https://www.medpagetoday.com/infectiousdisease/covid19/85827?xid=nl_mpt_investigative2020-04-08&eun=g885344d0r&utm_source=Sailthru&utm_medium=email&utm_campaign=InvestigativeMD_040820&utm_term=NL_Gen_Int_InvestigateMD_Active

— Health systems see massive disruption from COVID-19
In Michigan, Trinity Health is furloughing 2,500 of its 24,000 employees. In Florida, Sarasota Memorial Health Care is taking “immediate steps to reduce costs, including temporary furloughs and reduced hours” for workers.
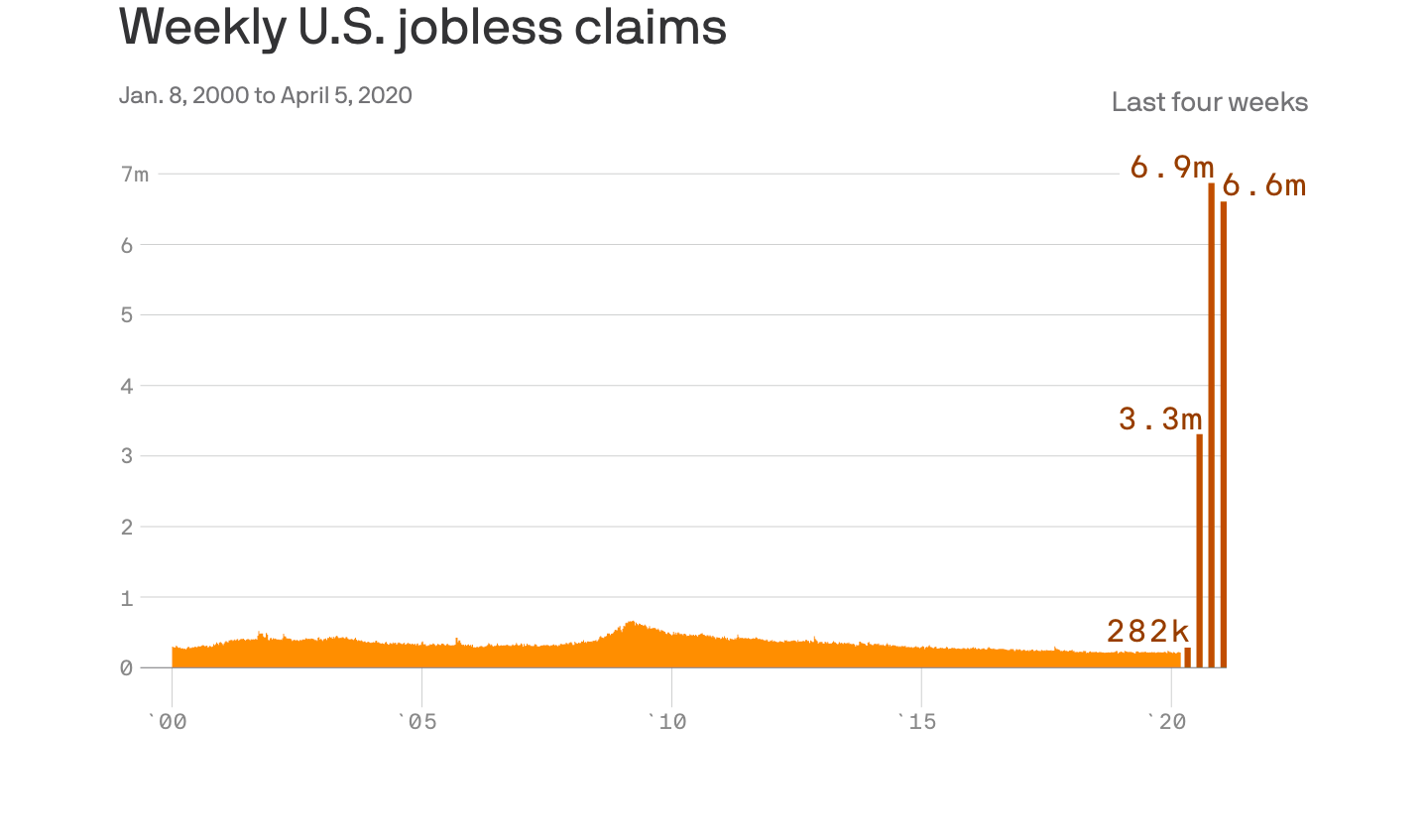
In less than 1 month, COVID-19 has made swift, deep cuts in hospital billings. Despite high volumes in the first 2 weeks, March revenue plunged by $16 million at Sarasota Memorial. Surgery cases fell by more than 50%, and volumes dropped by 45% at two emergency care centers and by 66% at seven urgent care centers.
Squeezed by plummeting income and climbing COVID-19 expenses, hospitals and health systems are bracing themselves for system-wide disruption by announcing temporary layoffs, reassignments, and pay cuts.
Many changes, like Trinity’s furloughs in Michigan, affect mainly non-clinical workers. Some alter compensation or duties for doctors, nurses, and other healthcare providers.
“In all parts of the country, physicians are being asked to sign agreements or acknowledgments for pay cuts ranging from 20% to 75%, depending on what their specialty is, where they are, and what the institutions are doing,” said Scott Weavil, JD, a California lawyer who counsels physicians nationwide about employment contracts.
“Many of these providers are not on the front lines of COVID, but they are still working,” Weavil noted. “Babies are being born. People are having accidents and visiting emergency departments. Urgent surgeries are happening. Physicians are at work or on call and ready to help if needed. And in most of these environments, there are patients who have tested positive for COVID-19,” he told MedPage Today.
“Ob/gyns aren’t doing a lot of elective procedures like hysterectomies, but they are delivering babies for COVID-positive patients, wearing donated cloth masks that may or may not be effective,” Weavil added.
In some cases, doctors have been sidelined and face the prospect of dwindling income as patient volumes fall. “We have 2,600 physicians and advanced-practice providers,” said Mark Briesacher, MD, senior vice president and chief physician executive of Intermountain Healthcare in Salt Lake City. “About 800 of them are on a patient volume-related type of contract, similar to what you would have in private practice.”
Because non-urgent and elective procedures are being delayed, some of these clinicians now see 30% to 50% fewer patients and could face big income drops, Briesacher told MedPage Today. “But we’ve put a floor in place,” he said: these providers will receive their usual pay until May 30, then 85% of that amount until normal patient volumes resume.
Redeployment can help practitioners make up lost income, Briesacher added. “A general surgeon often has critical care training,” he noted. “When this increase in patient care needs due to COVID-19 does come to Utah, we can deploy that surgeon to work in our ICUs with a critical care doctor, and if they’re working fulltime, they’ll get paid the same as they were before.”
Reassignment does not stop with doctors at Intermountain: hospital nurses can be deployed to screening desks, drive-through testing sites, or telehealth centers and will keep their current rate of pay, spokesperson Daron Crowley said.
“I recently reviewed a COVID-19 compensation plan of a health system in Florida that would give physicians their base or draw, or a midpoint between their 2019 base and their 2019 overall compensation,” noted Weavil, the attorney. “That seemed pretty good, but it came at a cost: the physicians had to agree to practice outside of their normal setting, as long as they were credentialed for the work.”
“At first blush, the credentialing requirement sounded like a protection; if you are a psychiatrist, you’d think ‘they’re not going to send me to the ICU,’ and normally, that’s correct,” Weavil continued.
But hospitals are adopting emergency credentialing provisions during COVID-19 and “doctors can be forced to practice pretty far afield of their specialty,” he said. In some ways, the situation resembles residency, he pointed out: “You have an attending physician who knows what she’s doing directing fish-out-of-water physicians who have been conscripted into service beyond their specialties.”
The list of hospital systems announcing major changes — including pay cuts for hospital executives, as Trinity Health in Michigan has done — grows each day. Boston Medical Center Health System has furloughed 700 employees; Cincinnati-based Bon Secours Mercy Health has announced it will do the same. Kentucky’s Appalachian Regional Healthcare will furlough about 500 staff members. South Carolina’s Prisma Health will lay off an undisclosed number of clinical, corporate, and administrative workers. Tenet Healthcare in Dallas has furloughed 500 fulltime positions.
Furloughing staff “was an extremely difficult decision, and one that we did not make lightly,” Sarasota Memorial CEO David Verinder wrote in a letter to employees.
“Staff have gone above and beyond to care for our patients throughout this crisis, even as they have been anxious about the health and well-being of themselves and their families,” he continued. “But as the health care safety net for the region, we must do all we can to continue fulfilling that critical role in the weeks ahead and for the long-term.”