5 Ways the Graham-Cassidy Proposal Puts Medicaid Coverage At Risk

The Graham-Cassidy proposal to repeal and replace the Affordable Care Act (ACA) is reviving the federal health reform debate and could come up for a vote in the Senate in the next two weeks before the budget reconciliation authority expires on September 30. The Graham-Cassidy proposal goes beyond the American Health Care Act (AHCA) passed by the House in May and the Better Care Reconciliation Act (BCRA) that failed in the Senate in July. The Graham-Cassidy proposal revamps and cuts Medicaid, redistributes federal funds across states, and eliminates coverage for millions of poor Americans as described below:
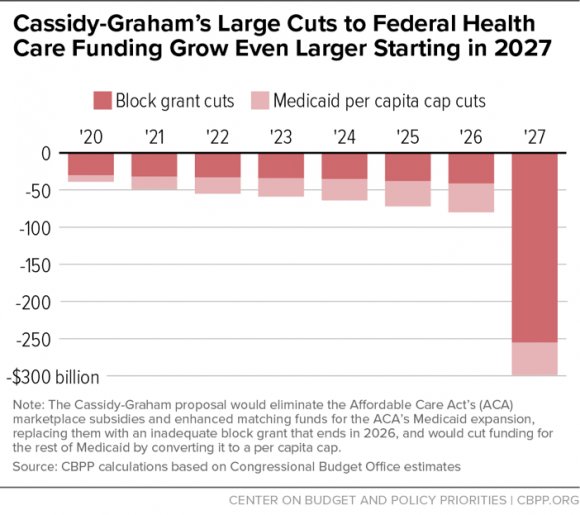
- Ends federal funding for current ACA coverage and partially replaces that funding with a block grant that expires after 2026. The proposal ends both the authority to cover childless adults and funding for the ACA Medicaid expansion that covers 15 million adults. Under Graham-Cassidy, a new block grant, the “Market-Based Health Care Grant Program,” combines federal funds for the ACA Medicaid expansion, premium and cost sharing subsidies in the Marketplace, and states’ Basic Health Plans for 2020-2026. Capped nationally, the block grant would be lower than ACA spending under current law and would end after 2026. States would need to replace federal dollars or roll back coverage. Neither the AHCA nor the BCRA included expiration dates for ACA-related federal funds or eliminated the ability for states to cover childless adults through Medicaid.
- Massively redistributes federal funding from Medicaid expansion states to non-expansion states through the block grant program penalizing states that broadened coverage. In 2020, block grant funds would be distributed based on federal spending in states for ACA Medicaid and Marketplace coverage. By 2026, funding would go to states according to the states’ portion of the population with incomes between 50% and 138% of poverty; the new allocation is phased in over the 2021-2025 period. The Secretary has the authority to make other adjustments to the allocation. This allocation would result in a large redistribution of ACA funding by 2026, away from states that adopted the Medicaid expansion and redirecting funding to states that did not. No funding is provided beyond 2026.
- Prohibits Medicaid coverage for childless adults and allows states to use limited block grant funds to purchase private coverage for traditional Medicaid populations. States can use funds under the block grant to provide tax credits and/or cost-sharing reductions for individual market coverage, make direct payments to providers, or provide coverage for traditional Medicaid populations through private insurance. The proposal limits the amount of block grant funds that a state could use for traditional Medicaid populations to 15% of its allotment (or 20% under a special waiver). These limits would shift coverage and funds for many low-income adults from Medicaid to individual market coverage. Under current law, 60% of federal ACA coverage funding is currently for the Medicaid expansion (covering parents and childless adults). Medicaid coverage is typically more comprehensive, less expensive and has more financial protections compared to private insurance. The proposal also allows states to roll back individual market protections related to premium pricing, including allowing premium rating based on health status, and benefits currently in the ACA.
- Caps and redistributes federal funds to states for the traditional Medicaid program for more than 60 million low-income children, parents, people with disabilities and the elderly. Similar to the BCRA and AHCA, the proposal establishes a Medicaid per enrollee cap as the default for federal financing based on a complicated formula tied to different inflation rates. As a result, federal Medicaid financing would grow more slowly than estimates under current law. In addition to overall spending limits, similar to the BCRA, the proposal would give the HHS Secretary discretion to further redistribute capped federal funds across states by making adjustments to states with high or low per enrollee spending.
- Eliminates federal funding for states to cover Medicaid family planning at Planned Parenthood clinics for one year. Additional funding restrictions include limits on states’ ability to use provider tax revenue to finance Medicaid as well as the termination of the enhanced match for the Community First Choice attendant care program for seniors and people with disabilities. Enrollment barriers include the option for states to condition Medicaid eligibility on a work requirement and to conduct more frequent redeterminations.
Much is at stake for low-income Americans and states in the Graham-Cassidy proposal. The recent debate over the AHCA and the BCRA has shown the difficulty of making major changes that affect coverage for over 70 million Americans and reduce federal funding for Medicaid. Medicaid has broad support and majorities across political parties say Medicaid is working well. More than half of the states have a strong stake in continuing the ACA Medicaid expansion as it has provided coverage to millions of low-income residents, reduced the uninsured and produced net fiscal benefits to states. Graham-Cassidy prohibits states from using Medicaid to provide coverage to childless adults. With regard to Medicaid financing changes, caps on federal funding could shift costs to states and result in less fiscal flexibility for states. States with challenging demographics (like an aging population), high health care needs (like those hardest hit by the opioid epidemic), high cost markets or states that operate efficient programs may have the hardest time responding to federal caps on Medicaid spending. Faced with substantially reduced federal funding, states would face difficult choices: raise revenue, reduce spending in other areas, or cut Medicaid provider payments, optional benefits, and/or optional coverage groups.