http://www.healthcaredive.com/news/healthcare-workforce-growth-cuts/446182/

Employment in the healthcare industry has risen since the ACA was passed, but many health systems have been trimming their workforce under financial pressure.
It’s clear there have been a fair amount of hospital and provider layoffs in 2017.
In the past few months, hospitals of all sizes, and in all parts of the country, have said they are cutting jobs or eliminating open positions. Major providers affected have included Memorial Hermann, Brigham and Women’s Hospital, NYC Health + Hospitals, Summa Health and Hallmark Health. In May, Becker’s Hospital Review listed 48 layoffs across the industry the publication had reported on in 2017.
The layoffs come in contrast with the sharp rise in hiring in the healthcare sector ever since the Affordable Care Act (ACA) was enacted. While the hiring growth is a long-term trend — though it’s yet to be determined at what rate in 2017 — these layoffs are due in part to the short-term trends of softening admissions and flattening reimbursements. Many providers cited similar problems: declining reimbursements, lower admissions and shrinking operating incomes. Layoffs aren’t the only play for struggling organizations, but hospital expenses are rising on multiple fronts, and executives have to make some hard choices.
Big drivers of the growth are the aging population and the pending retirement of many registered nurses. It’s unclear how or when the layoff and healthcare job growth trends will change, but the underlying themes are not going away. The Bureau of Labor Statistics (BLS) is scheduled to release 2016-2026 occupational projections in October, while layoffs will continue to be tracked throughout the year.
Then there’s the elephant in the room over the buzzword of 2017: Uncertainty. Whether it be in Congress or in the executive branch, uncertainty over U.S. healthcare policy is making providers nervous as the insurance open enrollment period nears with no clear ACA reform or repeal in sight.
Healthcare hiring still on the rise, but the pace may be slowing
To date, the healthcare employment bubble hasn’t burst. Healthcare jobs, including hospital jobs, still are on the rise. While job growth is a different metric than layoffs and require different considerations, both underscore the themes affecting the industry’s workforce.
Ani Turner, co-director of Altarum Institute’s Center for Sustainable Health Spending, told Healthcare Dive there have been some clear trends in hospital job growth in recent years. In 2013, there was little job growth but the expanded coverage affect — where more individuals gained health insurance for the first time under the ACA — helped spur hospital job growth in 2014.
This expanded coverage helped hospitals experience new revenue opportunities thanks to more people entering the care delivery space, especially in states that expanded Medicaid. In addition, since the implementation of the ACA, the level of uncompensated care nationwide has gone down from $46.4 billion in 2013 to $35.7 billion in 2015.
Since that time, hospitals experienced great growth from a jobs perspective. In a 2015 Forbes article, Politico’s Dan Diamond noted that healthcare job growth surged at its fastest pace since 1991 starting in July 2014 up through May of 2015. In fact, healthcare practitioners and healthcare support positions are expected to be among the fastest growing jobs from 2014 to 2024. BLS notes the aging population and expanded insurance coverage will help fuel this growth as demand for healthcare services increases.
The recent surge is “somewhat unexpected,” Turner says. “One would think hospitals would be conservative in their hiring. Everything I’m seeing is flat or slightly declining volumes, especially on inpatient side.”
“The data don’t always cooperate with the story that makes sense,” Turner added.
Brian Augustian, principal at Deloitte, believes the job growth is going to continue to slow this year in part because there will be a push for greater automation and productivity. “As organizations are able to use machine learning, artificial intelligence and better utilize technology to get tasks done, it will not only result in…needing fewer people but also different types of people,” he told Healthcare Dive.
The rate of job growth will be an issue to watch throughout the year. As shown above, just two months worth of data changes the story from a narrative of “slowing growth” to “continuing to soar.” The looming retirement of registered nurses and the aging population do point to hospitals and providers arming themselves to smooth the transition of both the workforce as well as the pending flood of baby boomers entering into the care space.
Job growth doesn’t stop financial troubles for providers
However, as seen in the job cut announcements and recent quarterly earnings for hospital operators, providers are facing challenges that are affecting their bottom lines.
One of the biggest challenges for providers is declining or flattening admissions. In 2010, all hospital admissions totaled 36.9 million admissions. By 2013, admissions had dropped by 1.5 million; 35 million patients were admitted in 2015.
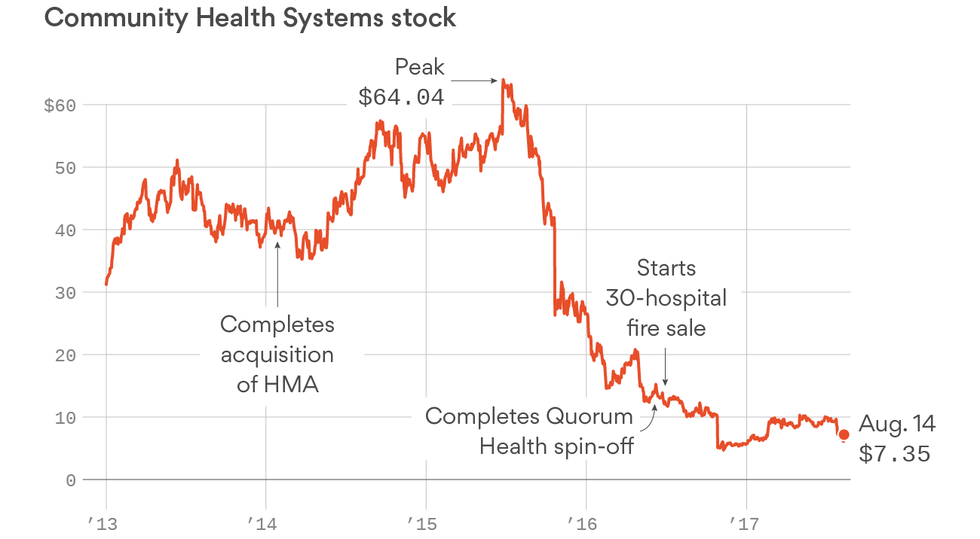
In the latest rounds of quarterly earnings, most for-profit hospital operators took a lashing, all acknowledging softening markets and weaker-than-expected patient volumes. Community Health Systems (CHS) reported it underperformed in Q2 2017 and is exploring more divestitures while HCA Healthcare reported it missed Q2 estimates due in part to higher expenses and lower-than-expected patient admissions. On Monday, Tenet Health reported a 4.5% decline in total admissions for the first six months of 2017.
Indiana University Health’s operating income suffered a 46% loss while seeing less individuals coming into the facilities, Modern Healthcare reported.
As seen in HCA Healthcare’s Q2 earnings call, lower acuity visits declined in the last quarter. At CHS, emergency department volume declined on the outpatient side, which Tim Hingtgen, president and COO of CHS, attributed to “industry dynamics, including urgent care growth, freestanding ED competition in select markets.” As Turner notes, the average person seeking a care setting visit is likely going to a physician’s office. This puts pressure on operators to rethink their lower acuity setting strategies and not rest on the strength of organic patient growth seen in previous years.
Another major issue for providers are expenses. More jobs equals more expenses, for example. Facility maintenance, equipment, electricity, telephone lines, internet, etc. all add up. According to the American Hospital Association, expenses for all U.S. registered hospitals are currently $936 billion, up from $859.4 billion in 2013. In addition to these changes, turning toward value-based care exposes providers more to risk-based contracts which can affect reimbursement formulas.
Hospitals know they need to lower cost structures, and personnel changes is one means
Ben Isgur, director of PricewaterhouseCoopers’ Health Research Institute, adds that squeezing costs isn’t a new concept for hospitals. There are many options for executives to manage out costs from its overhead. Supply chain, infrastructure and third party contracts are all go-to areas for such efforts. If two systems merge, departments can be streamlined or share services. In some cases, third-party contractors may be more beneficial to a provider than hiring for internal positions.
Igor Belokrinitsky, healthcare strategist at Strategy&, a member of the PwC network of firms, told Healthcare Dive in March many administrators faced with financial challenges tell their departments during the budgeting process to budget for zero cost increases or even for a reduction. “In the longer run, we are seeing and are working with health systems to take out pretty significant amounts of cost out of their operations, both clinical and nonclinical, and setting targets like 15-20%, which is a transformative change,” he said. “When talking about a 20% cost improvement, you’re questioning, ‘Do we need this facility? Do we need to provide this service at this location? Does this service need to be provided by a physician?'”
The current political landscape isn’t helping matters either
Isgur tells Healthcare Dive that healthcare industry layoffs should be watched closely and agrees with Turner that one of the biggest reasons is uncertainty in the industry.
As an example, he points to the Congressional Budget Office’s figure that 15 million individuals could have lost health coverage in 2018 if the Senate ACA repeal bill had become law. “Providers look at that and have to be ready for an environment where they have potentially fewer paying patients,” Isgur told Healthcare Dive.
During the heady time when ACA repeal-and/or-replace was on Congress’ plate this summer, many projections showed healthcare jobs would’ve been affected. One analysis of the House ACA bill estimated 725,000 jobs across the entire industry would be lost by 2026 if it had become law. The primary cause of the job disappearances and state economic downturns would have been attributable to cuts to healthcare funding, such as more than $800 billion to Medicaid, and lower premium subsidies.
Moody’s Investor Services projected the Senate ACA repeal bill would have caused uncompensated care costs to rise at hospitals.
The fight over healthcare policy is likely now headed to the executive branch, as Congress has failed to pass a bill that repeals or replaces the ACA. President Donald Trump has cost-sharing reduction payments to insurers hanging in the balance, and hasn’t publicly stated if the White House will continue to make these payments.
If these payments are discontinued, Fitch Ratings found in a new report that premiums could increase to the point where customers won’t be able to pay for coverage, thus increasing the chance for uncompensated payments to rise.
In addition, state Medicaid waivers will have to be looked at. Some applications, such as the Maine’s, could include work requirements, mandatory premiums and asset testing. It would be one of the most conservative state programs, and some health policy experts warn that the restrictions would push out many low-income adults who would otherwise qualify.
“When you add uncertainty to what’s already been going on in the reimbursement environment around how many more uninsured there may be going forward, that’s not the cause of [layoffs] but it’s certainly going to accelerate the thinking of executive teams to make sure [their organizations] are efficient and ready for anything,” Isgur said.
Isgur does think the industry will see more layoff announcements this year, but that it is an important trend to watch, especially as more decisions come out of Washington.