Sen. Bernie Sanders’ “Medicare for All” plan would drastically change not only how health care is paid for, but who ultimately pays for it.
While the wealthy and the poor usually pay the same premium for today’s employer-based insurance, Sanders’ plan would beef up insurance coverage for everyone and pay for it by increasing taxes on the wealthy.
Driving the news: As part of yesterday’s rollout, Sanders released a white paper with several “options” on how to raise the additional revenue it would take for the government to pay for everyone’s health care without any premiums or out-of-pocket costs.
While most people’s taxes would go up, the wealthy would pay for a much greater portion of the nation’s health care system than they currently do.
A 4% “income-based premium” for workers who make more than $29,000 and a 7.5% “income-based premium” on employers (exempting the first $2 million in payroll) are two of the financing options. Most economists assume that the employer tax would get passed onto employees through lost wages.
Other options include increasing the individual tax rate on high earners, taxing “unearned” income at the same rate as earned, and establishing a wealth tax.
What they’re saying: Even if all of these payment options were implemented, they still wouldn’t cover the total cost of Sanders’ plan, said the Committee for a Responsible Federal Budget’s Marc Goldwein.
He said there could also be unintended consequences of such high taxes on the wealthy, such as discouraging investment.
The bottom line: “More progressive tax-based financing of health care is a feature, not a bug, of Medicare for all,” the Kaiser Family Foundation’s Larry Levitt said.
“The idea of financing health care through taxes rather than premiums and out-of-pocket costs would be fairer in some people’s minds, but also disruptive,” he said.
The epidemic of rural hospital closures is threatening small towns such as Celina, Tenn. The town of 1,500 has been trying to position itself as a retiree destination but that task has grown more difficult since the March 1 closure of 25-bed Cumberland River Hospital.
KEY TAKEAWAYS
Celina became the 11th rural hospital in Tennessee to close in recent years — more than in any state but Texas. Both states have refused to expand Medicaid in a way that covers more of the working poor.
The closest hospital is now 18 miles away. That adds another 30 minutes through mountain roads for those who need an X-ray or bloodwork. For those in the back of an ambulance, that bit of time could mean the difference between life or death.
When a rural community loses its hospital, health care becomes harder to come by in an instant. But a hospital closure also shocks a small town’s economy. It shuts down one of its largest employers. It scares off heavy industry that needs an emergency room nearby. And in one Tennessee town, a lost hospital means lost hope of attracting more retirees.
Seniors, and their retirement accounts, have been viewed as potential saviors for many rural economies trying to make up for lost jobs. But the epidemic of rural hospital closures is threatening those dreams in places like Celina, Tenn. The town of 1,500, whose 25-bed hospital closed March 1, has been trying to position itself as a retiree destination.
“I’d say, look elsewhere,” said Susan Scovel, a Seattle transplant who arrived with her husband in 2015.
Scovel’s despondence is especially noteworthy given she leads the local chamber of commerce effort to attract retirees like herself. She considers the wooded hills and secluded lake to hold scenic beauty comparable to the Washington coast — with dramatically lower costs of living; she and a small committee plan getaway weekends for prospects to visit.
When she first toured the region before moving in 2015, Scovel and her husband, who had Parkinson’s, made sure to scope out the hospital, on a hill overlooking the sleepy town square. And she has rushed to the hospital four times since he died in 2017.
“I have very high blood pressure, and they’re able to do the IVs to get it down,” Scovel said. “This is an anxiety thing since my husband died. So now — I don’t know.”
She can’t in good conscience advise a senior with health problems to come join her in Celina, she said.
When Seconds Count, Delays In Care
Celina’s Cumberland River Hospital had been on life support for years, operated by the city-owned medical center an hour away in Cookeville, which decided in late January to cut its losses after trying to find a buyer. Cookeville Regional Medical Center executives explain that the facility faced the grim reality for many rural providers.
“Unfortunately, many rural hospitals across the country are having a difficult time and facing the same challenges, like declining reimbursements and lower patient volumes, that Cumberland River Hospital has experienced,” CEO Paul Korth said in a written statement.
Celina became the 11th rural hospital in Tennessee to close in recent years — more than in any state but Texas. Both states have refused to expand Medicaid in a way that covers more of the working poor. Even some Republicans now say the decision to not expand Medicaid has added to the struggles of rural health care providers.
The closest hospital is now 18 miles away. That adds another 30 minutes through mountain roads for those who need an X-ray or bloodwork. For those in the back of an ambulance, that bit of time could mean the difference between life or death.
“We have the capability of doing a lot of advanced life support, but we’re not a hospital,” said Natalie Boone, Clay County’s emergency management director.
The area is already limited in its ambulance service, with two of its four trucks out of service.
Once a crew is dispatched, Boone said, it’s committed to that call. Adding an hour to the turnaround time means someone else could likely call with an emergency and be told — essentially — to wait in line.
“What happens when you have that patient that doesn’t have that extra time?” Boone asked. “I can think of at least a minimum of two patients [in the last month] that did not have that time.”
Residents are bracing for cascading effects. Susan Bailey hasn’t retired yet, but she’s close. She has spent nearly 40 years as a registered nurse, including her early career at Cumberland River.
“People say, ‘You probably just need to move or find another place to go,'” she said.
Bailey and others are concerned that losing the hospital will soon mean losing the only three physicians in town. The doctors say they plan to keep their practices going, but for how long? And what about when they retire?
“That’s a big problem,” Bailey said. “The doctors aren’t going to want to come in and open an office and have to drive 20 or 30 minutes to see their patients every single day.”
Closure of the hospital means 147 nurses, aides and clerical staff have to find new jobs. Some employees come to tears at the prospect of having to find work outside the county and are deeply sad that their hometown is losing one of its largest employers — second only to the local school system.
Dr. John McMichen is an emergency physician who would travel to Celina to work weekends at the ER and give the local doctors a break.
“I thought of Celina as maybe the ‘Andy Griffith Show’ of healthcare,” he said.
McMichen, who also worked at the now-shutteredCopper Basin Medical Center, on the other side of the state, said people at Cumberland River knew just about anyone who would walk through the door. That’s why it was attractive to retirees.
“It reminded me of a time long ago that has seemingly passed. I can’t say that it will ever come back,” he said. “I have hopes that there’s still some hope for small hospitals in that type of community. But I think the chances are becoming less of those community hospitals surviving.”
“UNFORTUNATELY, RURAL HOSPITALS ACROSS THE COUNTRY ARE HAVING A DIFFICULT TIME AND FACE THE SAME CHALLENGES, LIKE DECLINING REIMBURSEMENTS AND LOWER PATIENT VOLUMES THAT CUMBERLAND RIVER HOSPITAL HAS EXPERIENCED.”
Facilities are faring better in states that expanded Medicaid, according to a new Commonwealth Fund report.
KEY TAKEAWAYS
A year after facing a federal funding cliff, CHCs in expansion states are thriving.
CHCs provide care to 27 million patients each year, according to the Health Resources and Services Administration.
The financial stability of CHCs, which serve medically vulnerable communities, is a benefit for health systems.
Community health centers (CHC) operating in states that expanded Medicaid under the ACA are 28% more likely to report improvements to their financial stability, according to a Commonwealth Fund report released Thursday morning.
CHCs in Medicaid expansion states reported were more likely to report improvements in their ability to provide affordable care to patients, 76%, than their counterparts in non-expansion states, 52%.
More than 60% of CHCs in expansion states reported improved ability to fund service or site expansions and upgrades for facilities, while only 46% of CHCs in non-expansion states said the same.
These facilities reported higher levels of unfilled job openings for mental health professional and social workers, while also implying a greater openness to operating under a value-based payment model.
The success and viability of CHCs are essential for larger health systems, according to Melinda K. Abrams, M.S., vice president and director of the Commonwealth Fund’s Health Care Delivery System Reform program, adding that CHCs act as a strong foundation for providing primary care to medically vulnerable populations in rural communities.
Abrams said that by making sure patients are insured and receiving care up front, rather than delaying treatment and exacerbating their condition, they are less likely to end up in a hospital emergency room and contribute to a rise in uncompensated care for hospitals.
She also told HealthLeaders that populations with higher enrollment rates make it easier for CHCs to innovate, invest in technology, hire new staff, train existing the workforce, and adopt new models of care.
“[Medicaid expansion] makes it a lot easier to provide high-quality comprehensive care when [a CHC’s] patients have health insurance,” Abrams said. “In this particular instance, it’s a lot easier to innovate and have financial stability when you have more paying patients, which means that it is easier if you are [a CHC] in a state that has expanded Medicaid.”
The Commonwealth Fund report provides a welcome note of positivity for CHCs, which serve vulnerable populations primarily composed by the uninsured, but have faced funding challenges in the past.
During the budget battles that produced multiple government shutdowns throughout the early portion of 2018, advocates wondered anxiously whether Congress would provide long term funding to the nearly 1,400 CHCs operating at nearly 12,000 service delivery sites across the country.
The Community Health Center Fund (CHCF), created in 2010 as a result of the ACA, is the largest source of comprehensive primary care for medically underserved communities, according to the Kaiser Family Foundation.
However, Abrams said that Medicaid expansion has also been a beneficial tool for CHCs, as they have begun to see more insured patients while also benefiting from Medicaid reimbursements, even though they are low compared to other reimbursement rates.
CHCs in states that expanded Medicaid have been able to grow the services that are offered while assisting in the ongoing fight against the opioid epidemic, according to the Commonwealth Fund report.
Abrams said that one downside to the growing success of CHCs have been the unfilled positions, mostly for mental health providers, that are falling behind rising demand levels, though she added that this finding is not surprising.
“I think it’s in part because the supply of the workforce is lagging a little bit behind the demand,” Abrams said. “There’s no reason to think that over time that this gap wouldn’t be closed. But we did find that as a challenge, that [CHCs] have a lot of positions open [yet] they’re hiring. A number of these CHCs are in economically depressed areas, so the good news is that there are some jobs available.”
CHCs are much more likely to participate in value-based payment models as a result of Medicaid expansion, with Abrams explaining that changes in payments and delivery models are common during insurance expansions.
She sees the continued progress made on the value-based front by CHCs as a way to “promote better healthcare and save money” over time.
Anyone interacting with the U.S. health care system is bound to encounter examples of unnecessary administrative complexity—from filling out duplicative intake forms to transferring medical records between providers to sorting out insurance bills. This administrative complexity, with its associated high costs, is often cited as one reason the United States spends double the amount per capita on health care compared with other high-income countries even though utilization rates are similar.1
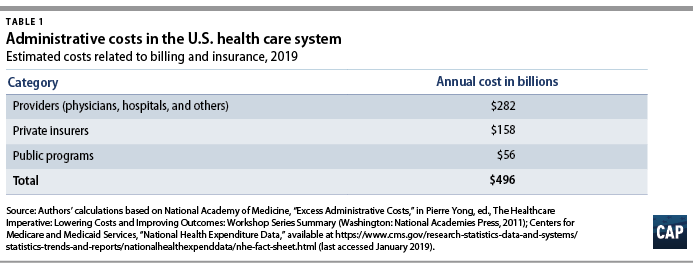
Each year, health care payers and providers in the United States spend about $496 billion on billing and insurance-related (BIR) costs, according to Center for American Progress estimates presented in this issue brief. As health care costs continue to rise, a logical starting point for potential savings is addressing waste. A 2010 report by the National Academy of Medicine (NAM) estimated that the United States spends about twice as much as necessary on BIR costs.2 That administrative excess currently amounts to $248 billion annually, according to CAP’s calculations.
This issue brief provides an overview of administrative expenditures in the U.S. health care system. It first explains the components of administrative costs and then presents estimates of the administrative costs borne by payers and providers. Finally, the issue brief describes how the United States can lower administrative costs through comprehensive reforms and incremental changes to its health care system. Many of the universal health care plans being discussed to expand coverage and lower costs would lower administrative costs through rate regulation, global budgeting, or simplifying the number of payers.3 Each of these financing changes deserves consideration—even in the absence of major systemwide reform.
Components of administrative costs
The main components of administrative costs in the U.S. health care system include BIR costs and hospital or physician practice administration.4 The first category, BIR costs, is part of the administrative overhead that is baked into consumers’ insurance premiums and providers’ reimbursements. It includes the overhead costs for the health insurance industry and providers’ costs for claims submission, claims reconciliation, and payment processing. The health care system also requires administration beyond BIR activities, including medical record-keeping; hospital management; initiatives that monitor and improve care quality; and programs to combat fraud and abuse.
To date, few studies have estimated the systemwide cost of health care administration extending beyond BIR activities. In a 2003 article in The New England Journal of Medicine, researchers Steffie Woolhandler, Terry Campbell, and David Himmelstein concluded that overall administrative costs in 1999 amounted to 31 percent of total health care expenditures or $294 billion5—roughly $569 billion today when adjusted for medical care inflation.6 A more recent paper by Woolhandler and Himmelstein, which looked at 2017 spending levels, placed the total cost of administration at $1.1 trillion.7
Billing and insurance-related costs
Many studies of administrative costs limit their scope to BIR costs. The BIR component of administration is most relevant to systemwide reforms that seek to reduce the expenses related to claims processing, billing rates, or health insurance. The largest share of BIR costs is attributable to insurance companies’ profits and overhead and to providers8where BIR costs include tasks such as record-keeping for claims submission and billing.
The costs associated with BIR administration can extend beyond the chief parties involved in receiving and submitting claims. The process of claims denials has become an industry unto itself, with private firms squeezing dollars out of Medicaid programs.9 One study estimated that the aggregate value of challenged claims ranges from $11 billion to $54 billion annually.10 Claims can also be manipulated to boost providers’ or insurers’ profits by recording services rendered in maximum detail and exaggerating the severity of patients’ conditions—a practice known as upcoding.11 Upcoding costs Medicare Advantage billions of dollars in excess expenditures,12 and in many cases the practice constitutes fraud.13
The NAM published one of the most thorough reports on U.S. administrative costs related to billing and insurance in 2010. In a synthesis of the literature on administrative costs, the NAM report concluded that BIR costs totaled $361 billion in 2009—about $466 billion in current dollars—among private insurers, public programs, and providers, amounting to 14.4 percent of U.S. health care spending at the time. The NAM estimated that BIR costs account for 13 percent of physician care spending; 8.5 percent of hospital care spending; 10 percent of spending on other providers; 12.3 percent of spending on private insurance; and 3.5 percent of public program spending, including Medicare and Medicaid.14
Applying the NAM’s percentages of BIR costs to recent projections of national health expenditures from the Centers for Medicare and Medicaid Services (CMS), CAP estimates that BIR costs will amount to $496 billion for 2019.15 (see Table 1) According to CAP’s calculations, this includes $158 billion in overhead for private insurance; $56 billion for administration of public insurance programs; and $282 billion for the BIR costs of hospitals, physicians, and other care providers. CAP’s estimate does not include the administrative costs associated with retail sales of medical products, including prescription drugs and durable medical equipment.
Even the most inclusive studies of administrative costs have not included at least one key piece of the U.S. health care system, namely, patients.16 The administrative complexity of the U.S. system also burdens patients, whether they are deciphering bewildering bills or shuttling records between providers. Three-quarters of consumers report being confused by medical bills and explanations of benefits.17 A Kaiser Family Foundation survey of people newly enrolled in the health insurance marketplace found that many were not confident in their understanding of the definitions of basic terms and concepts such as “premium,” “deductible,” or “provider network.”18 Insurers and employers spend an estimated $4.8 billion annually to assist consumers with low health insurance literacy, according to the consulting firm Accenture.19
Excess administrative costs
While U.S. administrative care spending is indisputably higher than that of other comparable countries, it’s unclear how much of the difference is excess and how much of that excess could be trimmed. The NAM report estimated that excess BIR costs amount to $190 billion—$245 billion in current dollars—or roughly half of total BIR expenditures in a year.20 The NAM report estimated that 66 percent of BIR costs for private insurers and 50 percent of BIR costs among providers are excess.21Based on these percentages, $248 billion of the total $496 billion BIR costs in CAP’s updated estimate are excess administrative costs.
Most studies that have attempted to identify excess costs in the American health care system rely on comparisons between the United States and Canada.22 In their 2010 review of the literature on the difference between the two countries’ health expenditures, economists Alexis Pozen and David M. Cutler looked at the sources of the gap between U.S. and Canadian health spending. They found that 62 percent of the difference between the two countries was attributable to prices and intensity of care, and 38 percent was linked to administrative costs.23Compared with Canada, the United States has 44 percent more administrative staff, and U.S. physicians dedicate about 50 percent more time on administrative tasks.24 Inflated to current dollars and today’s population, Pozen and Cutler’s estimate of per capita administrative excess in the United States, when compared with Canada, translates into a gap of $340 billion.25
Woolhandler and Himmelstein estimate that the United States currently spends $1.1 trillion on health care administration, and of that amount, $504 billion is excess.26Woolhandler and Himmelstein rely on surveys of physicians’ time use and utilized physician income data to translate the share of time physicians spend on administrative tasks into monetary value; their estimate of excess costs is the difference between U.S. and Canadian administrative spending27 Woolhandler and Himmelstein’s original 2003 article estimated that Canada spent $307 per capita on health system administration, compared with $1,059 per capita in the United States. Assuming this difference is excess requires an assumption that a Canadian-style health care system would achieve an identical level of administrative costs in the United States.
A separate criticism of the original 2003 Woolhandler and Himmelstein estimates, as articulated by Henry J. Aaron, an economist at the Brookings Institution, is that their methodology failed to account for differences in prices.28 Woolhandler and Himmelstein arrive at their national total administrative costs by tallying up costs in each country for items such as rent and salaries. As a consequence, the U.S.-Canada comparison captures not just the differences in the quantity of resources devoted to administration—such as physician time or office space—but also the differences in office rates, wages, and salaries. Taking Woolhandler and Himmelstein’s estimate of total administrative costs as a given and then making standard adjustments for price differences, Aaron argues that the two researchers exaggerated U.S. administrative spending in their 2003 report and that the true portion of excess would be about one-quarter less than what they estimated.
All estimates of administrative costs are inherently sensitive to what portion of health care spending one considers administrative.29 For example, time spent recording diagnosis or prescription information used in billing may also be vital for patient care, allowing medical teams to share up-to-date information or avoid harmful drug interactions. A recent study of an electronic health records (EHR) system estimated that on average, half of a primary care physician’s day is spent on EHR interaction, including billing, coding, ordering, and communication.30 Such tasks, however, can fall into a gray area between administrative and clinical. In a separate study, economist Julie Sakowski and her fellow researchers reported finding varying attitudes among physicians about whether interaction with electronic medical records—a subset of EHR—represented administrative or clinical time. As Sakowski and co-authors wrote, “Some felt they spent extra effort adding documentation that was needed only for billing. Others seemed to feel that nearly all of that information was needed for accurate clinical records.”31
Administrative costs for payers
Within the U.S. system, the share of expenditures that are attributable to administrative costs varies greatly by payer. The BIR costs for traditional Medicare and Medicaid hover around 2 percent to 5 percent, while those for private insurance is about 17 percent.32Some public finance experts, including Robert Book, have argued that the low levels of Medicare overhead are deceptive. Because seniors have relatively high health expenditures, the argument goes, administrative costs make up a relatively small share of their total health care spending. However, Medicare’s per capita administrative expenditures are higher than those in other forms of insurance.33 Even if one compares higher-end estimates of Medicare administrative costs to low-end estimates of costs for private insurance, the gulf between administrative costs for Medicare and private coverage is large.34 Organisation for Economic Co-operation and Development (OECD) data also show that other nations are able to achieve low levels of administrative costs while maintaining universal coverage across all ages of the population.35
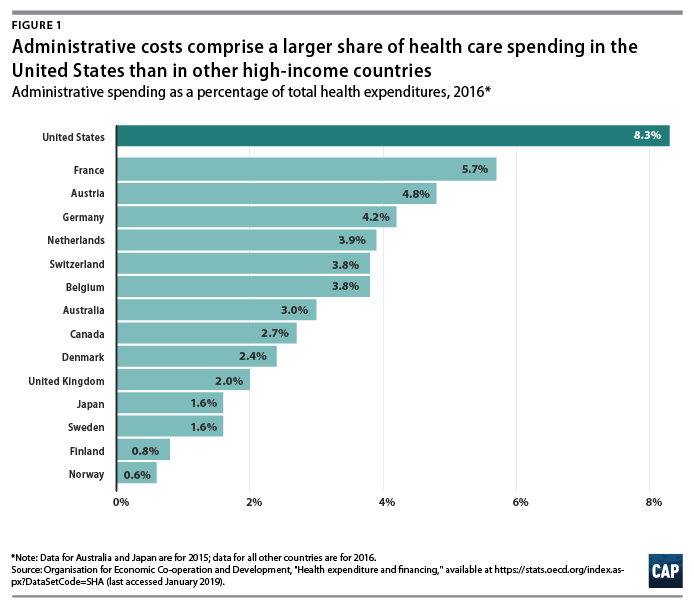
International health system data demonstrate that the United States is a clear outlier on administrative spending. And while the OECD’s definition includes administrative costs to government, public insurance funds, and private insurance, but not those borne by hospitals, physicians, and other providers, the stark difference is still informative. In 2016, administration accounted for 8.3 percent of total health care expenditures in the United States—the largest share among comparable nations. (see Figure 1) Countries with single-payer systems are among those with the lowest administrative costs. For example, administrative spending accounts for just 2.7 percent of total health care expenditures in Canada.36 OECD data also show that within a country, administrative costs are higher in private insurance than in government-run programs.37
Countries that have multipayer systems with stricter rate regulation also achieve much lower administrative costs than the United States. Administrative expenditures account for 4.8 percent of total health care expenditures in Germany, 3.9 percent in the Netherlands, 3.8 percent in Switzerland, and 1.6 percent in Japan, according to the OECD. If the United States could reduce administrative costs down to Canadian levels, it would save 68 percent of current administrative expenditures; reducing to German-level administrative costs would save 42 percent of current administrative expenditures. However, to assume that by simply adapting another country’s health care system—whether it is Canada’s single-payer Medicare, Germany’s sickness funds, or Switzerland’s heavily regulated private plans—the United States would automatically achieve the same level of administrative costs may ignore other fundamental differences between countries, including the market power of health care providers, political systems, and attitudes toward health care. Nevertheless, the experience of other multipayer systems such as those in Germany and Switzerland suggests that the United States could substantially reduce both administrative expenditures and overall health care spending by bringing down reimbursement rates and regulating insurance—even while continuing to allow multiple payers and private health care providers.
The lowest possible level of administrative spending for the U.S. health care system is not necessarily the optimal level of spending. As researchers Robert A. Berenson and Bryan E. Dowd have noted, administrative spending in Medicare may in fact be too low; the program would be more efficient with greater investment in initiatives to lower costs and improve quality.38 Many reforms that could generate overall savings require administrative resources to design and implement. Innovations such as bundled payments—the practice of paying providers a lump sum for an episode of care such as a knee replacement or childbirth rather than reimbursing each individual component—involve upfront investment in development. Increasing resources to combat fraud and abuse would also lower overall spending. While the U.S. Department of Health and Human Services (HHS) boasts that it sees a $5 return on every $1 it puts toward fraud and abuse investigations, that number indicates that the government may be underinvesting in those efforts.39
Administrative costs for health care providers
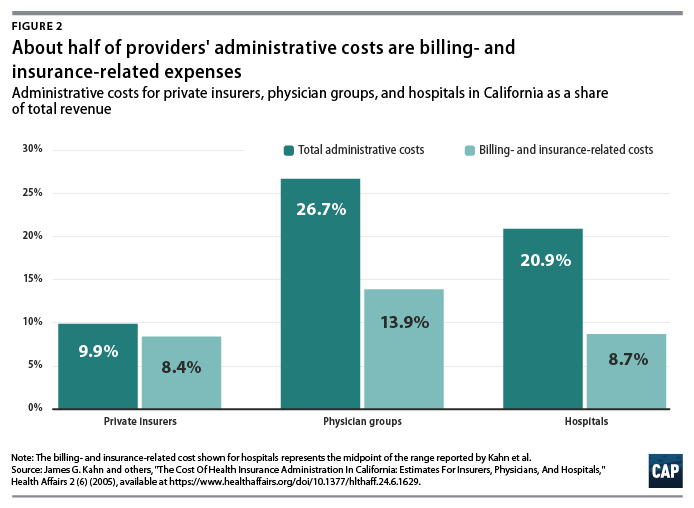
A number of studies have focused on the administrative costs borne by providers. Beyond BIR expenses, hospitals, physician practices, and other health care institutions house departments that are complementary to clinical services such as medical libraries, public relations, and accounting.40 A study of administrative costs in California found that administrative costs represented about one-quarter of physician revenue and one-fifth of hospital revenue, and BIR costs accounted for roughly half of administrative expenditures for physician and hospital services covered by private insurance.41 (see Figure 2) In a separate study, Himmelstein and others reported that one-quarter of U.S. hospital spending went toward administration; they found little difference between nonprofit hospitals and for-profit institutions, where administrative spending was 25 percent and 27.2 percent of total spending, respectively.42
On a per-encounter basis, BIR costs vary as a proportion of overall cost depending on the type of visit. In a 2018 study of an academic health care system, Phillip Tseng and others found that professional billing costs amounted to $20.49 for a primary care visit, $61.54 for an emergency department visit, and $124.26 for a general inpatient stay.43 Relative to the professional revenue associated with each encounter studied, the emergency department visit ranked the highest, with billing costs equal to 25.2 percent of revenue. Inpatient visits were the lowest, at 8 percent of a general inpatient stay and 3.1 percent for inpatient surgery.44 Encounters involving hospital care incurred additional facility-level billing costs. (see Figure 3)
In addition to the dollar cost of BIR activity, the study also reported the time spent on administration for typical encounters. The average processing time was 13 minutes for a primary care visit, 32 minutes for an emergency department visit, and 73 minutes for a general inpatient stay.45
Among other research on provider BIR costs, a 2009 study by Larry Casalino and others estimated that the cost of the time physicians spend on interactions with health plans is about $23 billion to $31 billion per year.46 A 2011 study by Dante Morra of the University of Toronto and others estimated that interaction with payers costs the equivalent of $22,205 per physician annually in Canada and $82,975 per physician annually in the United States, suggesting that the United States would save $27.6 billion annually if U.S. administrative costs could be brought down to Canadian levels.47
As with BIR costs, provider administrative costs in the United States are higher than those in other comparable countries. Hospital administrative costs in the United States far exceed those of other nations. In their comparison of hospital administrative costs among eight Western nations, Himmelstein and co-authors found that the United States had the highest levels, at 25.3 percent of total hospital expenditures.48 They conclude that in nations where hospital administrators have minimal responsibilities for procuring financing and where the hospital reimbursement system is least complex, administrative costs can be reduced to 12 percent of expenditures.49 These findings suggest that reforms that introduce global budgeting or limit the need to bargain with multiple payers could potentially bring down excess hospital administrative costs in the United States.
Lower administrative costs in single-payer and multipayer systems
Although administrative costs contribute to the high expenditures in the United States, they are not the primary reason for the health care spending gap. As economist Uwe Reinhardt and others candidly put it, “It’s the prices, stupid.”50 The United States pays more for care than other countries do—both for administrative services and for other components of health care.
Policies that target administrative costs alone would not necessarily bring overall U.S. health care expenditures in line with other countries. As economists Sherry Glied and Adam Sacarny observed, “there are very substantial variations in administrative costs among countries with universal health insurance, which do not translate directly into variations in overall costs.”51Comparative evidence from U.S. states also suggests that America’s multipayer system explains some, but by no means all, of the discrepancy between the United States and other developed nations. Harvard University researchers Joseph P. Newhouse and Anna Sinaiko observe that “there is considerable variation across the states in spending levels, with the lowest quintile of states spending approximately the same percentage as the higher spending OECD countries other than the U.S. This implies that the [United States’] pluralistic financing system may not be an important cause of the large percentage of GDP that the U.S. devotes to health care.”52
Systemwide reforms to lower administrative costs
Health care financing experts believe that changes to how Americans pay for coverage could dramatically reduce administrative costs. Researchers simulating the effects of single-payer programs have assumed that administrative costs would be brought down substantially. The Urban Institute set administrative costs at a “plausible” 6 percent of health care claims for their simulation of the single-payer plan proposed by Sen. Bernie Sanders (I-VT), noting that they “do not believe that administrative costs can fall far below this level; far too many administrative functions must be conducted.”53 In its analysis of a single-payer system for New York state, the RAND Corporation assumed administrative costs at 6 percent of total health expenditures in its base case, representing a reduction from 18 percent among commercial insurers and 7 percent in New York’s Medicaid program. RAND specified administrative costs at 13 percent and 3 percent in its alternative scenarios. 54 In a separate column, however, RAND researcher Jodi Liu cautioned that achieving the administrative expenditure levels of other countries “may be aspirational and is not guaranteed” under a single-payer system.55
Exactly how such lower costs could be achieved is another question. Reducing BIR costs requires simplifying the billing and payment process, which could be accomplished in a number of ways. Two avenues for reducing administrative costs as well as overall health costs are global budgeting and uniform rate-setting.56 These two concepts are central to health systems around the world and are also responsible for keeping administrative costs lower, whether a country has a multipayer or single-payer system. Another paperwork-reducing option would be a centralized claims clearinghouse to allow providers to submit all claims to a single entity, as they do in Germany and Japan. 57
All-payer rates and global budgeting
Setting all-payer reimbursement rates would eliminate the need for providers to negotiate rates with individual private insurers, while also giving policymakers better leverage for controlling overall health care cost growth. In the current U.S. system, providers charge different rates to different payers, and the billing process is complicated and opaque. The list prices that hospitals are now required to publish bear little connection to what individual patients—or those patients’ insurers—actually pay.58 Setting all-payer rates would simplify billing and improve transparency by establishing a single set of rates for each provider, while also giving regulators a tool to protect consumers from exorbitant rates.59
Global budgeting—the practice of paying providers revenue based on their expected costs—also holds promise for both lowering administrative spending and overall costs. As opposed to traditional fee-for-service payments, which reward providers for doing more, global budgeting incentivizes providers to deliver care more efficiently.60 Global budgeting is a feature of many countries with much lower health care administrative costs, including Scotland, Wales, and Germany.61 As Woolhandler, Campbell, and Himmelstein point out in their 2003 article, “The existence of global budgets in Canada has eliminated most billing and minimized internal cost accounting, since charges do not need to be attributed to individual patients and insurers.”62 As Germany shows, both single-payer and multipayer systems can use global budgets.
A system combining all-payer rates and global budgeting is already partially in place in the state of Maryland, where each hospital has a single set of rates it bills to Medicare, Medicaid, commercial insurers, and other payers. Maryland’s system is keeping overall cost growth lower than the national trend.63 According to RAND analysis of hospital costs, Maryland hospitals have administrative costs that are 9 percent lower than the national average and not far off from the 13 percent savings RAND assumed providers would achieve under a single-payer system. 64
Centralized claims processing
Germany and Japan both have multiple payers but centralized claims processing.65Despite having more than 3,000 health plans,66 Japan’s administrative expenditures were a stunningly low 1.6 percent of overall health care costs in 2015, one of the lowest among OECD member nations.67
In their analysis of three universal health care options for Vermont, including single payer, researchers William C. Hsiao, Steven Kappel, and Jonathan Gruber estimated substantial savings from administrative simplicity from each option. The two single-payer options they examined would result in even greater administrative savings of between 7.3 percent and 7.8 percent, depending on the rate-setting mechanism.68 The group estimated that a third scenario, which would establish a centralized claims clearinghouse while allowing multiple payers, could generate savings equal to 3.6 percent of total expenditures.69This suggests that about half of the total administrative savings from a single-payer system could be obtained within a regulated multipayer system.
Policy proposals directed at administrative costs
While major changes to the U.S. health care system have the greatest potential to bring down costs, more incremental changes could reduce administrative waste. A recent bill proposed by Sens. Bill Cassidy (R-LA) and Tina Smith (D-MN) would direct the HHS secretary to set goals to cut “unnecessary costs and administrative burdens” throughout the health care system by 50 percent over the next 10 years. It would also provide grant money for state-based efforts to bring down administrative costs.70Some possible avenues for achieving those kinds of reductions include changes to payment rules, improvements to facilitate electronic record-keeping and information exchange, and simplification of public insurance programs.
In their 2009 article in TheNew England Journal of Medicine, David Cutler, Elizabeth Wikler, and Peter Basch proposed one such package of reforms. The authors estimated that providers could save $17.9 billion to $23 billion annually with several, more incremental changes to the system, including greater adoption of EHR systems; integrated administrative and clinical systems; national and standardized reporting requirements and credentialing of providers; streamlined enrollment in public insurance programs; and greater automation.71 In a separate report, the same authors proposed additional reforms that they estimated could reduce excess administrative costs by $40 billion, or 25 percent of total health care expenditures.72
In a 2010 study published in Health Affairs, Bonnie B. Blanchfield and other Massachusetts researchers concluded that the administrative burden on physician organizations could be reduced by a “single transparent set of payment rules for a system with multiple payers.” The authors recommended that the United States adopt “a standard set of payment requirements, increased payment-rule transparency, standardized forms, and a standard set of data exchange requirements.” Doing so could save $7 billion in billing costs for physician and other clinical services, according to the authors’ estimates.73
Conclusion
Although estimates vary, a large body of evidence shows that the United States is spending about twice as much as needed on the administration of health care. Other nations enjoy world-class health care systems while spending a fraction of what the United States does on governance, billing, and insurance.
A structural overhaul of how health care is financed and priced that includes key features of other countries’ systems—whether one payer or many—would go a long way toward eliminating excess administrative costs. Simplifying the payment system should be an essential part of future health reform and would make the U.S. system work better for taxpayers and patients alike.
Medicare Advantage (MA) plans got a better-than-anticipated pay hike this week, as the Centers for Medicare & Medicaid Services (CMS) released its final 2020 policy and payment updates for the private coverage program for seniors. MA payments will increase by an average of 2.53 percent in 2020, higher than the 1.59 percent initially proposed by CMS earlier this year, reflecting CMS’s expectation that MA services will grow faster than it initially thought.
With the announcement, CMS is also finalizing plans to allow reimbursement for supplemental, non-clinical services covered by MA plans, such as transportation, nutrition support, and housing improvements, as long as those services are intended to improve health status. The final update also confirms CMS’s intent to continue updating its risk-adjustment methodology to more accurately reflect the intensity of services delivered to beneficiaries, a change that has been controversial among insurers, who fear the new methodology will result in lower payments from the government.
Despite these concerns, shares of MA insurers traded higher after the CMS announcement, and health plans will no doubt be pleased with yet another year of good news from CMS on MA rates. Given continued strong enrollment growth, robust rate increases, and a pipeline of millions of aging Baby Boomers poised to become eligible for Medicare, large insurers (and increasingly, providers) will view MA as their primary source of growth for the next decade or more.
Reversing course in the face of strong pushback from his own party’s leaders in Congress, President Trump this week backed off his earlier pledge to deliver a Republican healthcare plan to replace the Affordable Care Act (ACA).
After the Department of Justice switched positions on the Texas court case testing the constitutionality of the ACA, urging the Fifth Circuit Court of Appeals to invalidate the 2010 law entirely, Trump doubled down by declaring that Republicans would be known as the “party of healthcare”, going so far as to tap four GOP senators to craft a replacement bill.
However, the White House received a rare rebuke from Senate Majority Leader Mitch McConnell (R-KY), who said this week that in private discussions with the President, “I made it clear to him that we’re not going to be doing that in the Senate.” In tweets and a subsequent speech, Trump signaled his frustration with Congressional Republicans on the issue (“We blew it the last time. Man, I was fed a bill of goods.”), vowing to return to the issue after the 2020 elections.
By highlighting GOP divisions on the issue, this week’s public dust-up and Presidential about-face all but guarantee that healthcare will be a marquee issue in the upcoming elections, allowing Democrats to campaign on an issue that proved a strong suit for them in the 2018 midterms. Expect the politics of healthcare to remain front and center in the months to come.
Hospitals, physicians and insurer groups are united in wanting to preserve the Affordable Care Act and have defended it in briefs filed with the Fifth Circuit Court of Appeals.
On the other side is the Department of Justice, which last month reversed an earlier opinion and sided with the Texas judge who ruled that without the individual mandate, the entire ACA has no constitutional standing.
WHY THIS MATTERS
The ACA has insured millions who otherwise may not have been insured, allowing them to get care when needed instead of going to the more expensive emergency room when they have a medical crisis.
Hospitals and physicians see less uncompensated care under the ACA.
Without the ACA, patients would no longer have protections for pre-existing conditions, children would no longer have coverage under their parents’ health insurance plan until age 26, insurers would no longer be held to the 85 percent medical loss ratio, 100 percent coverage for certain preventive services would cease and individual marketplace and subsidies based on income would be eliminated.
Also, federal funding for Medicaid expansion would end.
TREND
Republicans under President Trump have tried unsuccessfully to repeal and replace the law.
The lawsuit, brought by 19 Republican governors, puts the GOP in a political bind over supporting the repeal of a law that is popular with consumers and their constituents. President Donald Trump recently said Republicans would unveil an ACA replacement after the 2020 election.
Democrats are also facing a crisis within their party over healthcare as it becomes a priority issue in the presidential election. Some of the leading candidates, such as Senator Kamala Harris, support Medicare for all. The Medicare for All Act of 2019 has been introduced in the Democratic-led House of Representatives.
Veteran politician and attorney Earl Pomeroy said he believes the Texas versus United States appeal changes the political course for 2020. The entire MFA argument will move to the back burner because of the Texas lawsuit, he said.
“The fight is going to be trying to underscore the Congressional importance of the provisions of the ACA and enhancing them,” Pomeroy said. “I do not believe that supporting Medicare for all is an advantageous position for a Democratic candidate running in a district that is not a secure Democratic seat. I believe Kamala Harris will spend much of the campaign walking back her comments on health insurance.”
Pomeroy is a former member of the U.S. House of Representatives for North Dakota’s at-large district, a North Dakota Insurance Commissioner and senior counsel in the health policy group with Alston & Bird.
“The safe political ground is defending a law people have warmed up to,” he said. “All politics is local but all healthcare is personal. There is little risk tolerance in the middle class for bold experiments in healthcare.”
BACKGROUND
The lawsuit was brought by Texas and the 19 other Republican-led states, based on the end of the individual mandate. In February, U.S. District Court Judge Reed O’Connor agreed that the federal law cannot stand without the individual mandate because if there is no penalty for not signing up for coverage, then the rest of the law is unconstitutional.
Twenty-one Democratic attorneys general appealed and the House of Representatives has intervened to defend the ACA in the case.
Either outcome in the appeals court may see the case headed to the U.S. Supreme Court.
WHAT THE PROVIDERS AND INSURERS ARE TELLING THE COURT
In a court brief filed by the AHA, the Federation of American Hospitals, The Catholic Health Association of the United States, America’s Essential Hospitals, and the Association of American Medical Colleges urged the Fifth Circuit Court of Appeals to reject a district court decision they said would have a harmful impact on the American healthcare system.
“Those without insurance coverage forgo basic medical care, making their condition more difficult to treat when they do seek care. This not only hurts patients; it has severe consequences for the hospitals that provide them care. Hospitals will bear a greater uncompensated-care burden, which will force them to reallocate limited resources and compromise their ability to provide needed services,” they said.
In a separate friend-of-the-court brief, 24 state hospital associations also urged the Fifth Circuit to reverse, highlighting specific innovative programs and initiatives for more coordinated care.
The American Medical Association, the American College of Physicians, American Academy of Family Physicians, American Academy of Pediatrics and the American Psychiatric Association filed a brief. AMA President Dr. Barbara L. McAneny said, “The district court ruling that the individual mandate is unconstitutional and inseverable from the remainder of the ACA would wreak havoc on the entire healthcare system, destabilize health insurance coverage, and roll back federal health policy to 2009. The ACA has dramatically boosted insurance coverage, and key provisions of the law enjoy widespread public support.”
AHIP said the law impacts not only the individual and group markets, but also other programs such as Medicaid, Medicare and Part D coverage.
“Since its passage in 2010, the ACA has transformed the nation’s healthcare system,” AHIP said. “It has restructured the individual and group markets for purchasing private health care coverage, expanded Medicaid, and reformed Medicare. Health insurance providers (like AHIP’s members) have invested immense resources into adjusting their business models, developing new lines of business, and building products to implement and comply with those reforms.”
More than three in four Americans expect healthcare costs to increase over the next few years and result in “significant and lasting damage” to the U.S. economy, according to a survey by nonprofit West Health and Gallup. And 69%were “not at all” confident policymakers will fix the situation.
Given the choice between a 10% increase in income or a complete five year freeze of healthcare costs, 61% of people said they’d choose the latter, in line with the almost half of Americans concerned that a major health event would lead to bankruptcy for their family. In the past year alone, 12% have borrowed money to pay for care and 10% had foregone treatment due to cost.
However, although just 39% of those surveyed were pleased with the U.S. healthcare system as a whole, 64% were satisfied in how it worked for their households. Roughly half believe the quality of U.S. healthcare is either the “best in the world” or “among the best.”
Dive Insight:
Frustrations faced by Americans in paying for healthcare are understandable given that the U.S. ranks first among the 36 OECD developed nations in healthcare cost per person.
But their belief in the supremacy of the U.S. healthcare system is misplaced at best.
The U.S. ranks 31st among the OECD group in terms of infant mortality, a key indicator of overall quality, and a depressing 28th in overall life expectancy.
While healthcare is more regulated in nearly every other developed country,mammoth bills pack a bigger punch because they can come out of nowhere in the U.S. Some 47% of Americans reported never knowing what a visit to the emergency room will cost before receiving care. Just 19% of respondents said they “always” knew their out-of-pocket costs before visiting the ER.
Outpatient surgery, visits to a physical therapist or chiropractor, and check-ups and physicals didn’t fare much better, with only 17%, 23% and 39% of respondents respectively saying they always knew their out-of-pocket costs at those sites of care.
Obfuscation of prices may lead to “risky and unhealthy behavior,” according to the West Health report. It found 41% of Americans surveyed reported forgoing a visit to the ER over the past year due to cost concerns.
And this fear over costs is affecting people at every rung of the socioeconomic ladder. West Health and Gallup found the concern wasn’t just unique to people struggling financially — it was consistent up to the top 10% of earners.
“Angst is a very appropriate word to use when you see the data,” Mike Ellrich, healthcare portfolio leader at Gallup said at the West Health Healthcare Costs Innovation Summit on Tuesday.
Political debate over fixing this problem has centered of late on drug prices, surprise medical bills, pre-existing conditions and lowering insurance premiums, which are rising faster than income. And CMS has prodded providers and payers to make out-of-pocket costs more transparent for patients.
But Americans largely don’t think politicians will be able to fix the problem, with more than two-thirds of Republicans and Democrats alike not at all confident that elected officials will be able to achieve bipartisan legislation to lower costs.
However, perceptions of quality diverged among party lines. West Health and Gallup found 67% of Republicans view the U.S. healthcare system as delivering the best or among the best care in the world. Just 38% of Democrats agreed.
“I’m all for patriotism, but this is a disconnect from reality,” Ellrich said. “This issue is not red or blue.”
The ceaseless battle over the 2010 law has made it difficult to address the high cost of American health care.
The Obamacare wars have ignored what really drives American anxiety about health care: Medical costs are decimating family budgets and turning the U.S. health system into a runaway $3.7 trillion behemoth.
Poll after poll shows that cost is the number one issue in health care for American voters, but to a large extent, both parties are still mired in partisan battles over other aspects of Obamacare – most notably how to protect people with pre-existing conditions and how to make insurance more affordable, particularly for people who buy coverage on their own.
That leaves American health care consumers with high premiums, big deductibles and skyrocketing out-of-pocket costs for drugs and other services. Neither party has a long-term solution — and the renewed fight over Obamacare that burst out over the past 10 days has made compromise even more elusive.
Democrats want to improve the 2010 health law, with more subsidies that shift costs to the taxpayer. Republicans are creating lower-cost alternatives to Obamacare, which means shifting costs to older and sicker people.
Neither approach gets at the underlying problem — reducing costs for both ordinary people and the health care burden on the overall U.S. economy.
Senate HELP Committee chair Lamar Alexander, the retiring Tennessee Republican with a reputation for deal-making, has reached out to think tanks and health care professionals in an attempt to refocus the debate, saying the interminable fights about the Affordable Care Act have “put the spotlight in the wrong place.”
“The hard truth is that we will never get the cost of health insurance down until we get the cost of health care down,” Alexander wrote, soliciting advice for a comprehensive effort on costs he wants to start by summer.
But given the partisanship around health care — and the fact there have been so many similar outreaches over the years for ideas, white papers and commissions — it’s hard to detect momentum. Truly figuring how to fix anything as vast, complex and politically charged as health care is difficult. Any serious effort will create winners and losers, some of whom are well-protected by powerful K Street lobbies.
And the health care spending conversation itself gets muddled. People’s actual health care bills aren’t always top of mind in Washington.
“Congress is looking at federal budgets. Experts are looking at national health spending and the GDP and value. And the American people look at their own out-of-pocket health care costs and the impact it has on family budgets,” said Drew Altman, the president and CEO of the Kaiser Family Foundation, which extensively tracks public attitudes on health.
But Congress tends to tinker around the edges — and feud over Obamacare.
“We’re doing nothing. Nothing. We’re heading toward the waterfall,” said former CBO director Doug Elmendorf, now the dean of the Harvard Kennedy School, who sees the political warfare over the ACA as a “lost decade,” given the high stakes for the nation’s economic health.
The solutions championed by the experts — a mix of pricing policies, addressing America’s changing demographics, delivering care more efficiently, creating the right incentives for people to use the right care and the smarter use of high-cost new technologies — are different than what the public would prescribe. The most recent POLITICO-Harvard T.H. Chan School of Public Health poll found the public basically wants lower prices, but not a lot of changes to how — or how much — they consume health care, other than spending more on prevention.
Lawmakers are looking at how to start chipping away at high drug prices, or fix “surprise” medical bills that hit insured people who end up with an out-of-network doctor even when they’re at an in-network hospital. Neither effort is insignificant,and both are bipartisan. While those steps would help lower Americans’ medical bills, health economists say they won’t do enough to reverse the overall spending trajectory.
Drug costs and surprise bills, which patients have to pay directly, “have been a way the public glimpses true health care costs,” said Melinda Buntin, chair of the Department of Health Policy at Vanderbilt University School of Medicine. “That information about how high these bills and these charges can be has raised awareness of health care costs — but it has people focused only on that part of the solution.”
And given that President Donald Trump has put Obamacare back in the headlines, the health law will keep sucking up an outsized share of Washington’s oxygen until and quite likely beyond the 2020 elections.
Just in the last week, the Justice Department urged the courts to throw out Obamacare entirely, two courts separately tossed key administration policies on Medicaid and small business health plans, and Trump himself declared he wants the GOP to be the “party of health care.” Facing renewed political pressure over the party’s missing Obamacare replacement plan, Trump last week promised Republicans would devise a grand plan to fix it. He backtracked days later and said it would be part of his second-term agenda.
Democrats say Trump’s ongoing assaults on the ACA makes it harder to address the big picture questions of cost, value and quality. “That’s unfortunately our state of play right now,” said Rep. Raul Ruiz (D-Calif.). “Basic health care needs are being attacked and threatened to be taken away, so we have to defend that.”
The ACA isn’t exactly popular; more than half the country now has a favorable view of it, but it’s still divisive. But for Republicans and Democrats alike, the new POLITICO-Harvard poll found the focus was squarely on health care prices — the cost of drugs, insurance, hospitals and doctors, in that order.
The Republicans’ big ideas have been to encourage less expensive health insurance plans, which are cheaper because they don’t include the comprehensive benefits under Obamacare. That may or may not be a good idea for the young and healthy, but it undoubtedly shifts the costs to the older and sicker. The GOP has also supported spending hundreds of millions less each year on Medicaid, which serves low-income people — but if the federal government pays less, state governments, hospitals and families will pay more.
Last week, courts blocked rules in two states that required many Medicaid enrollees to work in order to keep their health benefits, and also nixed Trump’s expansion of association health plans, which let trade groups and businesses offer coverage that doesn’t include all the benefits required under the ACA.
House Democrats last week introduced a package of bills that would boost subsidies in the Obamacare markets and extend that financial assistance to more middle-class people. The legislation would also help states stabilize their insurance markets — something that the Trump administration has also helped some states do through programs backstopping health insurers’ large costs.
These ideas may also bring down some people’s out-of-pocket costs, which indirectly lets taxpayers pick up the tab. These steps aren’t meaningless — more people would be covered and stronger Obamacare markets would stabilize premiums — but they aren’t an overall fix.
The progressive wing of the Democratic party backs “Medicare for All,” a brand new health care system that would cover everyone for free,including long-term care for elderly or disabled people. Backers say that the administrative simplicity, fairness, and elimination of the private for-profit insurance industry would pay for much of it.
The idea has moved rapidly from pipe dream to mainstream, but big questions remain even among some sympathetic Democrats about financing and some of the economic assumptions, including about how much of a role private insurance plays in Medicare today, and how much Medicare puts some of its costs onto other payers. Already a political stretch, the idea would face a lot more economic vetting, too.
The experts, as well as a smattering of politicians, define the health cost crisis more broadly: what the country spends. Health care inflation has moderated in recent years; backers of the Affordable Care Act say the law has contributed to that. But health spending is still growing faster than the overall economy. CMS actuaries said this winter that if current trends continue, national health expenditures would approach nearly $6 trillion by 2027 — and health care’s share of GDP would go from 17.9 percent in 2017 to 19.4 percent by 2027. There aren’t a lot of health economists who’d call that sustainable.
And ironically, the big fixes favored by the health policy experts — the ones that Alexander is collecting but most politicians are ignoring — might address many of the problems that keep aggravating U.S. politics. If there were rational prices that reflected the actual value of care provided for specific episodes of illness and treatment, instead of the fragmented system that largely pays for each service provided to patients, then no medical bill would be a surprise, noted Mark McClellan, who was both FDA and CMS chief under the President George W. Bush and now runs the Duke-Margolis Center for Health Policy.
“But taking those steps take time and will be challenging,” McClellan noted. “And they’ll be resisted by a lot of entrenched forces.”
The only plausible explanation for President Trump’s renewed effort through the courts to do away with the Affordable Care Act, other than muscle memory, is a desire to play to his base despite widely reported misgivings in his own administration and among Republicans in Congress.
Reality check: But the Republican base has more complicated views about the ACA than the activists who show up at rallies and cheer when the president talks about repealing the law. The polling is clear: Republicans don’t like the ACA, but just like everyone else, they like its benefits and will not want to lose them.
The big picture: About three quarters of Republicans still have an unfavorable view of the ACA, and seven in 10 say repealing the law is a top health priority for Congress — higher than other priorities such as dealing with prescription drug costs. And yes, 7 in 10 Republicans still want to see the Supreme Court overturn the law.
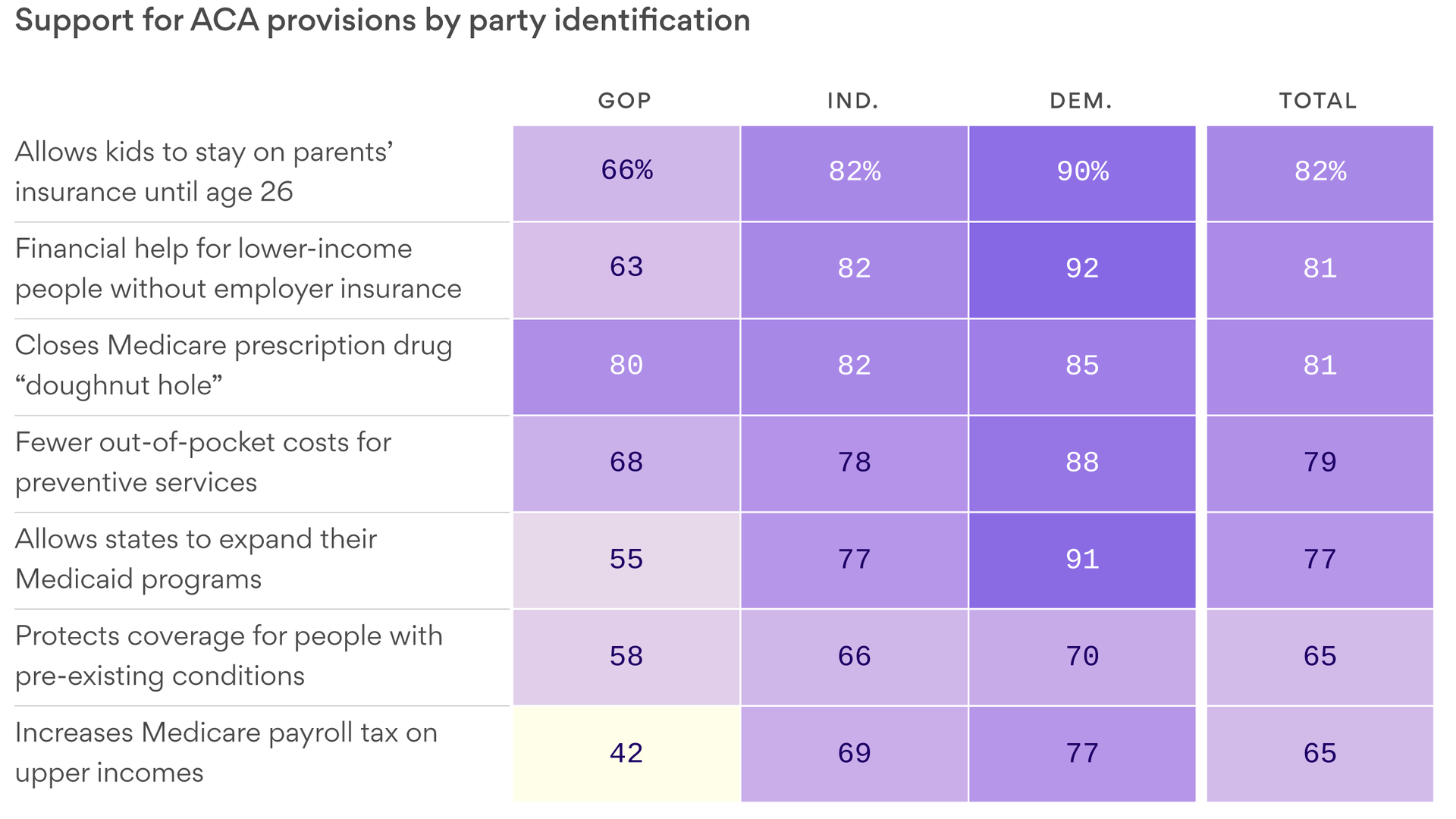
But as the chart shows, majorities of Republicans like many elements of the ACA —especially closing the “donut hole” in Medicare prescription drug coverage (80%), eliminating copayments for preventive services (68%), keeping young adults under 26 on their parents’ plans (66%) and subsidies for low and middle-income households (63%).
Nearly half of Republicans want the Supreme Court to keep the protections for pre-existing conditions (49%), and even more show general support for the pre-existing conditions protections (58%).
During the repeal and replace debate in 2017, even Republicans were nervous to hear that these sorts of things would go away. The 2020 campaign would drive home to the public, and to Republicans, what they have to lose — and it would become especially real to them if the 5th Circuit Court of Appeals upholds the ruling striking down the ACA.
Maybe Republicans would forget about these lost benefits if they could agree on a replacement plan they liked? But there isn’t one, and many of the ideas thought to be elements of one — such as cutting and block granting both Medicaid and ACA subsidies — are non-starters with Democrats and moderate Republicans on Capitol Hill. They’re unpopular with the public, too.
The bottom line: It is widely accepted that a renewed debate about repeal hands Democrats a powerful new political opportunity. Deeper in the polling, it’s also clear that’s it’s more of a mixed bag for Republicans than President Trump may realize.