The Biden administration has proposed giving rehabilitation facilities a 2.2% payment increase for the 2022 federal fiscal year that starts in October.
The payment rate outlined in a proposed rule released late Thursday is slightly below the 2.4% that CMS gave rehab facilities for the 2021 federal fiscal year. CMS proposed in a separate rule a 2.3% increase for payments to inpatient psychiatric facilities as well.
Both payment rules also give updates on outlier payments, which help facilities deal with the costs of treating extremely costly beneficiaries.
For rehab facilities, CMS proposes to maintain outlier payments to 3% of the total facility payments for fiscal 2022, which begins on Oct. 1.
CMS also aims to keep the outlier payments for psychiatric facilities at 2% for 2022.
A major change for both rules is a new addition aimed to track coverage of COVID-19 vaccinations among healthcare personnel.
CMS also wants to add vaccination coverage among healthcare personnel as a measure to the quality reporting program for psychiatric facilities. The program outlines quality metrics that facilities need to meet.
“This measure would be reported using the COVID-19 modules on the [Centers for Disease Control and Prevention’s] National Healthcare Safety Network web portal,” a fact sheet on the psychiatric payment rule said.
The agency also is proposing a similar measure for rehab facilities to report any vaccinations of healthcare personnel for COVID-19.
“This proposed measure is designed to assess whether [IRFs] are taking steps to limit the spread of COVID-19 among their [healthcare personnel], reduce the risk of transmission within their facilities and help sustain the ability of [rehabilitation facilities] to continue serving their communities through the public health emergency and beyond,” a fact sheet on the rehab rule said.
In the rehab facility rule, CMS also asked for comments on how to improve health equity for all patients.
CMS is seeking comments on whether to add more measures that address patient equity in standardized patient assessment data elements, which must be collected by facilities after post-acute care.
The agency also wants comments on ways to attain health equity for psychiatric facilities as well.
“CMS is committed to addressing the significant and persistent inequities in health outcomes in the United States through improving data collection to better measure and analyze disparities across programs and policies,” the agency said in a fact sheet.
President Joe Biden proposed an ambitious budget for the next federal fiscal year that includes more money for fighting the opioid epidemic, bolstering public health and several other healthcare items.
The budget request to Congress, released Friday, acts as essentially a wish list of priorities for the administration for the next year.
It is doubtful how much would get approved by Congress but sends a message of what the administration prioritizes.
Here are three healthcare priorities outlined in the request:
The opioid epidemic:$10.7 billion was requested for fighting the opioid epidemic, $3.9 billion over the 2021 enacted level. The money will help support research, prevention and recovery services. The administration also is calling for targeted investments for “populations with unique needs, including Native Americans, older Americans and rural populations,” according to a release from the Office of Management and Budget on Friday.
Public health infrastructure:$8.7 billion was requested for the Centers for Disease Control and Prevention to boost public health capacity in states and territories. OMB calls the budget increase the largest in nearly two decades for the agency at the frontlines of combating COVID-19. The Biden administration hopes to use the new money to train new epidemiologists and public health experts and “build international capacity to detect, prepare for and respond to emerging global threats.” A letter sent Friday to congressional leaders from the White House said that CDC funding was 10% lower than the previous decade after adjusting for inflation.
Research funding boosts:$6.5 billion to launch a new agency called the Advanced Research Projects Agency for Health. The new agency would provide major increases in federal research and development spending on cancer and other diseases such as diabetes and Alzheimer’s. The goal of the investment is to “drive transformational innovation in health research and speed application and implementation of health breakthroughs,” OMB’s letter to Congress said. The funding is rolled into a $51 billion request for funding to the National Institutes of Health.
A new report out later today concludes that basic scientific research plays an essential role in creating companies that later produce thousands of jobs and billions in economic value.
Why it matters: The report uses thepandemic — and especially the rapid development of new mRNA vaccines — to show how basic research funding from the government lays the necessary groundwork for economically valuable companies down the road.
By the numbers: The Science Coalition — a nonprofit group that represents 50 of the nation’s top private and public research universities — identified 53 companies that have spun off from federally funded university research.
Those companies — which range from pharmaceutical startups to agriculture firms — have contributed more than $1.3 billion to U.S. GDP between 2015 and 2019, while supporting the creation of more than 100,000 jobs.
What they’re saying:“The COVID-19 pandemic has shown that the need for the federal government to continue investing in fundamental research is far from theoretical,” says John Latini, president of the Science Coalition. “Consistent, sustained, robust federal funding is how science evolves.”
Details: Latini praised the Biden administration’s first budget proposal to Congress, released last week, which includes what would be a $9 billion funding boost for the National Institutes of Health (NIH) — the country’s single biggest science research funding agency.
The National Oceanic and Atmospheric Administration would see its budget rise to a record high of $6.9 billion, including $800 millionreserved for climate research.
The catch: The Biden budget proposal is just that, and it will ultimately be up to Congress to decide how much to allocate to research agencies.
Context: Government research funding is vital because private money tends to go to applied research. But without basic research — the lifeblood of science — the U.S. risks missing out on potentially world-changing innovations in the future.
The long-term value of that funding can be seen in the story of Katalin Kariko, an obscure biomedical researcher who labored for years on mRNA with little reward — until the pandemic, when her work helped provide the foundation for mRNA COVID-19 vaccines.
The bottom line: Because its ultimate payoff might lay years in the future, it’s easy to see basic research funding as a waste — until the day comes when we need it.
There’s widespread agreement that it’s important to help older adults and people with disabilities remain independent as long as possible. But are we prepared to do what’s necessary, as a nation, to make this possible?
That’s the challenge President Joe Biden has put forward with his bold proposal to spend $400 billion over eight years on home and community-based services, a major part of his $2 trillion infrastructure plan.
It’s a “historic and profound” opportunity to build a stronger framework of services surrounding vulnerable people who need considerable ongoing assistance, said Ai-jen Poo, director of Caring Across Generations, a national group advocating for older adults, individuals with disabilities, families and caregivers.
It comes as the coronavirus pandemic has wreaked havoc in nursing homes, assisted living facilities and group homes, killing more than 174,000 people and triggering awareness of the need for more long-term care options.
“There’s a much greater understanding now that it is not a good thing to be stuck in long-term care institutions” and that community-based care is an “essential alternative, which the vast majority of people would prefer,” said Ari Ne’eman, senior research associate at Harvard Law School’s Project on Disability.
“The systems we do have are crumbling” due to underfunding and understaffing, and “there has never been a greater opportunity for change than now,” said Katie Smith Sloan, president of LeadingAge, at a recent press conference where the president’s proposal was discussed. LeadingAge is a national association of more than 5,000 nonprofit nursing homes, assisted living centers, senior living communities and home care providers.
But prospects for the president’s proposal are uncertain. Republicans decry its cost and argue that much of what the proposed American Jobs Plan contains, including the emphasis on home-based care, doesn’t count as real infrastructure.
“Though this [proposal] is a necessary step to strengthen our long-term care system, politically it will be a challenge,” suggested Joseph Gaugler, a professor at the University of Minnesota’s School of Public Health, who studies long-term care.
Even advocates acknowledge the proposal doesn’t address the full extent of care needed by the nation’s rapidly growing older population. In particular, middle-income seniors won’t qualify directly for programs that would be expanded. They would, however, benefit from a larger, better paid, better trained workforce of aides that help people in their homes — one of the plan’s objectives.
“This [plan] isn’t everything that’s needed, not by any step of the imagination,” Poo said. “What we really want to get to is universal access to long-term care. But that will be a multistep process.”
Understanding what’s at stake is essential as communities across the country and Congress begin discussing Biden’s proposal.
The services in question.Home and community-based services help people who need significant assistance live at home as opposed to nursing homes or group homes.
Services can include home visits from nurses or occupational therapists; assistance with personal care such as eating or bathing; help from case managers; attendance at adult day centers; help with cooking, cleaning and other chores; transportation; and home repairs and modifications. It can also help pay for durable medical equipment such as wheelchairs or oxygen tanks.
The need. At some point, 70% of older adults will require help with dressing, hygiene, moving around, managing finances, taking medications, cooking, housekeeping and other daily needs, usually for two to four years. As the nation’s aging population expands to 74 million in 2030 (the year all baby boomers will have entered older age), that need will expand exponentially.
Younger adults and children with conditions such as cerebral palsy, blindness or intellectual disabilities can similarly require significant assistance.
The burden on families. Currently, 53 million family members provide most of the care that vulnerable seniors and people with disabilities require — without being paid and often at significant financial and emotional cost. According to AARP, family caregivers on average devote about 24 hours a week, to helping loved ones and spend around $7,000 out-of-pocket.
This reflects a sobering reality: Long-term care services are simply too expensive for most individuals and families. According to a survey last year by Genworth, a financial services firm, the hourly cost for a home health aide averages $24. Annually, assisted living centers charge an average $51,600, while a semiprivate room in a nursing home goes for $93,075.
Medicare limitations. Many people assume that Medicare — the nation’s health program for 61 million older adults and people with severe disabilities — will pay for long-term care, including home-based services. But Medicare coverage is extremely limited.
In the community, Medicare covers home health only for older adults and people with severe disabilities who are homebound and need skilled services from nurses and therapists. It does not pay for 24-hour care or care for personal aides or homemakers. In 2018, about 3.4 million Medicare members received home health services.
In nursing homes, Medicare pays only for rehabilitation services for a maximum of 100 days. It does not provide support for long-term stays in nursing homes or assisted living facilities.
Medicaid options. Medicaid — the federal-state health program for 72 million children and adults in low-income households — can be an alternative, but financial eligibility standards are strict and only people with meager incomes and assets qualify.
Medicaid supports two types of long-term care: home and community-based services and those provided in institutions such as nursing homes. But only care in institutions is mandated by the federal government. Home and community-based services are provided at the discretion of the states.
Although all states offer home and community-based services of some kind, there’s enormous variation in the types of services offered, who is served (states can set caps on enrollment) and state spending. Generally, people need to be frail enough to need nursing home care to qualify.
Nationally, 57% of Medicaid’s long-term care budget goes to home and community-based services — $92 billion in the 2018 federal budget year. But half of states still spend twice as much on institutional care as they do on community-based care. And 41 states have waiting lists, totaling nearly 820,000 people, with an average wait of 39 months.
Based on the best information available, between 4 million and 5 million people receive Medicaid-funded home and community-based services — a fraction of those who need care.
Workforce issues. Biden’s proposal doesn’t specify how $400 billion in additional funding would be spent, beyond stating that access to home and community-based care would be expanded and caregivers would receive “a long-overdue raise, stronger benefits, and an opportunity to organize or join a union.”
Caregivers, including nursing assistants and home health and personal care aides, earn $12 an hour, on average. Most are women of color; about one-third of those working for agencies don’t receive health insurance from their employers.
By the end of this decade, an extra 1 million workers will be needed for home-based care — a number of experts believe will be difficult, if not impossible, to reach given poor pay and working conditions.
“We have a choice to keep these poverty-wage jobs or make them good jobs that allow people to take pride in their work while taking care of their families,” said Poo of Caring Across Generations.
Next steps.Biden’s plan leaves out many details. For example: What portion of funding should go to strengthening the workforce? What portion should be devoted to eliminating waiting lists? What amount should be spent on expanding services?
How will inequities of the current system — for instance, the lack of accessible services in rural counties or for people with dementia — be addressed? “We want to see funding to states tied to addressing those inequities,” said Amber Christ, directing attorney of the health team at Justice in Aging, an advocacy organization.
Meanwhile, supporters of the plan suggest it could be just the opening of a major effort to shore up other parts of the safety net. “There are huge gaps in the system for middle-income families that need to be addressed,” said David Certner, AARP’s legislative counsel.
Reforms that should be considered include tax credits for caregivers, expanding Medicare’s home health benefit and removing the requirement that people receiving Medicare home health be homebound, said Christ of Justice in Aging.
”We should be looking more broadly at potential solutions that reach people who have some resources but not enough to pay for these services as well,” she said.
All the things that could prolong the COVID-19 pandemic — that could make this virus a part of our lives longer than anyone wants — are playing out right in front of our eyes.
Driving the news: The British variant is driving another surge in cases in Michigan, and Gov. Gretchen Whitmer has resisted reimposing any of the lockdown measures she embraced earlier in the pandemic.
Variants are beginning to infect more kids — “a brand new ball game,” as University of Minnesota epidemiologist Michael Osterholm recently put it.
New research confirms that our existing vaccines don’t work as well against the South African variant.
And some experts fear the pace of vaccinations in the U.S. is about to slow down.
Between the lines:The concern isn’t necessarily that the facts on the ground right now could end up being disastrous, but rather that we’re getting a preview of the longer, darker coronavirus future the U.S. may face without sufficient vaccinations.
If we don’t control the virus well enough, then even years into the future, we could be living through more new variants — some of which might be more deadly, some of which might be more resistant to vaccines, some of which might be more dangerous for certain specific populations.
That would translate into an ongoing risk of illness or potentially death for unvaccinated people and new races to reformulate vaccines as new variants keep emerging.
And it would lead to a world in which today’s vaccine-eager population would have to stay on top of those emerging risks, get booster shots when they’re available, and perhaps revive some of the pandemic’s social-distancing measures, in order to stay safe.
I got my first Pfizer vaccine in January. Is it too late to get the second injection now, more than two months later? What should I do?
The second dose of Pfizer-BioNTech’s vaccine should ideally be given three weeks after the first. (Moderna’s second dose is meant to be given four weeks after the first, while the Johnson & Johnson/Janssen shot is delivered in a single dose.) But, well, sometimes life gets in the way. So what happens if you don’t make it to that second appointment?
Schedule another one as soon as you can, says Dr. Adam Ratner, a pediatric infectious disease doctor at NYU Langone Health and a vaccine researcher.
While a three- or four-week gap between shots is ideal, the U.S. Centers for Disease Control and Prevention (CDC) saysyou can get your second shot within 42 days of the first one and still mount a full immune response. “Beyond that, we start to operate in an area where there’s simply less data,” Ratner says.
That doesn’t mean your second shot will be ineffective if it’s given more than six weeks after the first. It only means that studies have not specifically measured how much protection the two-dose vaccines offer when the shots are given more than 42 days apart. Still, the CDC says you don’t have to start over if you can’t get a second vaccine within 42 days. Countries including the U.K. are even purposely delaying second shots so they can get first doses out to more people, and some experts in the U.S. advocate for the same policy.
Ratner says if he were in your shoes, he wouldn’t worry too much. “I would say get the second dose now and consider yourself fully vaccinated,” he says. Just make sure you get a second dose of the same vaccine, since the CDC does not recommend mixing and matching with different shots.
It may be tempting to just stick with the one dose you’ve got—after all, one recent study showed that a single dose of the vaccine was about 80% effective at preventing COVID-19 infections, compared to 90% protection after two doses. But “it is somewhat of a tenuous 80%,” National Institute of Allergy and Infectious Diseases Director Dr. Anthony Fauci said at a recent press briefing. “When you leave it at one dose, the question is, ‘How long does it last?’”
To get the vaccine’s full benefits, and to make sure they last as long as possible, you’ll need a second shot.
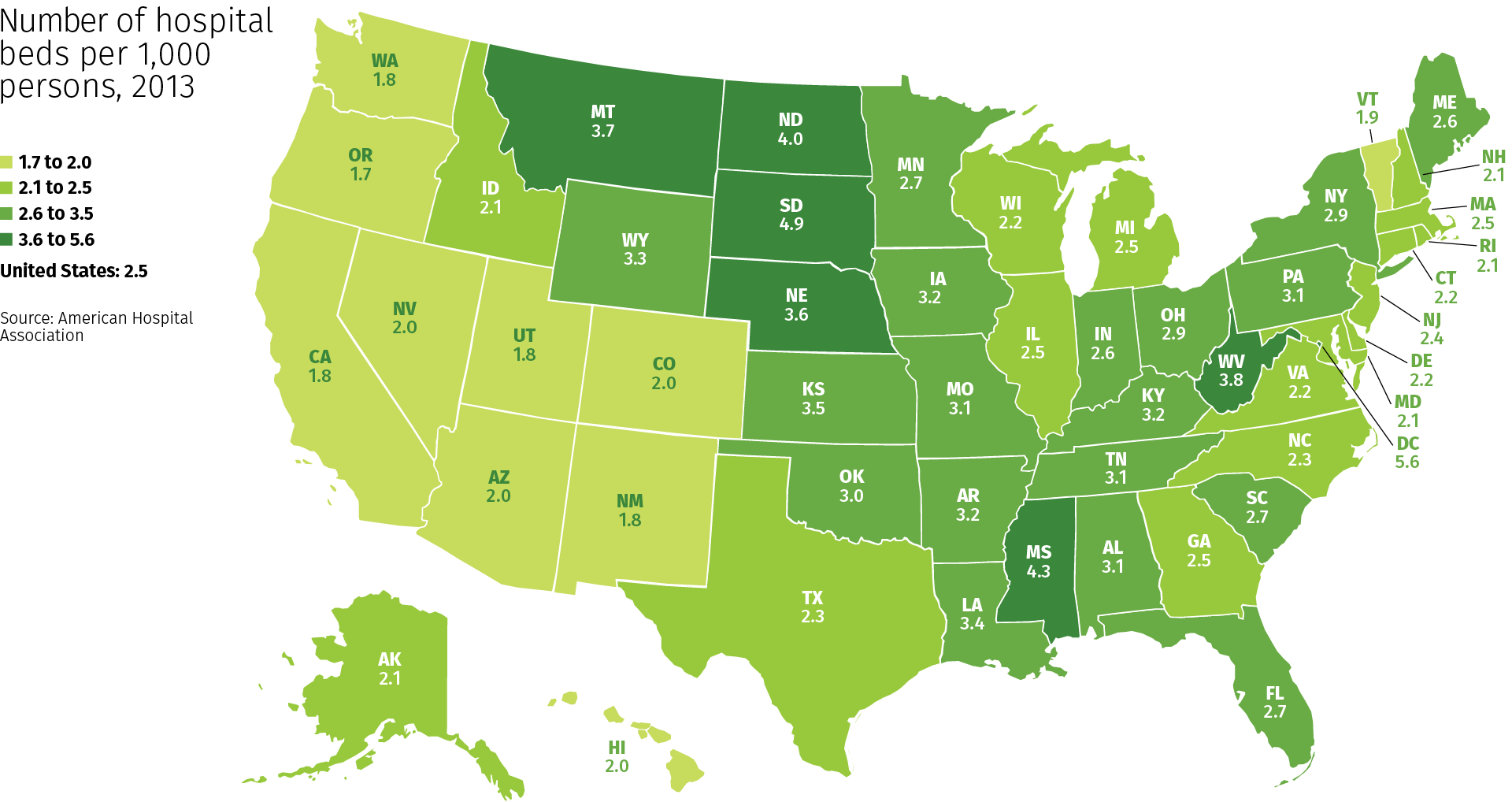
South Dakota has the highest number of hospital beds per 1,000 population in the U.S., while Oregon and Washington have the lowest, according to a ranking from the Kaiser Family Foundation.
The data is based on an analysis of the American Hospital Association’s annual survey from 2015 to 2019.
The national average per 1,000 U.S. residents was 2.4 hospital beds.
Here are the U.S. states ranked by number of staffed hospital beds per 1,000 population:
Note: The list includes ties and results in a numerical listing of 22.
Cancer Treatment Centers of America is selling its hospital in Philadelphia and will lay off the facility’s 365 employees, according to a closure notice filed with the state.
Boca Raton, Fla.-based Cancer Treatment Centers of America signed an agreement in March to sell the hospital to Philadelphia-based Temple University Hospital. The deal requires approval from the Pennsylvania Department of Health.
In the notice filed with the state, Cancer Treatment Centers of America said some displaced Philadelphia workers may be offered jobs at affiliated entities outside of Pennsylvania, according to the Philadelphia Business Journal. The company’s other hospitals are in Chicago, Atlanta, Phoenix and Tulsa, Okla. In March, the company announced it will close its hospital in Tulsa June 1.
Cancer Treatment Centers of America said it anticipates the layoffs in Philadelphia will begin after May 30, according to the Philadelphia Business Journal.
Temple Health CEO Michael Young told the Philadelphia Business Journal that the system wants to hire as many CTCA workers as possible if the deal is finalized.
President Joe Biden moved to unwind Medicaid work requirements in Michigan and Wisconsin, after pulling the rules in Arkansas and New Hampshire.
CMS sent letters to health officials in Michigan and Wisconsin April 6 withdrawing their approval to implement work requirements for Medicaid beneficiaries. In both letters, CMS noted that combined with the COVID-19 pandemic, the work rules risk “significant coverage losses and harm to beneficiaries.”
In March, the Biden administration revoked approval for similar Medicaid work requirements in Arkansas and New Hampshire.
Centers for Disease Control and Prevention (CDC) Director Rochelle Walensky finds herself in a delicate position as she seeks to balance the optimism of increasing vaccinations with the reality that the U.S. is still very much in the grip of a deadly pandemic.
Walensky started the CDC job with a reputation as a savvy communicator, tasked with salvaging the reputation of an agency that took a beating under the Trump administration.
“When I first started at CDC about two months ago, I made a promise to you: I would tell you the truth, even if it was not the news we wanted to hear,” Walensky told reporters recently.
Walensky’s expertise is in HIV research, like her predecessor Robert Redfield, and before being appointed to lead the CDC, she was head of infectious diseases at Massachusetts General Hospital.
While former colleagues say Walensky is the perfect fit for the CDC post, her skills are now being put to the test as she faces criticism for being both too negative and too hopeful.
“She is quite a compelling and clear communicator, but it’s a challenging set of messages to try and get out there,” said Chris Beyrer, a professor of epidemiology at Johns Hopkins Bloomberg School of Public Health.
Public health messaging during a global pandemic is complicated enough, but experts say this particular moment is especially difficult.
After weeks of decline and then stagnation, the rate of coronavirus infections has once again started to climb across much of the country. Cases are up about 12 percent nationally compared with the previous week, averaging around 62,000 cases per day, according to the CDC.
At the same time, nearly 100 million Americans have received at least one dose of a coronavirus vaccine. Many states are expanding vaccine eligibility, in some instances to all adults, and federal health officials say there will be enough supply for everyone to be vaccinated by the end of May.
Walensky tried to emphasize both aspects this week when she issued an emotional appeal to the public.
“We have so much to look forward to, so much promise and potential of where we are, and so much reason for hope. But right now I’m scared,” Walensky said, adding that she had a “sense of impending doom” if people continued to ignore public health precautions.
Yet almost in the next breath, she talked about a “tremendously encouraging” new study showing that vaccinated people were 90 percent protected from infection, meaning they pose an extremely low risk of spreading the virus.
While that may come across as mixed messaging, experts say it accurately reflects not only where things stand right now but also how the country has been reacting to the virus for the past year.
“Whiplash is a true reflection of how we’re all experiencing the epidemic and the response to it. So I’d rather she be honest about that and others be honest about that than give people something that they want … to make them feel better,” said Judith Auerbach, a professor in the University of California San Francisco School of Medicine.
Auerbach, who previously worked with Walensky on HIV research, praised the director’s openness, which she said had been missing from agency leadership during the Trump administration.
“She’s being really honest about her own emotions. That’s hard for a fed to do and get away with,” Auerbach said. “The science that says we all still need to be, in fact, quite scared because we’re in this race between the vaccines … versus the emergence of these variants, and she felt it at a visceral level, and she conveyed that in a way that I thought was quite telling.”
Glen Nowak, director of the Center for Health and Risk Communication at the University of Georgia and a former CDC media relations director, said Walensky’s candor helps establish credibility.
“She has embraced the fact that credibility comes from being transparent and honest and genuine about your fears and your concerns,” Nowak said.
The CDC declined to make Walensky available for an interview, but in a statement to The Hill, an agency spokesman said every communication reflects the latest science and epidemiology.
“At times, moments must balance hope that we will move out of the pandemic with the reality that we are not out of it yet,” the spokesman said.
“We acknowledge the challenge of conveying such hope and promise that vaccines offer with the reality that cases and deaths are rising. While we are sending the critical message that people cannot and should not let up on their prevention measures, we do remain very optimistic about what the future of a fully vaccinated public will offer,” the spokesman added.
On Friday, Walensky again came under criticism for her messaging. In updated guidance, the CDC said it is safe for people who have been fully vaccinated to travel.
But Walensky struck a cautionary tone by saying the CDC still recommends anyone, vaccinated or not, avoid nonessential travel because infection numbers are so high.
“We know that right now we have a surging number of cases,” Walensky said during a White House briefing. “I would advocate against general travel overall. Our guidance is silent on recommending or not recommending fully vaccinated people travel. Our guidance speaks to the safety of doing so.”
Nowak said part of what makes public health messaging so difficult is the fact that science doesn’t always deal in absolutes and that the public overall doesn’t do well with nuance.
“Often people don’t want to listen to the nuance; they want advice and guidance to be stable. They get frustrated with the changes or when it seems to be contradictory. They also get frustrated if it doesn’t match their everyday living experiences,” Nowak said.
With the travel guidance, Walensky attempted to spell out the balance she was trying to strike and asked the public for patience and understanding.
“I want to acknowledge today that providing guidance in the midst of a changing pandemic and its changing science is complex,” Walensky said.
“The science shows us that getting fully vaccinated allows you to do more things safely, and it’s important for us to provide that guidance, even in the context of rising cases.At the same time, we must balance the science with the fact that most Americans are not yet fully vaccinated, which is likely contributing to our rising cases,” she said.
Jen Kates, director for global health and HIV policy at the Kaiser Family Foundation, who has known Walensky for decades, said she thinks the CDC director is aware that she can’t escape criticism, especially when so many people have pandemic fatigue.
If the CDC is too strict and refuses to endorse relatively normal behavior, especially after people get vaccinated, it could risk others refusing to get the shot, Kates said.
But if the agency paints too rosy a picture, more people could act like the pandemic is over and risk further spread of the virus.
“It behooves public officials to always be cognizant that their words are being listened to and can be taken out of context or may be hard for people to grasp,” Kates said. “So I think Dr. Walensky is a great communicator, but that doesn’t mean that this is always easy to do and the balance is always straightforward.”