, president of the Society of Critical Care Medicine. Ventilators, he said, are exceptionally complex machines that require expertise and constant monitoring for the weeks or even months that patients are tethered to them. The explosion of cases in rural parts of Idaho, Ohio, South Dakota and other states has prompted local hospitals that lack such experts on staff to send patients to cities and regional medical centers, but those intensive care beds are quickly filling up.
Public health experts have long warned about a shortage of critical care doctors, known as intensivists, a specialty that generally requires an additional two years of medical training. There are 37,400 intensivists in the United States, according to the American Hospital Association, but nearly half of the country’s acute care hospitals do not have any on staff, and many of those hospitals are in rural areas increasingly overwhelmed by the coronavirus.
“We can’t manufacture doctors and nurses in the same way we can manufacture ventilators,” said Dr. Eric Toner, an emergency room doctor and senior scholar at the Johns Hopkins Center for Health Security. “And you can’t teach someone overnight the right settings and buttons to push on a ventilator for patients who have a disease they’ve never seen before. The most realistic thing we can do in the short run is to reduce the impact on hospitals, and that means wearing masks and avoiding crowded spaces so we can flatten the curve of new infections.”
Medical association message boards in states like Iowa, Oklahoma and North Dakota are awash in desperate calls for intensivists and respiratory therapists willing to temporarily relocate and help out. When New York City and hospitals in the Northeast issued a similar call for help this past spring, specialists from the South and the Midwest rushed there. But because cases are now surging nationwide, hospital officials say that most of their pleas for help are going unanswered.
Dr. Thomas E. Dobbs, the top health official in Mississippi, said that more than half the state’s 1,048 ventilators were still available, but that he was more concerned with having enough staff members to take care of the sickest patients.
“If we want to make sure that someone who’s hospitalized in the I.C.U. with the coronavirus has the best chance to get well, they need to have highly trained personnel, and that cannot be flexed up rapidly,” he said in a news briefing on Tuesday.
Dr. Matthew Trump, a critical care specialist at UnityPoint Health in Des Moines, said that the health chain’s 21 hospitals had an adequate supply of ventilators for now, but that out-of-state staff reinforcements might be unlikely to materialize as colleagues fall ill and the hospital’s I.C.U. beds reach capacity.
“People here are exhausted and burned out from the past few months,” he said. “I’m really concerned.”
The domestic boom in ventilator production has been a rare bright spot in the country’s pandemic response, which has been marred by shortages of personal protective equipment, haphazard testing efforts and President Trump’s mixed messaging on the importance of masks, social distancing and other measures that can dent the spread of new infections.
Although the White House has sought to take credit for the increase in new ventilators, medical device executives say the accelerated production was largely a market-driven response turbocharged by the national sense of crisis. Mr. Trump invoked the wartime Defense Production Act in late March, but federal health officials have relied on government contracts rather than their authority under the act to compel companies to increase the production of ventilators.
Scott Whitaker, president of AdvaMed, a trade association that represents many of the country’s ventilator manufacturers, said the grave situation had prompted a “historic mobilization” by the industry. “We’re confident that our companies are well positioned to mobilize as needed to meet demand,” he said in an email.
Public health officials in Minnesota, Mississippi, Utah and other states with some of the highest per capita rates of infection and hospitalization have said they are comfortable with the number of ventilators currently in their hospitals and their stockpiles.
Mr. Whitaker said AdvaMed’s member companies were making roughly 700 ventilators a week before the pandemic; by the summer, weekly output had reached 10,000. The juggernaut was in part fueled by unconventional partnerships between ventilator companies and auto giants like Ford and General Motors.
Chris Brooks, chief strategy officer at Ventec Life Systems, which collaborated with G.M. to fill a $490 million contract for the Department of Health and Human Services, said the shared sense of urgency enabled both companies to overcome a thicket of supply-chain and logistical challenges to produce 30,000 ventilators over four months at an idled car parts plant in Indiana. Before the pandemic, Ventec’s average monthly output was 100 to 200 machines.
“When you’re focused with one team and one mission, you get things done in hours that would otherwise take months,” he said. “You just find a way to push through any and all obstacles.”
Despite an overall increase in the number of ventilators, some researchers say many of the new machines may be inadequate for the current crisis. Dr. Richard Branson, an expert on mechanical ventilation at the University of Cincinnati College of Medicine and an author of a recent study in the journal Chest, said that half of the new devices acquired by the Strategic National Stockpile were not sophisticated enough for Covid-19 patients in severe respiratory distress. He also expressed concern about the long-term viability of machines that require frequent maintenance.
“These devices were not built to be stockpiled,” he said.
The Department of Health and Human Services, which has acknowledged the limitations of its newly acquired ventilators, said the stockpile — nine times as large as it was in March — was well suited for most respiratory pandemics. “These stockpiled devices can be used as a short-term, stopgap buffer when the immediate commercial supply is not sufficient or available,” the agency said in a statement.
Projecting how many people will end up requiring mechanical breathing assistance is an inexact science, and many early assumptions about how the coronavirus affects respiratory function have evolved.
During the chaotic days of March and April, emergency room doctors were quick to intubate patients with dangerously low oxygen levels. They subsequently discovered other ways to improve outcomes, including placing patients on their stomachs, a protocol known as proning that helps improve lung function. The doctors also learned to embrace the use of pressurized oxygen delivered through the nose, or via BiPAP and CPAP machines, portable devices that force oxygen into a patient’s airways.
Many health care providers initially hesitated to use such interventions for fear the pressurized air would aerosolize the virus and endanger health care workers. The risks, it turned out, could be mitigated through the use of respirator masks and other personal protective gear, said Dr. Greg Martin, the chief of pulmonary and critical care at Grady Health Systems in Atlanta.
“The familiarity of taking care of so many Covid patients, combined with good data, has just made everything we do 100 times easier,” he said.
Some of the earliest data about the perils of intubating coronavirus patients turned out to be incomplete and misleading. Dr. Susan Wilcox, a critical care specialist at Massachusetts General Hospital, said many providers were spooked by data that suggested an 80 percent mortality rate among ventilated coronavirus patients, but the actual death rate turned out to be much lower. The mortality rate at her hospital, she said, was about 25 to 30 percent.
“Some people were saying that we should intubate almost immediately because we were worried patients would crash and have untoward consequences if we waited,” she said. “But we’ve learned to just go back to the principles of good critical care.”
Survival rates have increased significantly at many hospitals, a shift brought about by the introduction of therapeutics like dexamethasone, a powerful steroid that Mr. Trump took when he was hospitalized with the coronavirus. The changing demographics of the pandemic — a growing proportion of younger patients with fewer health risks — have also played a role in the improving survival rates.
Dr. Nikhil Jagan, a critical care pulmonologist at CHI Health, a hospital chain that serves Iowa, Kansas and Nebraska, said many of the coronavirus patients who were arriving at his emergency room now were less sick than the patients he treated in the spring.
“There’s a lot more awareness about the symptoms of Covid-19,” he said. “The first go-around, when people came in, they were very sick right off the bat and in respiratory distress or at the point of respiratory failure and had to be intubated.”
But the promising new treatments and enhanced knowledge can go only so far should the current surge in cases continue unabated. The country passed 250,000 deaths from the coronavirus last week, a reminder that many critically ill patients do not survive. The daily death toll has been rising steadily and is approaching 2,000.
“Ventilators are important in critical care but they don’t save people’s lives,” said Dr. Branson of the University of Cincinnati. “They just keep people alive while the people caring for them can figure out what’s wrong and fix the problem. And at the moment, we just don’t have enough of those people.”
For now, he said there was only one way out the crisis: “It’s not that hard,” he said. “Wear a mask.”
As we navigate the greatest health crisis of our lifetimes, it turns out that many aspects of our experiences in 2020 aren’t as “unprecedented” as we may think. The widely varied pandemic responses by local and state officials (and resulting political polarization) occurring today also transpired over 100 years ago during the Spanish Flu.
Lessons from a century ago may be worth revisiting: the left side of the graphic above details the health and economic case for public health mitigation strategies.Cities that enacted “longer interventions” (including mask mandates, closures, business capacity restrictions, and social distancing measures) in 1918 experienced fewer deaths per capita, as well as higher employment gains through 1919, compared to “similar” cities that enacted “shorter interventions.” For example, Los Angeles, which declared a state of emergency and banned all public gatherings early in the pandemic, had 25 percent fewer deaths per capita, and a 27 percentage-point greater gain in subsequent employment than San Francisco, which mainly focused on urging residents to wear masks in public.
Fast forward to today, when we’re also seeing significant differences between COVID containment policies at the state level. The right side of the graphic shows thatstates with the weakest overall pandemic containment policies are currently experiencing the worst outbreaks, measured here by hospitalizations per capita. States like Hawaii and New York, which maintained many of the strict mitigation strategies first put into place in the spring, are seeing those restrictions pay off with fewer hospitalizations during the latest spike.
Conversely, Iowa and the Dakotas have fewer, and less stringent, public health measures, and are now seeing the highest surges in the country today. (New Mexico shows that state-level policy decisions don’t explain everything—it’s currently battling a serious outbreak despite maintaining some of the strongest containment measures over the course of the pandemic.)
As we head into the worst COVID wave so far, the debate over whether saving “lives” or “livelihoods” should dominate the pandemic response rages on.History shows that higher levels of public health intervention can both save lives and result in stronger economic recovery.
Sioux Falls, S.D.-based Sanford Health President and CEO Kelby Krabbenhoft shared his thoughts about having COVID-19 and why he won’t be wearing a mask in an email to health system staff, according to the Grand Forks Herald.
In the 1,000-word email sent Nov. 18, Mr. Krabbenhoft said he had COVID-19, but he’s now back in his office working without a mask. He said he won’t be wearing a mask because doing so would only be a “symbolic gesture.” He considers himself immune from the virus.
“The information, science, truth, advice and growing evidence is that I am immune for at least seven months and perhaps for years to come, similar to that of chicken pox, measles, etc. For me to wear a mask defies the efficacy and purpose of a mask and sends an untruthful message that I am susceptible to infection or could transmit it,” Mr. Krabbenhoft wrote. “I have no interest in using masks as a symbolic gesture when I consider that my actions in support of our family leave zero doubt to my support of all 50,000 of you. My team and I have a duty to express the truth and facts and reality and not feed the opposite.”
The CDC says those who have had COVID-19 should take steps to reduce the risk of spreading the virus, including wearing a mask in public places and staying at least 6 feet away from other people.
In his email, Mr. Krabbenhoft argues the “on-again, off-again” use of masks is absurd. “Masks have been a symbolic issue that frankly frustrates me,” he wrote.
“On the other hand, for people who have not contracted the virus and may acquire it and then spread it … it is important for them to know that masks are just plain smart to use and in their best interest,” Mr. Krabbenhoft wrote.
The health system CEO concluded his letter by sharing his optimism for the future, noting that some Sanford Health workers would be among the first to get a COVID-19 vaccine once it is available.
Sanford Health didn’t respond to Becker’s Hospital Review‘s request for comment by deadline.
Read the Grand Forks Herald article here, which includes full text of the email Mr. Krabbenhoft sent to employees.
At least 250,000 people in the United States have died of covid-19, the disease caused by the coronavirus, since February, and many public health officials warn the pandemic is just entering its deadliest phase. Yet, as the country confronts this horrifying death toll, there is little understanding of what a loss of this size represents.
Here is some historical perspective about losing a quarter of a million people, looking at major events in our past that have cost American lives.
More than 58,000 Americans were killed during the decade-plus of involvement in the Vietnam War. So the pandemic’s fatalities represent four Vietnam Wars since February.
During the Korean War, nearly 37,000 Americans were lost; covid-19 has claimed nearly seven times more.
During World War II, the country mourned 405,000 members of the “Greatest Generation.” The pandemic has taken nearly two-thirds as many people, a lot of them old enough to remember the fight against the Nazis and the Japanese.
And World War I? 116,000 U.S. dead in two years of fighting. The pandemic has more than doubled that number in a fraction of the time.
What about our deadliest conflict, the Civil War? Death toll estimates range from 600,000 to 850,000. Even at the high end of that range, the pandemic has permanently taken nearly 30 percent as many family members from Thanksgiving tables.
On Sept. 11, 2001, almost 3,000 people were killed in terrorist attacks in New York, Washington and Shanksville, Pa.
The deadliest day of the pandemic so far — Sept. 18 — surpassed that, at 3,660 deaths. Wednesday, as the virus surged across the country, the daily death toll had risen again to 1,894. Public health officials fear that by the end of this month, the United States could lose more people per day from the pandemic than the 2,403 Americans killed inthe Japanese attack on Pearl Harbor on Dec. 7, 1941.
And how does this pandemic compare to others in U.S. history?
The Centers for Disease Control and Prevention keeps records on four of them. The 2009 H1N1 pandemic killed 12,469 Americans. The 1968 Influenza A pandemic killed about 100,000 people. And the 1957-1958 Influenza A pandemic took 116,000 U.S. lives.
One of the more conservative disease models currently projects the United States could reach 438,000 deaths, more than during World War II, by March 1, 2021.
No state in America could clear the threshold right now to safely allow indoor gatherings, Axios’ Sam Baker and Andrew Witherspoon report.
The big picture: This is bad as the pandemic has ever been — the most cases, the most explosive growth and the greatest strain on hospitals.
If businesses were closed right now, it would not be safe to reopen them. And holiday travel will be risky no matter where you’re coming from or where you’re going.
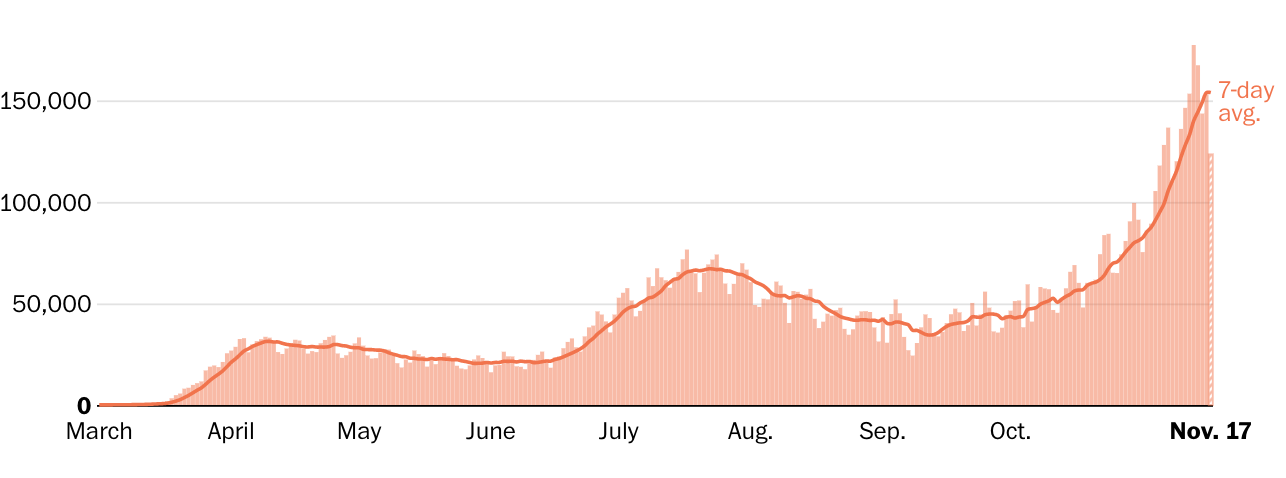
By the numbers: Over the past week, the U.S. averaged more than 154,000 new cases per day, the highest rate of the entire pandemic.
The number of new infections rose in 46 states, held steady in three, and declined in only one — Hawaii.
This week’s nationwide totals are a 30% increase over last week, which was a 40% increase over the week before that. Daily infections have been rising by at least 15% for the past six weeks.
Testing was up about 11% over the past week. The U.S. is now conducting about 1.5 million tests per day. That’s a lot, but cases clearly are still rising faster than testing.
Between the lines:Whatever metric you might use to decide whether it’s safe to have a large Thanksgiving get-together, or to sit inside a bar or restaurant, the answer is probably no.
Experts recently told The Atlantic that they wouldn’t feel comfortable attending an indoor dinner party at all, but that it would be least risky in areas with only about 10–25 new cases per day, per 100,000 people.
The bottom line: Eating and drinking indoors with large groups of people, at a time when 150,000 people are contracting the virus every day, is about as risky as it gets.
The disease caused by the novel coronavirus has killed at least 247,000 people in the United States since February and has enveloped nearly every part of the country.
As health officials long predicted, autumn brought soaring case counts, strained hospital capacity and increased deaths nationwide, as the virus is not only popping up in new places but also circling back to areas that once appeared to have it contained. Nearly all metrics in most of the country are trending in the wrong direction.
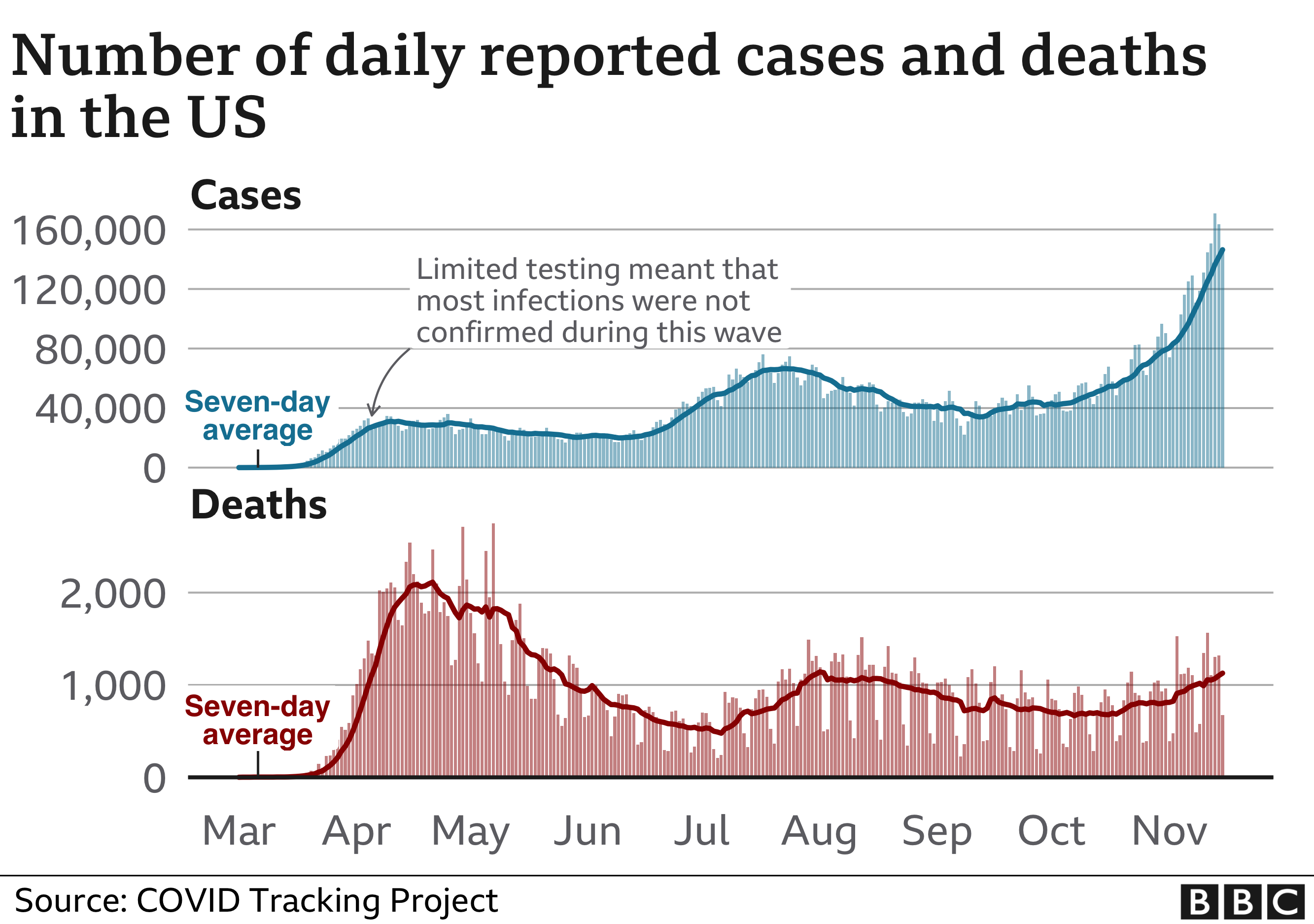
During an April peak, the seven-day-average U.S. death toll hit more than 2,000 per day, but cases were concentrated largely in the Northeast. During a July lull, average deaths sank to a low of 463 per day, although cases surged in the Sun Belt.
By early November, however, the country was recording more new cases than ever — well over 100,000 per day — and many states reported record-high caseloads and hospitalizations. The average U.S. deaths per day again shot past 1,000, despite improvements in treatment that make survival more likely.
In the past week in the U.S….New daily reported cases rose 26% New daily reported deaths rose 13.5% Covid related hospitalizations rose 23.9%.
Among reported tests, the positivity rate was 10%.
The number of tests reported rose 9.6% from the previous week.
Numbers in this article have fluctuated as testing and reporting criteria have evolved, particularly in areas that were hit early. Three spikes in the deaths chart above reflect large, one-time adjustments: In mid-April, New York City added more than 3,700 deaths. New Jersey added more than 1,800 on June 25. And in September, The Post changed its methodology for reporting deaths in New York and added a one-day increase of more than 2,700 on Sept. 18.
Health officials, including the country’s top infectious disease expert, Anthony S. Fauci, have said the virus has killed more people than official death tolls indicate.
New York, which was slammed with the new disease in spring and where at least 33,000 have died, is one of several states experiencing a second or even third wave.
Sun Belt states had serious outbreaks after Memorial Day when people flocked to beaches. By late summer, parts of the Midwest were inundated. In August and September, clusters appeared in newly reopened college campuses, particularly in the Northeast and Midwest. By October, Upper Midwest, Great Plains and Western states that had previously been mostly spared were reporting major outbreaks, including Minnesota, Wisconsin, Arkansas, the Dakotas and Alaska.
In November, most states reported record-high case counts and greater demand for hospital beds. Several set records for single-day fatalities.
A majority of states and many retail chains required masks in public places by late July, and public health officials touted them as one of the easiest ways to stop the pandemic. Still, some people in even the hardest-hit areas refuse to wear them, despite evidence that they protect wearers and those around them.
People older than 65 and those with obesity and underlying health problems are the mostly likely to die from covid-19, but a large percentage of infections occur in younger, more mobile people. People younger than 40 tend to become less sick but also unknowingly may pass the disease to others around them.
Sparsely populated areas don’t have the huge raw numbers that cities have reported, but some rank among the highest in deaths and cases per capita.
By late October, covid-19 had been documented in all but three U.S. counties and areas in Montana, the Dakotas and Idaho had some of the highest per capita caseloads.
People in very rural areas may be more vulnerable to covid-19 than urbanites, according to a Post analysis of CDC data.
Demand has often overwhelmed testing infrastructure, muddying the ability of officials to get a true picture of the virus’s reach. In June, CDC Director Robert Redfield estimated that, based on antibody tests, the actual number of U.S. residents who had been infected by the virus was likely to be 10 times as high as the number of confirmed cases. More recently, conflicting CDC guidelines about whether people without symptoms should be tested caused confusion and inhibited contact tracing.
A sharp increase in hospitalizations in late October and November demonstrates that the virus is spreading, not just that more testing is finding more asymptomatic cases. A group of Illinois health-care workers predicted in a Nov. 10 open letter to state and Chicago officials that “Illinois will surpass its ICU bed capacity by Thanksgiving.”
Some hospitals, straining to find beds and health-care workers to handle the crush of patients, are considering unusual measures.
In North Dakota, health-care workers who test positive but have no symptoms can continue working in covid-19 wards, according to Gov. Doug Burgum (R). Some facilities in Oklahoma, Kansas and Ohio are limiting routine care and deferring non-emergency surgeries.
Not all news is bleak, however.
On Nov. 9, Pfizer announced that its promising vaccine — one of many in the works — appeared more than 90 percent effective in an ongoing trial. The same day, regulators granted emergency authorization to an antibody treatment that may keep mild illness from becoming severe.
And the next day, Fauci told CNN that the average American may have access to a vaccine by April.
State-level reports are the best publicly available data on child COVID-19 cases in the United States. The American Academy of Pediatrics and the Children’s Hospital Association are collaborating to collect and share all publicly available data from states on child COVID-19 cases (definition of “child” case is based on varying age ranges reported across states; see report Appendix for details and links to all data sources).
As of November 12th, over 1 million children have tested positive for COVID-19 since the onset of the pandemic. The age distribution of reported COVID-19 cases was provided on the health department websites of 49 states, New York City, the District of Columbia, Puerto Rico, and Guam. Children represented 11.5% of all cases in states reporting cases by age.
A smaller subset of states reported on hospitalizations and mortality by age; the available data indicated that COVID-19-associated hospitalization and death is uncommon in children.
The number of new child COVID-19 cases reported this week, nearly 112,000, is by far the highest weekly increase since the pandemic began. At this time, it appears that severe illness due to COVID-19 is rare among children. However, there is an urgent need to collect more data on longer-term impacts on children, including ways the virus may harm the long-term physical health of infected children, as well as its emotional and mental health effects.
Summary of Findings (data available as of 11/12/20) :
(Note: Data represent cumulative counts since states began reporting)
Cumulative Number of Child COVID-19 Cases*
1,039,464 total child COVID-19 cases reported, and children represented 11.5% (1,039,464/9,037,991) of all cases
Overall rate: 1,381 cases per 100,000 children in the population
Change in Child COVID-19 Cases*
111,946 new child COVID-19 cases were reported the past week from 11/5-11/12 (927,518 to 1,039,464)
Over two weeks, 10/29-11/12, there was a 22% increase in child COVID-19 cases (185,829 new cases (853,635 to 1,039,464))
Testing (10 states reported)*
Children made up between 5.0%-17.4% of total state tests, and between 3.9%-18.8% of children tested were tested positive
Hospitalizations (23 states and NYC reported)*
Children were 1.2%-3.3% of total reported hospitalizations, and between 0.5%-6.1% of all child COVID-19 cases resulted in hospitalization
Mortality (42 states and NYC reported)*
Children were 0.00%-0.21% of all COVID-19 deaths, and 16 states reported zero child deaths
In states reporting, 0.00%-0.15% of all child COVID-19 cases resulted in death
* Note: Data represent cumulative counts since states began reporting; All data reported by state/local health departments are preliminary and subject to change
Coronavirus cases reported in the United States passed 11 million on Sunday, as the nation shatters records for hospitalizations and daily new infections and as leaders turn to new, painful restrictions to stem the pandemic’s long-predicted surge.
The milestone came one week after the country hit 10 million cases, a testament to just how rapidly the virus is spreading — the first 1 million cases took more than three months. This new wave has increased covid-19 hospitalizations past the peaks seen in April and July, straining health-care systems and pushing some reluctant Republican governors to enact statewide mask mandates for the first time.
Other states are reenacting stay-at-home orders and store closures. Michigan Gov. Gretchen Whitmer (D) on Sunday announced sweeping new limits on gatherings for three-weeks — including a ban on indoor dining at restaurants and bars, and a halt to in-person classes at high schools and colleges. Washington Gov. Jay Inslee (D) also laid out a slew of new rules, which prohibit indoor social gatherings with people outside one’s household and indoor service at restaurants, bars and more.
“As hard as those first months were for our state, these next few are going to be even harder,” Whitmer said at a news conference, as health experts fear that winter weather driving people indoors will accelerate the crisis.
Inslee acknowledged that slowing the virus would come at a steep price for struggling businesses, even as the state works to distribute millions more in aid. He and Whitmer both appealed to the federal government to step in with more help. Congress remains deadlocked on a stimulus package, and President Trump — still denying his election loss — has largely tuned out the pandemic’s surge; his refusal to concede is also stalling the transition to a new administration, including the formal transfer of information on the nation’s pandemic response.
Whitmer said that Trump has “an opportunity to meet the needs of the people of this country” and emphasized the importance of his final months in office. Inslee was already looking ahead to the administration of President-elect Joe Biden.
“All of us who feel, as I do, the pain of the small-business people ought to be pounding the doors of the Congress and the new president, who I’m glad we’re going to have, to really get this job done,” Inslee said.
Washington’s restrictions are not as tough as its stay-at-home order issued in March but extend into nearly every aspect of daily life. Wedding and funeral receptions are forbidden. Religious services and in-store retail are forced to operate at reduced capacity. Even outdoor social gatherings must be kept to a maximum of five people from outside one’s household.
Inslee and other leaders in the state emphasized the need to intervene early amid spiraling statistics, even as Washington posts some of the lowest numbers for new coronavirus infections in the country. The number of hospital patients with covid-19 recently rose about 40 percent in a week, officials said, and Seattle’s mayor said that nearly a fifth of the city’s cases have come just in the past two weeks.
Clint Wallace, an ICU nurse in Spokane, joined Inslee at Sunday’s news conference to plead with residents for their help. He called the ICU “as busy as I’ve seen it.”
“We are exhausted,” Wallace said of health-care workers around the state.
State and local officials nationwide are reinstating restrictions to fight the virus. New Mexico and Oregon on Friday ordered extensive new statewide shutdowns, while the Navajo Nation — devastated early on by the virus — reissued its stay-at-home order for at least three weeks. The Navajo Nation said cases threaten to swamp the health system on the southwestern reservation without immediate action.
North Dakota Gov. Doug Burgum (R) on Friday issued a statewide mask mandate and new capacity limits on businesses, less than a week after Utah Gov. Gary R. Herbert (R) announced a similar mask order in the face of overwhelmed hospitals warning that they might have to ration care.
“Our situation has changed, and we must change with it,” Burgum said in a late-night video message.
But state rules are just one piece of the puzzle, and some leaders are looking to Congress and the incoming president to take stronger action.
Ron Klain, Joe Biden’s incoming chief of staff, said Sunday it’s critical for the president-elect’s transition team to start working with Trump administration officials to ensure “nothing drops in this change of power” that could imperil the distribution of a potential coronavirus vaccine.
“Joe Biden is going to become president of the United States in the midst of an ongoing crisis. That has to be a seamless transition,” Klain said on NBC News’s “Meet the Press.”
President Trump’s White House is blocking the administration from formally cooperating with Biden, forcing the president-elect’s transition team to continue preparations with recently departed government officials and other experts. That means Biden’s team has not heard from Trump’s about vaccine development and other work to combat the pandemic.
A health expert on Biden’s covid-19 advisory board said there’s “a lot of information that needs to be transmitted. It can’t wait until the last minute.”
It is in the nation’s interest that the transition team get the threat assessments that the team knows about, understand the vaccine distribution plans, need to know where the stockpiles are, what the status is of masks and gloves,” said Atul Gawande, a surgeon at Brigham and Women’s Hospital and a professor at Harvard Medical School, on ABC News’s “This Week.”
Anthony S. Fauci, head of the National Institute of Allergy and Infectious Diseases, compared the process Sunday to “passing a baton in a race.”
“I’ve been through multiple transitions now, having served six presidents for 36 years, and it’s very clear that transition process that we go through … is really important in a smooth handing over of the information,” Fauci said on CNN’s “State of the Union.”
“Of course it would be better if we could start working with them,” he added when asked whether working with Biden’s team would serve the public interest.
On “Meet the Press,” Klain said there is “not that much Joe Biden can do right now to change things,” because he is not yet president.
“Right now we have a crisis that’s getting worse,” Klain said. “We had never had a day with 100,000 cases in a single day until last week. By next week, we may see 200,000 cases in a single day.”