But there is still one dark cloud hanging over the vaccines that many people don’t yet understand.
The vaccines will be much less effective at preventing death and illness in 2021 if they are introduced into a population where the coronavirus is raging — as is now the case in the U.S. That’s the central argument of a new paper in the journal Health Affairs. (One of the authors is Dr. Rochelle Walensky of Massachusetts General Hospital, whom President-elect Joe Biden has chosen to run the Centers for Disease Control and Prevention.)
An analogy may be helpful here. A vaccine is like a fire hose. A vaccine that’s 95 percent effective, as Moderna’s and Pfizer’s versions appear to be, is a powerful fire hose. But the size of a fire is still a bigger determinant of how much destruction occurs.
I asked the authors of the Health Affairs study to put their findings into terms that we nonscientists could understand, and they were kind enough to do so. The estimates are fairly stunning:
At the current level of infection in the U.S. (about 200,000 confirmed new infections per day), a vaccine that is 95 percent effective — distributed at the expected pace — would still leave a terrible toll in the six months after it was introduced. Almost 10 million or so Americans would contract the virus, and more than 160,000 would die.
This is far worse than the toll in an alternate universe in which the vaccine was only 50 percent effective but the U.S. had reduced the infection rate to its level in early September (about 35,000 new daily cases). In that scenario, the death toll in the next six months would be kept to about 60,000.
It’s worth pausing for a moment on this comparison, because it’s deeply counterintuitive. If the U.S. had maintained its infection rate from September and Moderna and Pfizer had announced this fall that their vaccines were only 50 percent effective, a lot of people would have freaked out.
But the reality we have is actually worse.
How could this be? No vaccine can eliminate a pandemic immediately, just as no fire hose can put out a forest fire.While the vaccine is being distributed, the virus continues to do damage. “Bluntly stated, we’ll get out of this pandemic faster if we give the vaccine less work to do,” A. David Paltiel, one of the Health Affairs authors and a professor at the Yale School of Public Health, told me.
There is one positive way to look at this:Measures that reduce the virus’s spread — like mask-wearing, social distancing and rapid-result testing — can still have profound consequences. They can save more than 100,000 lives in coming months.
In the past seven days, 15,813 people in the U.S. died from the virus, breaking a record that had stood since mid-April.
Better leadership is needed on both ends of the chain, expert says.
The U.S. drug supply chain works well in the middle, but the beginning and end leave much room for improvement, according to Stephen Schondelmeyer, PharmD, PhD, of the University of Minnesota in Minneapolis.
“When a manufacturer imports a drug into the U.S. and sells it to wholesalers and then it goes to group purchasing organizations and through hospital institutional systems, that system works very well,” Schondelmeyer said last week at a public workshop of the National Academies of Science, Engineering, and Medicine’s Committee on Security of Medical Product Supply Chain. “But where problems occur is when the API [active pharmaceutical ingredient] is not being produced or is not available, or is not shipped to the finished dose manufacturer to make enough.” With the current “just in time” manufacturing system, “inventories may only last a month” before supplies dry up, he said.
Leadership on this issue “is certainly needed at the top, but also needed at the end,” said Schondelmeyer, who is co-principal investigator of the Resilient Drug Supply Project at the university’s Center for Infectious Disease Research and Policy.
For example, he said, “I routinely meet with groups of pharmacy directors at major hospital systems. I have heard stories from pharmacy directors … who have said they had remdesivir allocated by their state; it showed up in their hospital’s lab. Nobody in the lab knew what it was or why it arrived, and it sat there for several days before they figured out this was a drug and pharmacy should be managing this … You can run a marathon, but if you don’t finish the last 200 yards, you don’t finish the marathon, and that’s what happened with remdesivir.”
“We need to be predicting not only demand changes but what things can create a supply disruption, because a lot of shortages we have are from supply disruption,” Schondelmeyer said. In the COVID-19 era, this could include unexpected political moves such as export bans — such as those recently put in place in India and the United Kingdom — which could mean that “we could find whole categories of drugs not available in the U.S., and we don’t have the capacity to replace that supply, in the short run at least,” he said.
Pharmaceuticals are a very unique market, he added. “We established a pharmaceutical market based on monopolies when drugs first come on the market, via intellectual property, and even later on, when you’re down to two or three generics they function like an oligopoly. We have a marketplace that has extreme asymmetries of information, where people selling a drug know a lot more than people buying the drug. We have to establish an infrastructure to understand the pharmaceutical market and the flow of products so we can correct the market when it’s not working.”
“Our current system of fixing drug shortages is a ‘fail and fix’ system,” he said. The list of shortages “is a list of products that have already failed. I think we should have a system that has supply chain maps that identify critical stages — even pre-API — that can suggest where we might have a failure, and do something before the failure occurs. I suggest we move from ‘fail and fix’ to ‘predict and prevent.'”
Schondelmeyer said he and his colleagues are trying to build such supply chain maps, “but really the government should be doing that … I don’t fault the FDA; the FDA may or may not be the right place to do that.” But more agencies and other players need to be involved because “no one player in the market can solve this problem alone.”
Schondelmeyer displayed percentages of various drug types that were in shortage. Among 156 “critical acute care drugs” — those that must be used within hours or days of an illness’s onset to avoid serious outcomes or death — the FDA found 25.6% were in shortage, while the American Society of Hospital Pharmacists (ASHP) found that 41.7% of them were in shortage, “and this was even before COVID-19,” he said. Among a list of 40 “critical COVID-19 drugs,” the FDA has listed 45% of them as being in shortage, while the ASHP rated 75% as being in shortage. “Most were in short supply even before COVID-19 hit,” he added. “These are alarming levels of shortage and they have persisted.”
Many people suggest that the supply chain problem can be solved by moving manufacturing for particular drug products from overseas to a U.S. plant, but that doesn’t quite solve the problem, said Schondelmeyer. “If we manufactured our entire supply of drugs in the U.S., it doesn’t solve the problem if you put all the manufacturing in one facility and it gets wiped out by a hurricane,” he said, recalling what happened when a hurricane hit Puerto Rico, the home of several medical product manufacturers. “Hospitals were scrambling to get things like normal saline. So simply bringing production back to the U.S. but concentrating it in one place doesn’t solve the problem — it just moves the problem.”
Khatereh Calleja, president and CEO of the Healthcare Supply Chain Association, agreed. “We’ve got to focus on this very issue of geographic diversity,” Calleja said. “Otherwise we’re creating a risk when we create that concentration.”
When people are discussing the supply chain, having a common language among institutions is also important, said Chris Liu, director of enterprise services for the state of Washington, “In hospitals, ‘conservation’ of PPE [personal protective equipment] means something different at every hospital you go to,” he said.
Another thing that needs to be taken on is the vulnerability of drug precursors, said James Lawler, director of international programs and innovation at the University of Nebraska’s Global Center for Health Security. “It’s one thing if the plant that makes the final small-molecule antibiotic … is in the U.S., but if all the precursor chemicals they require to synthesize that product come from overseas, you haven’t necessarily fixed your supply chain vulnerability.”
Americans have made no secret of their skepticism of COVID-19 vaccines this year, with fears of political interference and a “warp speed” timeline blunting confidence in the shots. As recently as September, nearly half of U.S. adults said they didn’t intend to be inoculated.
But with two promising vaccines primed for release, likely within weeks, experts in ethics and immunization behavior say they expect attitudes to shift quickly from widespread hesitancy to urgent, even heated demand.
“People talk about the anti-vaccine people being able to kind of squelch uptake. I don’t see that happening,” Dr. Paul Offit, a vaccinologist with Children’s Hospital of Philadelphia, told viewers of a recent JAMA Network webinar. “This, to me, is more like the Beanie Baby phenomenon. The attractiveness of a limited edition.”
Reports that vaccines produced by drugmakers Pfizer and BioNTech and Moderna appear to be safe and effective, along with the deliberate emphasis on science-based guidance from the incoming Biden administration, are likely to reverse uncertainty in a big way, said Arthur Caplan, director of the division of medical ethics at New York University School of Medicine.
“I think that’s going to flip the trust issue,” he said.
The shift is already apparent. A new poll by the Pew Research Center found that by the end of November 60% of Americans said they would get a vaccine for the coronavirus. This month, even as a federal advisory group met to hash out guidelines for vaccine distribution, a long list of advocacy groups — from those representing home-based health workers and community health centers to patients with kidney disease — were lobbying state and federal officials in hopes their constituents would be prioritized for the first scarce doses.
“As we get closer to the vaccine being a reality, there’s a lot of jockeying, to be sure,” said Katie Smith Sloan, chief executive of LeadingAge, a nonprofit organization pushing for staff and patients at long-term care centers to be included in the highest-priority category.
Certainly, some consumers remain wary, said Rupali Limaye, a social and behavioral health scientist at the Johns Hopkins Bloomberg School of Public Health. Fears that drugmakers and regulators might cut corners to speed a vaccine linger, even as details of the trials become public and the review process is made more transparent. Some health care workers, who are at the front of the line for the shots, are not eager to go first.
“There will be people who will say, ‘I will wait a little bit more for safety data,” Limaye said.
But those doubts likely will recede once the vaccines are approved for use and begin to circulate broadly, said Offit, who sits on the FDA advisory panel set to review the requests for emergency authorization Pfizer and Moderna have submitted.
He predicted demand for the COVID vaccines could rival the clamor that occurred in 2004, when production problems caused a severe shortage of flu shots just as influenza season began. That led to long lines, rationed doses and ethical debates over distribution.
“That was a highly desired vaccine,” Offit said. “I think in many ways that might happen here.”
Initially, vaccine supplies will be tight, with federal officials planning to ship 6.4 million doses within 24 hours of FDA authorization and up to 40 million doses by the end of the year. The CDC panel recommended that the first shots go to the 21 million health care workers in the U.S. and 3 million nursing home staff and residents, before being rolled out to other groups based on a hierarchy of risk factors.
Even before any vaccine is available, some people are trying to boost their chances of access, said Dr. Allison Kempe, a professor of pediatrics at the University of Colorado School of Medicine and expert in vaccine dissemination. “People have called me and said, ‘How can I get the vaccine?’” she said. “I think that not everyone will be happy to wait, that’s for sure. I don’t think there will be rioting in the streets, but there may be pressure brought to bear.”
That likely will include emotional debates over how, when and to whom next doses should be distributed, said Caplan. Under the CDC recommendations, vulnerable groups next in line include 87 million workers whose jobs are deemed “essential” — a broad and ill-defined category — as well as 53 million adults age 65 and older.
“We’re going to have some fights about high-risk groups,” said Caplan of NYU.
The conversations will be complicated. Should prisoners, who have little control over their COVID exposure, get vaccine priority? How about professional sports teams, whose performance could bolster society’s overall morale? And what about residents of facilities providing care for people with intellectual and developmental disabilities, who are three times more likely to die from COVID-19 than the general population?
Control over vaccination allocation rests with the states, so that’s where the biggest conflicts will occur, Caplan said. “It’s a short fight, I hope, in the sense in which it gets done in a few months, but I think it will be pretty vocal.”
Once vaccine supplies become more plentiful, perhaps by May or June, another consideration is sure to boost demand: requirements for proof of COVID vaccination for work and travel.
“It’s inevitable that you’re going to see immunity passports or that you’re required to show a certificate on the train, airplane, bus or subway,” Caplan predicted. “Probably also to enter certain hospitals, probably to enter certain restaurants and government facilities.”
But with a grueling winter surge ahead, and new predictions that COVID-19 will fell as many as 450,000 Americans by February, the tragic reality of the disease will no doubt fuel ample demand for vaccination.
“People now know someone who has gotten COVID, who has been hospitalized or has unfortunately died,” Limaye said.
“We’re all seeing this now,” said Kempe. “Even deniers are beginning to see what this illness can do.”
Trump administration officials deny there will be availability issues, but others say problems are possible in the second quarter.
Pfizer has told the Trump administration it cannot provide substantial additional doses of its coronavirus vaccine until late June or July because other countries have rushed to buy up most of its supply, according to multiple individuals familiar with the situation.
That means the U.S. government may not be able to ramp up as rapidly as it had expected from the 100 million doses of the Pfizer vaccine that it purchased earlier this year, raising questions about whether it can keep to its aggressive schedule to vaccinate most Americans by late spring or early summer.
Trump administration officials denied there would be availability issues in the second quarter, citing other vaccines in the pipeline — most immediately, Moderna’s, also expected to be approved in coming weeks. Both vaccines are two-dose regimens, so the 100 million doses purchased of each would cover 50 million people each.
“I’m not concerned about our ability to buy vaccines to offer to all of the American public,” Gen. Paul Ostrowski, who oversees logistics for Operation Warp Speed, the government’s initiative to expedite vaccine development, said in an interview Monday. “It’s clear that Pfizer made plans with other countries. Many have been announced. We understand those pieces.”
But several officials knowledgeable about the contracts said that supplies from other companies may be insufficient to fill the gap.
Last summer, Pfizer officials had urged Operation Warp Speed to purchase 200 million doses, or enough of the two-shot regimen for 100 million people, according to people knowledgeable about the issue who spoke on the condition of anonymity because they weren’t authorized to discuss the situation. But the Warp Speed officials declined, opting instead for 100 million doses, they said. The New York Times first reported that federal officials passed on the opportunity when Pfizer offered to sell more doses.
“Anyone who wanted to sell us … without an [FDA] approval, hundreds of millions of doses back in July and August, was just not going to get the government’s money,” said a senior administration official.
It was only last weekend, with a Food and Drug Administration clearance expected any day, that federal officials reached back out to the company asking to buy another 100 million doses. By then, Pfizer said it had committed the supply elsewhere and suggested elevating the conversation to “a high level discussion,” said a person familiar with the talks.
Pfizer said the company might be able to provide 50 million doses at the end of the second quarter, and another 50 million doses in the third quarter, the individuals said.
The government had a different type of contract with Pfizer than with other companies involved with Operation Warp Speed. Pfizer was the only company that did not take government money for research and development, which meant U.S. officials have had less insight into its decisions than it does with the other companies, said a senior administration official familiar with the matter who spoke on the condition of anonymity.
The contract between the government and Pfizer stipulated that if Pfizer’s vaccine was successful and received authorization from the FDA, the U.S. government would purchase 100 million doses at a set price.
Pfizer spokeswoman Amy Rose declined to confirm any information about the company’s discussions with the government, and said that beyond the first 100 million doses the U.S. has already secured, a separate agreement would have to be negotiated.
President Trump is expected to sign an executive order Tuesday that would prioritize vaccinating Americans before providing doses to other countries, according to a senior administration official who requested anonymity because he was not authorized to speak about the plans. Fox News first reported the executive order. It is not clear whether the order is related to the Pfizer supply issue, or whether the president can prevent an American company from fulfilling lawful contracts with other countries.
“The executive order reaffirms to the American people that we are going to put America first,” said a senior administration official, who spoke on the condition of anonymity because he was not authorized to discuss the issue publicly.
The order will be announced as part of a White House “vaccine summit” designed to highlight the administration’s accomplishments on vaccines.
The vaccine by Pfizer and German biotech firm BioNTech is expected to receive emergency authorization from the FDA in the next several days, and Moderna is lined up for likely clearance shortly after that. Shipments of the vaccines will begin within 24 hours of the approvals, federal officials have said.
Warp Speed officials hope that other companies with promising vaccine candidates will supplement the supply in the near future, but some are still conducting late-stage clinical trials, while others haven’t begun them.
That means it could be several weeks to months before they are ready to apply to the FDA for clearance. One of the companies, AztraZeneca recently reported encouraging vaccine data, but experts raised questions about it and what it meant about the efficacy of the vaccine.
Moncef Slaoui, chief science adviser to Warp Speed, said in an interview Monday that the U.S. government strategy was to spread its risk widely over many different types of vaccines from different manufacturers. He declined to comment on negotiations with any company, but said he did not believe there would be any kind of vaccine “cliff,” where the available doses would fall off sharply.
Slaoui said that Johnson & Johnson was likely to report trial results in early January and be ready to ship doses in February, if its vaccine is authorized. He predicted that AstraZeneca’s trial would report results in late January or early February and potentially begin providing doses later that month.
“We could have all of them,” Slaoui said. “And for this reason, we feel confident we could cover the needs without a specific cliff … We have planned things in such a way as we would indeed avoid a cliff.”
The contract that Pfizer signed with the government in July was to deliver 100 million vaccine doses, and contained an option to contract to buy an additional 500 million doses.
“Pfizer shall inform the Government of appropriate lead times based on purchase of raw materials, capacity reservation and other factors, and Pfizer and the Government shall mutually agree on an appropriate estimated delivery schedule,” the contract states.
“Recognizing the urgency of the need, our manufacturing teams have been working around-the-clock so we can bring the vaccine to the world as quickly, efficiently and equitably as possible,” Rose said.
Additional doses would be “subject to a separate and mutually acceptable agreement” she said.
No agreements with Moderna beyond its initial contract for 100 million have been announced, but the U.S. has the option to purchase 400 million additional doses. Moderna is expected to deliver 20 million doses by year’s end and another tranche in the first quarter of 2021.
We are now in uncharted and dangerous new territory in the coronavirus pandemic, with the US recording a record-high 2,800 deaths on Thursday, along with 200,000 new cases—the second highest daily total of the pandemic so far.
More than 100,000 Americans are now hospitalized with COVID-19, occupying more than 10 percent of the nation’s hospital beds, and creating capacity constraints at hospitals around the country. With the impact of Thanksgiving travel—which was the heaviest since March—yet to be seen in the numbers, and with hospitalizations and deaths lagging new case counts by several weeks (as an epidemiological rule of thumb, 1.7 percent of new cases will result in reported deaths from COVID after 22 days), we are almost certainly headed for a grim winter holiday season.
But the light at the end of the tunnel grew brighter this week, with the United Kingdom becoming the first Western country to approve a COVID vaccine. (China and Russia both rolled out vaccines prior to Phase 3 trials being completed.)
Doctors and hospital staff in the UK will begin to administer Pfizer’s vaccine next week, and the US Food and Drug Administration (FDA) is expected to approve the same vaccine for emergency use on or shortly after an outside panel of experts convenes on December 10th.
Moderna, whose vaccine is similar to Pfizer’s, submitted an application for emergency use this week, and it will be evaluated on December 17th.
In the meantime, a group advising the Centers for Disease Control and Prevention (CDC) held a public meeting this week to craft recommendations for which populations should be prioritized to receive the new vaccines, settling on healthcare workers and residents of long-term care facilities as first in line. While state public health officials will make the final decisions about who gets vaccinated, most are expected to follow the CDC’s guidelines. The two priority groups represent about 24M people, most of whom could be immunized by the end of this month if all goes according to plan. The end of the pandemic will not come quickly, or easily, but it will come—we are near the beginning of the end.
President-elect Joe Biden’s front-runner for secretary of Health and Human Services is New Mexico Governor Michelle Lujan Grisham, and he may announce several of his administration’s health leaders as soon as next week, according to people familiar with the matter.
The position of HHS secretary is down to two possibilities, the people said, between Lujan Grisham and former Surgeon General Vivek Murthy, a co-chair of the coronavirus advisory board Biden appointed shortly after he was elected.
Biden’s health team will assume office with the U.S. still suffering from the pandemic, as virus cases and hospitalizations soared over the past month. His health secretary is expected to have input on filling other top health posts, such as FDA commissioner and the administrator of the Centers for Medicare and Medicaid Services, the people said, so those appointments may not be announced until later.
The Health and Human Services secretary will have the tough task of rebuilding Obamacare, which Biden has promised to expand. That will be a difficult undertaking with a Republican-led Senate.
Murthy or Jeff Zients, who led the Obama administration effort to repair healthcare.gov, the faulty Obamacare website, may be named to a leadership role on the pandemic, according to the people familiar with the matter — a “Covid-19 czar.”
Mandy Cohen, the North Carolina state health secretary, is a favorite for CMS, the people said. Biden’s choices to lead the Food and Drug Administration appear narrowed down to David Kessler, a former commissioner of the agency who is another co-chair of his coronavirus advisory board, and Joshua Sharfstein, a former FDA official who is a vice dean at Johns Hopkins University’s Bloomberg School of Public Health.
Biden announced his economic team on Tuesday, a group led by Treasury Secretary-designate Janet Yellen whose top priority will be restoring jobs eliminated by the pandemic. An announcement on some of his health team could come as soon as Monday, the people said.
The people familiar with the matter asked not to be identified because talks are still ongoing and no final decision has been made. It’s not clear how many people will be announced at once, or which positions would later be filled by the health secretary once the Biden administration is in place.
Biden’s transition team did not immediately respond to a request for comment.
The U.S. recorded 158,000 new coronavirus infections on Monday and a record 205,000 cases three days earlier. Biden will take office as distribution of coronavirus vaccines ramps up, and he has warned that any delay in the transition to his administration could slow or complicate that endeavor.
Lujan Grisham is seen as having an easier path to confirmation than Murthy, who has spoken out against gun violence as a public health threat and may draw strong opposition from Senate Republicans as a result, the people familiar with the matter said.
If he isn’t nominated to lead HHS, Murthy is under consideration as Covid-19 czar or another role, including a second stint as surgeon general, the people said. Murthy talks to Biden almost every day as co-chair of his advisory board and is seen as having influential supporters.
Murthy and Zients have also represented Biden’s transition team on calls with current HHS officials, two of the people said.
Biden’s team is still discussing what the White House coronavirus task force and Operation Warp Speed — the Trump administration’s effort to fast-track vaccines — will look like under the new administration.
If Biden announces his health team next week, he may be just days ahead of the first emergency FDA approval of a coronavirus vaccine. President Donald Trump is planning a vaccine summit next week at the White House, while an FDA advisory panel is scheduled to meet on Dec. 10 to discuss the shots.
People who refuse a vaccine for COVID-19 could find normal life curtailed as restaurants, bars, cinemas and sports venues could block entry to those who don’t have proof they are inoculated, Britain’s new vaccine minister said on Monday.
Several major COVID-19 vaccines have been announced in recent weeks, raising hopes that the world could soon return to some semblance of normality after the coronavirus killed 1.46 million people and wiped out a chunk of the global economy.
The British minister responsible for the vaccine rollout, Nadhim Zahawi, said getting vaccinated should be voluntary but that Google, Facebook and Twitter should do more to fact-check opposing views of vaccines.
Asked by the BBC if there would be an immunity passport, Zahawi said a person’s COVID-19 vaccine status might be included in a phone app that would inform local doctors of a person’s status.
“But also I think you’d probably find that restaurants and bars and cinemas and other venues, sports venues, will probably also use that system as they’ve done with the app,” Zahawi told the BBC.
“The sort of pressure will come both ways: from service providers – who will say ‘look, demonstrate to us that you have been vaccinated’ – but also we will make the technology as easy and accessible as possible.”
Health authorities in many countries have become increasingly concerned in recent years by the growth of anti-vaccine groups, which are especially active on social media.
Asked if it would become virtually impossible to do anything without the vaccine, Zahawi said: “I think people have to make a decision but I think you’ll probably find many service providers will want to engage in this in the way they did with the app.”
Zahawi declined to give any specific date on a vaccine rollout as none have yet been approved for public use.
The message, he said, should be that a vaccine is good for the community and the country.
AstraZeneca on Monday became the third pharmaceutical company to announce remarkable results from late-stage trials of a coronavirus vaccine, saying that its candidate, developed by Oxford University, is up to 90 percent effective.
This is the third straight week to begin with buoyant scientific news that suggests, even as coronavirus cases surge to devastating levels in many countries, an end to the pandemic is in sight.
Pfizer and its German partner BioNTech and Moderna have each reported vaccines that are 95 percent effective in clinical trials. A direct comparison to the Oxford-AstraZeneca vaccine is complicated, due to the trial design, but the vaccine may be a more realistic option for much of the world, as it is likely to be cheaper and does not need to be stored at subzero temperatures.
Peter Piot, director of the London School of Hygiene & Tropical Medicine, who was instrumental in the battle against AIDS, said the positive results from three vaccine candidates cannot be overestimated.
“2020 will be remembered for the many lives lost from covid-19, lockdowns and the U.S. election. Science should now be added to this list,” said Piot, adding, “the only way to stop covid-19 in its tracks is having multiple effective and safe vaccines that can be deployed all around the world and in vast quantities.”
“I’m totally delighted,” said Hildegund C.J. Ertl, a vaccine expert at the Wistar Institute in Philadelphia. Adding to the results from Pfizer and Moderna, “what it tells me is this virus can be beaten quite easily: 90 to 95 percent efficacy is something we’d dream about for influenza virus, and we’d never get it.”
The Oxford-AstraZeneca team said in a video conference with journalists that its candidate offered 90 percent protection against the virus when a subject received a half-dose, followed with a full dose one month later. Efficacy was lower — 62 percent — when subjects received two full doses a month apart. The interim results, therefore, averaged to 70 percent efficacy.
Andrew Pollard, chief investigator of the Oxford trial, said the findings showed the vaccine would save many lives.
“Excitingly, we’ve found that one of our dosing regimens may be around 90 percent effective, and if this dosing regimen is used, more people could be vaccinated with planned vaccine supply,” he said.
Britain has preordered 100 million doses — which at a dose and a half per person would cover most of its population. The United States has ordered 300 million.
The results have yet to be peer-reviewed or published, and will be scrutinized by regulators. Many questions remain, including whether the vaccine can reduce transmission of the virus by people without symptoms, which would have repercussions for how soon people could stop wearing masks. It is also unclear how long the immunity from the vaccine lasts — a crucial question.
Sarah Gilbert, a lead Oxford researcher, cautioned that the dose-and-a-half regimen would have to be more closely studied to be fully understood. But she said the first half-dose might be priming a person’s immune system just enough, and that the second booster then encourages the body to produce a robust defense against sickness and infection.
AstraZeneca and Oxford have been conducting Phase 3 clinical trials worldwide, with the most recent data coming from an interim analysis based on 131 coronavirus infections in Britain and Brazil among 10,000 volunteers, with half getting the vaccine and half getting a placebo.
The company said it would present the results to Britain’s health-care products regulators immediately and would seek approval to fine-tune its clinical trials in the United States, to further assess the half-dose shot followed by a booster.
Because the vaccine is already in production, if approved, the first 4 million doses could be ready in December, and 40 million could be delivered in the first quarter of 2021, company executives said. By the spring, the company and its global partners in India, Brazil, Russia and the United States could be cranking out 100 million to 200 million doses a month.
British Health Secretary Matt Hancock said “should all that go well, the bulk of the rollout will be in the new year.”
In a statement to Parliament, Prime Minister Boris Johnson said that vaccines were “edging ever closer to liberating us from the virus, demonstrating emphatically that this is not a pandemic without end. We can take great heart from today’s news, which has the makings of a wonderful British scientific achievement.”
World markets have rallied on optimistic vaccine news, though shares in AstraZeneca were down Monday on the London stock exchange.
No participants who received the vaccine developed severe cases or required hospitalization, AstraZeneca said Monday. The drugmaker also said that no “serious safety events” were reported in connection with the vaccine, which was typically “well tolerated” by participants regardless of their dosing levels or ages.
The vaccine uses a harmless cold virus that typically infects chimpanzees to deliver to the body’s cells the genetic code of the spike protein that dots the outside of the coronavirus. That teaches the body’s immune system to recognize and block the real virus.
Although the reason the regimen with an initial half-dose worked better remains to be teased out, Ertl said that it could be related to the fact that the body’s immune system can develop a defense system to block the harmless virus that’s used to deliver the spike protein’s code. Giving a smaller initial dose may lessen those defenses, and make the vaccine more effective.
Several other vaccines in late-stage development use a similar technology, harnessing a harmless virus to deliver a payload that will teach the immune system how to fight off the real thing — including the Johnson & Johnson vaccine, the Russian vaccine being developed by the Gamaleya Research Institute and the vaccine made by CanSino Biologics in China.
While the results released by AstraZeneca indicate somewhat lower efficacy than Pfizer and Moderna, the vaccine can be stored and transported at normal refrigerated conditions for up to six months. That could make it significantly easier to roll out than Pfizer’s vaccine, which has to be stored at minus-70 degrees Celsius, or Moderna’s, which is stable in refrigerated conditions for only 30 days and must be frozen at minus-20 degrees Celsius after that.
The Oxford-AstraZeneca vaccine was first developed in a small laboratory running on a shoestring budget by Gilbert at Oxford and her team. The university kicked in 1 million pounds ($1.3 million) and then sought a manufacturing partner, before settling on AstraZeneca.
“We wanted to ensure there wouldn’t be any profiteering off the pandemic,” said Louise Richardson, the university’s vice chancellor, so that their vaccine would be widely distributed “and wouldn’t just be for the wealthy and the first world.”
The scientists said that although it appeared to be a race, or a competition, among the front-running vaccine developers, no one company could produce by itself the millions of doses needed to end the pandemic.
“We don’t have enough supply for the whole planet,” Pollard said, adding that the important message is that today there are at least three highly effective, safe vaccines, that also appear to work well among the elderly, and that they are produced using different technologies, ensuring the quickest route to manufacture the billions of doses that will be necessary.
Pollard said it is “unclear why” the different vaccines were producing different results, and he said he and the scientific community awaited full data sets from all the clinical trials to fully understand what is going on. He said different studies were also using different end points to describe efficacy.
“At this moment we can’t fully explain the differences,” Pollard said. “It’s critical to understand what everyone is measuring.”
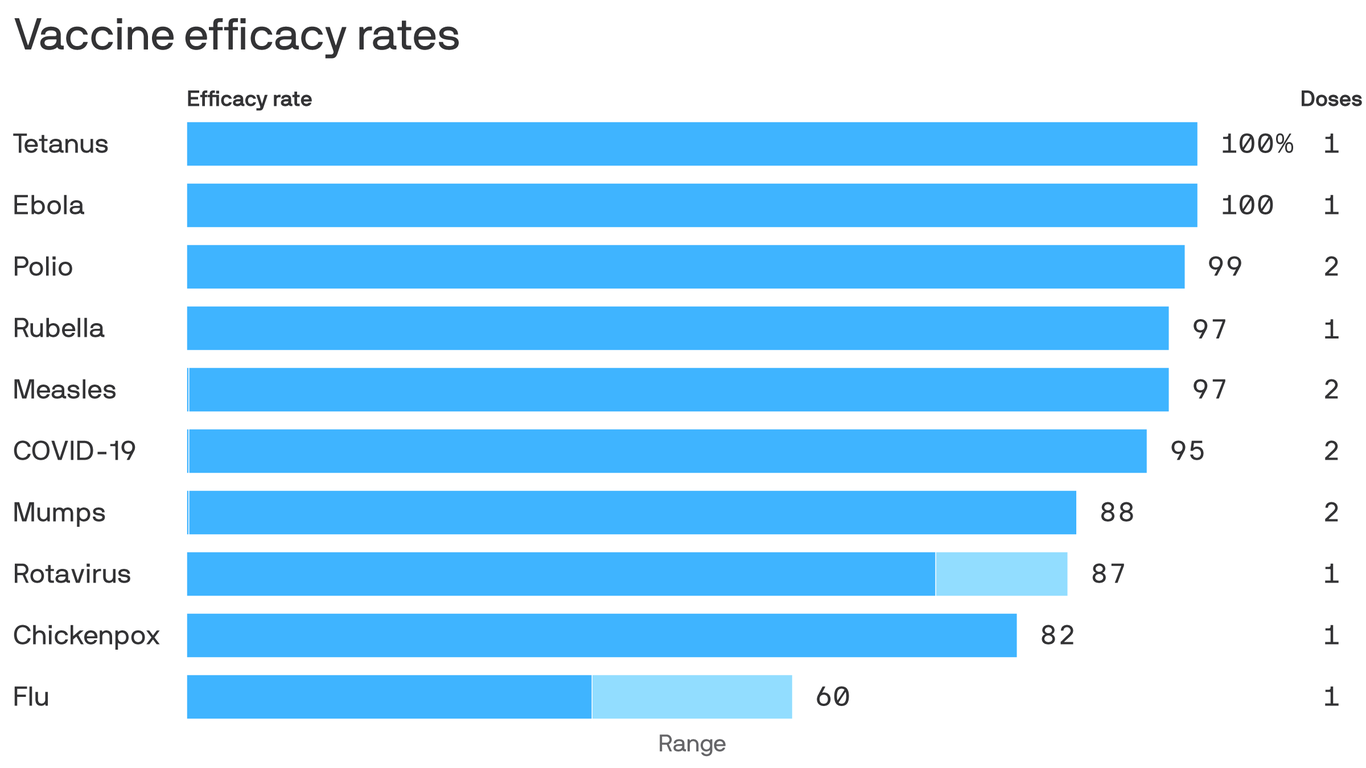
The leading coronavirus vaccines are shaping up to be on par with some of the most effective vaccines in medicine, Axios’ Marisa Fernandez reports.
Why it matters:Vaccines with efficacy rates of about 95% — which both Pfizer and Moderna say they’ve achieved — will be more powerful weapons against the coronavirus than many experts had anticipated.
Flashback: The Food and Drug Administration initially set the bar for a COVID-19 vaccine at 50% efficacy, roughly in line with the seasonal flu vaccine.
Some scientists had hoped, in a best-case scenario, it might be as much as 70% effective.
“We don’t know yet what the efficacy might be. We don’t know if it will be 50% or 60%. I’d like it to be 75% or more,” the NIH’s Anthony Fauci said in August.
But coming in closer to 95% would put Pfizer and Moderna’s vaccines more in line with the highly effective inoculations against measles, mumps and rubella.
Like the MMR and polio vaccines, both prospective COVID-19 products would require two shots to reach that level of efficacy.
The third leading contender, being developed by AstraZeneca and Oxford University, would also require two shots. Johnson & Johnson is testing both a single-dose and a two-dose vaccine in simultaneous phase 3 trials.
Yes, but: There’s still a lot we don’t know about these vaccines, including how well they’re likely to work among various demographic groups, and how long the immunity they confer will last.
Like a lot of people, I have really gotten into listening to podcasts over the last year. They’re such an immersive way to learn about the world, and I like how the format lets you dive as deep on a topic as you want. So, I was inspired to start one of my own—but I knew I couldn’t do it on my own.
I couldn’t ask for a better partner on this project than Rashida Jones. A mutual friend suggested that the two of us might have a lot to talk about, and it turned out he was right. I already knew she was a talented actor, but I was impressed by her thoughtful perspective on the world. So, we decided to start a podcast that lets us think through some of today’s most pressing problems together. In our first episode, Rashida and I explore a big question that is top of mind for many people: what will the world look like after COVID-19?
I know it’s hard to imagine right now while new cases are surging around the world, but there will come a time when the COVID-19 pandemic is behind us. I think it’s safe to assume that society will be changed forever, given how disruptive the virus has been to virtually every part of our lives.
Unfortunately, we still have a long way to go before life truly gets back to “normal.” Rashida and I were joined by Dr. Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases, to discuss what to expect in the months to come. I’ve had the opportunity to work with Dr. Fauci on a number of global health issues over the years, including the quest for an HIV vaccine and cure. He’s such a quiet and unassuming guy normally, so it’s been wild to watch him become a huge celebrity.
Dr. Fauci and I are both optimistic that a vaccine will bring an end to the pandemic at some point in the near future. But what the world looks like after that is a lot less clear. I suspect that some of the digitization trends we’ve seen—especially in the areas of online learning, telemedicine, and remote work—will become a regular part of our lives. I hope this episode leaves you hopeful about the future and curious about what comes next.