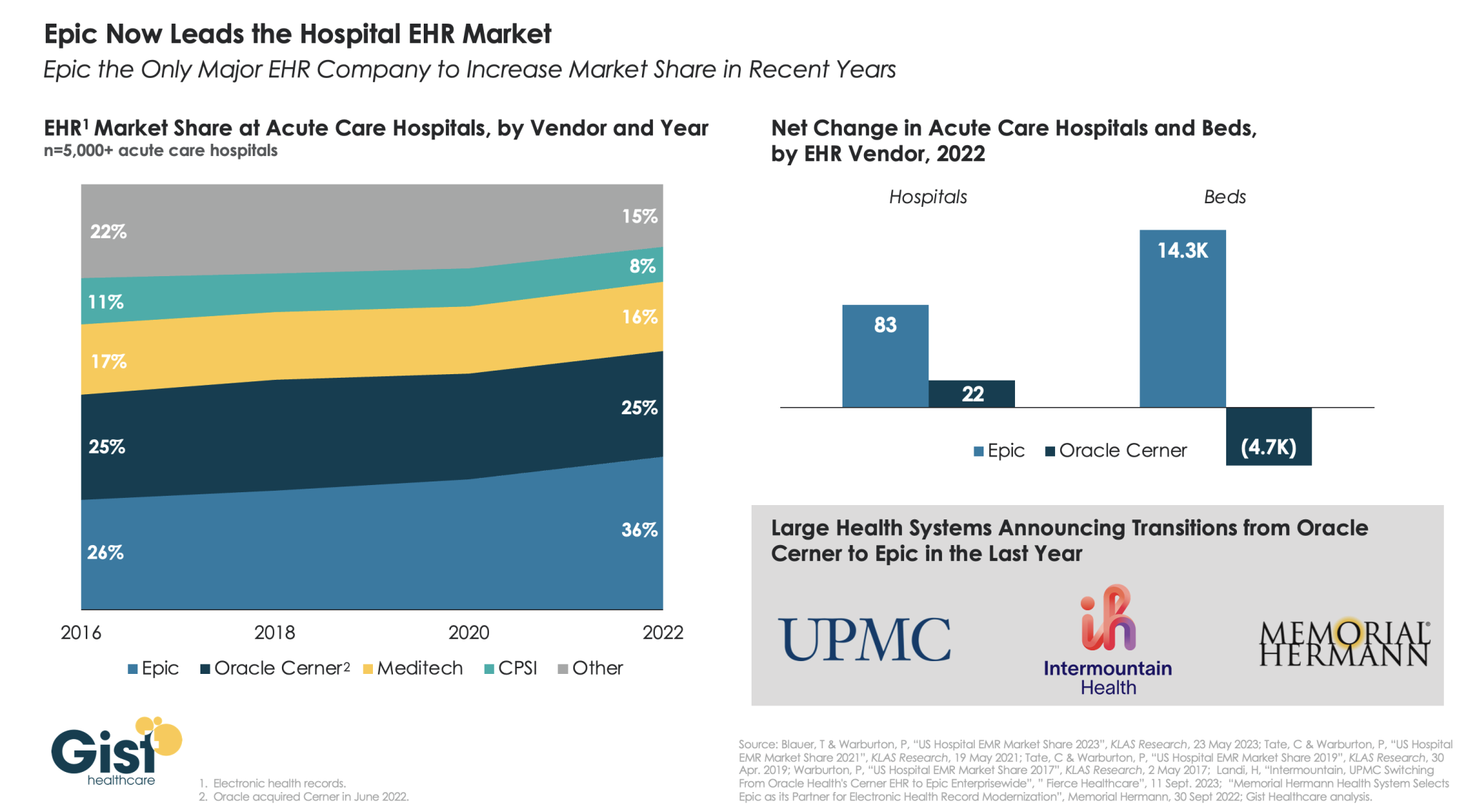
Two large nonprofit health systems made headlines earlier this month announcing that they plan to transition, enterprise-wide, from Oracle Cerner to Epic for their electronic health record (EHR) system.
Using data from KLAS Research, the graphic below shows how Epic has emerged in recent years as the leader in the hospital EHR market. From 2016 to 2022, Epic increased its acute care hospital market share from 26 percent to 36 percent, while its main rival, Oracle Cerner, held flat at 25 percent.
Moreover, Epic is gaining popularity among larger health systems,while Oracle Cerner lost almost 5K beds in 2022, despite gaining 22 hospitals, as it trades large systems for smaller hospitals.
Epic’s ability to consolidate multiple archives into a single, more functional platform has made it popular with physicians, whose feedback was cited by Intermountain as a key reason behind the system’s decision to switch.
With three quarters of Americans having an Epic record, the company is leveraging its pole position in aggregating healthcare data as healthcare approaches the cusp of a generative AI boom, recently announcing an expanded partnership with Microsoft focused on integrating AI tools into its EHR system.
Published this week in the Harvard Business Review, this intriguing case study tells the story of how Hawaii Pacific Health, a four-hospital system based in Honolulu, worked with its providers to reduce the deluge of needless or low-value administrative tasks required each day by the system’s electronic health record (EHR) platform.
The system’s “Get Rid of Stupid Stuff” (GROSS) initiative created a simple, accessible submission form that allowed providers to flag EHR prompts and workflows ranging from inefficient (printing and scanning discharge papers patients had already signed electronically) to nonsensical (affirming adolescent patients had received proper care for their non-existent umbilical cords). Around 10 percent of suggestions submitted were for prompts that could be immediately eliminated, 15 percent caught gaps in communication and workflow, and the remaining 75 percent identified more complex opportunities for redesign. The GROSS initiative not only freed thousands of labor hours, but also boosted morale by engaging clinicians in the system’s efforts to improve operations.
The Gist: While Hawaii Pacific Health is far from the only system to have successfully engaged its providers in the mission of reducing administrative busywork, this case study provides an example of how sometimes the simplest approaches can be the most effective.
As systems now look to generative AI as the next frontier of bureaucratic efficiency, they will need to optimize workflow processes before automating them in order to avoid ingraining today’s inefficiencies.
Two of the nation’s largest nonprofit health systems, Salt Lake City, UT-based Intermountain Healthcare and Pittsburgh, PA-based UPMC, have recently announced plans to end their electronic health record (EHR) contracts with Oracle Cerner and transition, enterprise-wide, to Epic.
Intermountain, which operates 33 hospitals across seven states, plans to integrate Epic’s EHR into all of its facilities by 2025; its legacy SCL Health hospitals in Colorado and Montana already use Epic.
UPMC, which operates 40 hospitals in three states, has set mid-2026 as the target for consolidating its nine EHRs into a single platform with Epic. It has been using Oracle Cerner in inpatient settings and Epic for ambulatory care.
Both systems cited provider feedback and a desire to simplify patient record-keeping as key reasons behind their decisions to switch.
The Gist: With two more marquee health systems jumping ship for Epic, Oracle Cerner faces a steeper battle to maintain a foothold with health systems and may need to rethink its target market and value proposition.
Cerner initially appealed to large, progressive, value-oriented systems with highly customizable offerings, but over the years the resulting “Franken-Cerner” systems (as one CIO put it) became hard to maintain and scale.
Meanwhile, Epic continues to grow its lead in the domestic EHR market: it now covers roughly half of acute-care beds in the US and holds records on 78 percent of US patients.
Sitting on troves of health data, Epic is also well-positioned to become a leader in the rollout of next-generation healthcare AI, which it has already set in motion through its partnership with Microsoft.
We had an interesting exchange with a health system CEO this week, which started as a discussion about what to tell his board about the rapidly changing AI landscape, but drifted into a larger conversation about how human-dependent healthcare is. His system has invested heavily in virtual care and has begun to make strides in applying automation and artificial intelligence to both clinical care delivery and key operational processes. He’s glimpsed the potential for process automation—AI’s less sexy sibling, now that “generative AI” has burst onto the scene—to radically reduce staffing costs in areas like revenue cycle management.
And that’s making him wonder about the larger implications for workforce development—both inside his organization and in the economy as a whole. Like many health systems, his organization not only provides care to the community, but also employment opportunities and job growth.
What happens when large swaths of healthcare delivery become more automated—how will the system look to retrain those workers for other roles?
One clear area of workforce need over the coming decades will be hands-on caregiving for an older, sicker population that wants to age in place. Health aides, home health workers, community social workers and so forth—will those roles ultimately be filled by workers from other parts of healthcare (and the economy beyond) who find themselves displaced by AI and robotics?
Will the Amazon warehouse worker of today become the home care worker of tomorrow?
The conversation was fascinating and made us realize that we’ve paid too little attention to two key issues.
First, the tension between healthcare as a cost problem and healthcare as a source of job growth.
And second, the redistribution of workers into roles that will require hands-on, human presence (like caregiving) in the coming wave of AI and robotics.
Five years ago, I started the Fixing Healthcare podcast with the aim of spotlighting the boldest possible solutions—ones that could completely transform our nation’s broken medical system.
But since then, rather than improving, U.S. healthcare has fallen further behind its global peers, notching far more failures than wins.
In that time, the rate of chronic disease has climbed while life expectancy has fallen, dramatically. Nearly half of American adults now struggle to afford healthcare. In addition, a growing mental-health crisis grips our country. Maternal mortality is on the rise. And healthcare disparities are expanding along racial and socioeconomic lines.
Reflecting on why few if any of these recommendations have been implemented, I don’t believe the problem has been a lack of desire to change or the quality of ideas. Rather, the biggest obstacle has been the immense size and scope of the changes proposed.
To overcome the inertia, our nation will need to narrow its ambitions and begin with a few incremental steps that address key failures. Here are three actionable and inexpensive steps that elected officials and healthcare leaders can quickly take to improve our nation’s health:
1. Shore Up Primary Care
Compared to the United States, the world’s most-effective and highest-performing healthcare systems deliver better quality of care at significantly lower costs.
One important difference between us and them: primary care.
In most high-income nations, primary care makes up roughly half of the physician workforce. In the United States, it accounts for less than 30% (with a projected shortage of 48,000 primary care physicians over the next decade).
Primary care—better than any other specialty—simultaneously increases life expectancy while lowering overall medical expenses by (a) screening for and preventing diseases and (b) helping patients with chronic illness avoid the deadliest and most-expensive complications (heart attack, stroke, cancer).
But considering that it takes at least three years after medical school to train a primary care physician, to make a dent in the shortage over the next five years the U.S. government must act immediately:
The first action is to expand resident education for primary care. Congress, which authorizes the funding, would allocate $200 million annually to create 1,000 additional primary-care residency positions each year. The cost would be less than 0.2% of federal spending on healthcare.
The second action requires no additional spending. Instead, the Centers for Medicare & Medicaid Services, which covers the cost of care for roughly half of all American adults, would shift dollars to narrow the $108,000 pay gap between primary care doctors and specialists. This will help attract the best medical students to the specialty.
Together, these actions will bolster primary care and improve the health of millions.
2. Use Technology To Expand Access, Lower Costs
A decade after the passage of the Affordable Care Act, 30 million Americans are without health insurance while tens of millions more are underinsured, limiting access to necessary medical care.
Furthermore, healthcare is expected to become even less affordable for most Americans. Without urgent action, national medical expenditures are projected to rise from $4.3 trillion to $7.2 trillion over the next eight years, and the Medicare trust fund will become insolvent.
With costs soaring, payers (businesses and government) will resist any proposal that expands coverage and, most likely, will look to restrict health benefits as premiums rise.
Almost every industry that has had to overcome similar financial headwinds did so with technology. Healthcare can take a page from this playbook by expanding the use of telemedicine and generative AI.
At the peak of the Covid-19 pandemic, telehealth visits accounted for 69% of all physician appointments as the government waived restrictions on usage. And, contrary to widespread fears at the time, patients and doctors rated the quality, convenience and safety of these virtual visits as excellent. However, with the end of Covid-19, many states are now restricting telemedicine, particularly when clinicians practice in a different state than the patient.
To expand telemedicine use—both for physical and mental health issues—state legislators and regulators will need to loosen restrictions on virtual care. This will increase access for patients and diminish the cost of medical care.
It doesn’t make sense that doctors can provide treatment to people who drive across state lines, but they can’t offer the same care virtually when the individual is at home.
Similarly, physicians who faced a shortage of hospital beds during the pandemic began to treat patients in their homes. As with telemedicine, the excellent quality and convenience of care drew praise from clinicians and patients alike.
Building on that success, doctors could combine wearable devices and generative AI tools like ChatGPT to monitor patients 24/7. Doing so would allow physicians to relocate care—safely and more affordably—from hospitals to people’s homes.
Translating this technology-driven opportunity into standard medical practice will require federal agencies like the FDA, NIH and CDC to encourage pilot projects and facilitate innovative, inexpensive applications of generative AI, rather than restricting their use.
3. Reduce Disparities In Medical Care
American healthcare is a system of haves and have-nots, where your income and race heavily determine the quality of care you receive.
Black patients, in particular, experience poorer outcomes from chronic disease and greater difficulty accessing state-of-the-art treatments. In childbirth, black mothers in the U.S. die at twice the rate of white women, even when data are corrected for insurance and financial status.
Generative AI applications like ChatGPT can help, provided that hospitals and clinicians embrace it for the purpose of providing more inclusive, equitable care.
Previous AI tools were narrow and designed by researchers to mirror how doctors practiced. As a result, when clinicians provided inferior care to Black patients, AI outputs proved equally biased. Now that we understand the problem of implicit human bias, future generations of ChatGPT can help overcome it.
The first step will be for hospitals leaders to connect electronic health record systems to generative AI apps. Then, they will need to prompt the technology to notify clinicians when they provide insufficient care to patients from different racial or socioeconomic backgrounds. Bringing implicit bias to consciousness would save the lives of more Black women and children during delivery and could go a long way toward reversing our nation’s embarrassing maternal mortality rate (along with improving the country’s health overall).
The Next Five Years
Two things are inevitable over the next five years. Both will challenge the practice of medicine like never before and each has the potential to transform American healthcare.
First, generative AI will provide patients with more options and greater control. Faced with the difficulty of finding an available doctor, patients will turn to chatbots for their physical and psychological problems.
Already, AI has been shown to be more accurate in diagnosing medical problems and even more empathetic than clinicians in responding to patient messages. The latest versions of generative AI are not ready to fulfill the most complex clinical roles, but they will be in five years when they are 30-times more powerful and capable.
Second, the retail giants (Amazon, CVS, Walmart) will play an ever-bigger role in care delivery. Each of these retailers has acquired primary care, pharmacy, IT and insurance capability and all appear focused on Medicare Advantage, the capitated option for people over the age of 65. Five years from now, they will be ready to provide the businesses that pay for the medical coverage of over 150 million Americans the same type of prepaid, value-based healthcare that currently isn’t available in nearly all parts of the country.
American healthcare can stop the current slide over the next five years if change begins now. I urge medical leaders and elected officials to lead the process by joining forces and implementing these highly effective, inexpensive approaches to rebuilding primary care, lowering medical costs, improving access and making healthcare more equitable.
On Tuesday, Verona, WI-based Epic and Redmond, WA-based Microsoft announced a suite of new AI-powered solutions available to users of Epic’s electronic health records (EHR) system.
In April 2023, Epic began integrating Microsoft’s Azure OpenAI Service, which utilizes GPT-4 capabilities, into its EHR. This next phase builds on that collaboration, introducing tools that support ambient notetaking, create clinical documentation summaries, and offer medical coding suggestions, all through generative AI. Epic is rolling out these services as it debuts its revamped third-party app market, which now hosts programs developed by Microsoft-owned Nuance as well as smaller startups.
The Gist: Given the massive datasets required to train these AI programs, the competition to deploy AI-powered healthcare workforce at scale will likely be driven by the largest tech and healthcare data companies rather than smaller start-ups.
Epic’s new app marketplace for third-party vendors is meant to ensure just that, by positioning it as the primary hub for many healthcare-specific AI programs in development.
Health systems will race to take advantage of the cost savings unlocked by these technologies, which they will hope integrate seamlessly into their EHRs.
As physicians stand to benefit from eased administrative burdens, but also have justified concerns over generative AI’s reliability, health systems should keep an open dialogue with frontline providers as they implement these new tools.
Generative AI applications can already help health systems improve margins, yet only 6% have a strategy ready.
At a Glance
In the wake of their most challenging financial year since 2020, US hospitals are desperately searching for margin improvements.
Generative AI can increase productivity and cost efficiency, but only 6% of health systems currently have a strategy.
Leading providers and payers will start with highly focused, low-risk generative AI use cases, generating the funds and experience for more transformative future applications.
While Covid-19 may no longer be dominating the global news cycle, healthcare providers and payers are still feeling its reverberations. More than half of US hospitals ended 2022 with a negative margin, marking the most difficult financial year since the start of the pandemic.
CEOs and CFOs remember the challenges all too well: The Omicron surge halted nonurgent procedures in the first half of the year, government support tapered off, and labor expenses ballooned amid staffing shortages. There was also the record-high inflation that continues to intensify margin pressures today. According to a recent Bain survey of health system executives, 60% cite rising costs as their greatest concern.
Payers and providers are now on the hunt for margin improvements. In our experience, the most successful companies won’t merely reduce costs, but also ramp up productivity. When done right, modest technology investments can accomplish both.
Artificial intelligence (AI) may hold part of the answer. With the costs to train a system down 1,000-fold since 2017, AI provides an arsenal of new productivity-enhancing tools at a low investment.
Many executives recognize the growing opportunity, especially with the recent rise of generative AI, which uses sophisticated large language models (LLMs) to create original text, images, and other content. It’s inspiring an explosion of ideas around use cases, from reviewing medical records for accuracy to making diagnoses and treatment recommendations.
Our survey reveals that 75% of health system executives believe generative AI has reached a turning point in its ability to reshape the industry. However, only 6% have an established generative AI strategy.
It’s time to play offense—or be forced to play defense later. But choosing from the laundry list of generative AI applications is daunting. Companies are at high risk of overinvesting in the wrong opportunities and underinvesting in the right ones, undermining future profitability, growth, and value creation. A wait-and-see approach is a tempting prospect.
However, we believe the next generation of leading healthcare companies will start today, with highly focused, low-risk use cases that boost productivity and cost efficiency. Over the next three to nine months, these companies will improve margins and learn how to implement a generative AI strategy, building up the funds and experience needed to invest in a more transformative vision.
Endless potential—and high hurdles
The excitement around generative AI may feel akin to the hype around other recent digital and technology developments that never quite rose to their promised potential. Well-intentioned, well-informed individuals are debating how much change will truly materialize in the next few years. While developments over the past six months have been a testament to the breakneck speed of change, nobody can accurately predict what the next six months, year, or decade will look like. Will new players emerge? Will we rely on different LLMs for different use cases, or will one dominate the landscape?
Despite the uncertainty, generative AI already has the power to alleviate some of providers’ biggest woes, which include rising costs and high inflation, clinician shortages, and physician burnout. Quick relief is critical, considering that the heightened risk of a recession will only compound margin pressures, and the US could be short 40,800 to 104,900 physicians by 2030, according to the Association of American Medical Colleges.
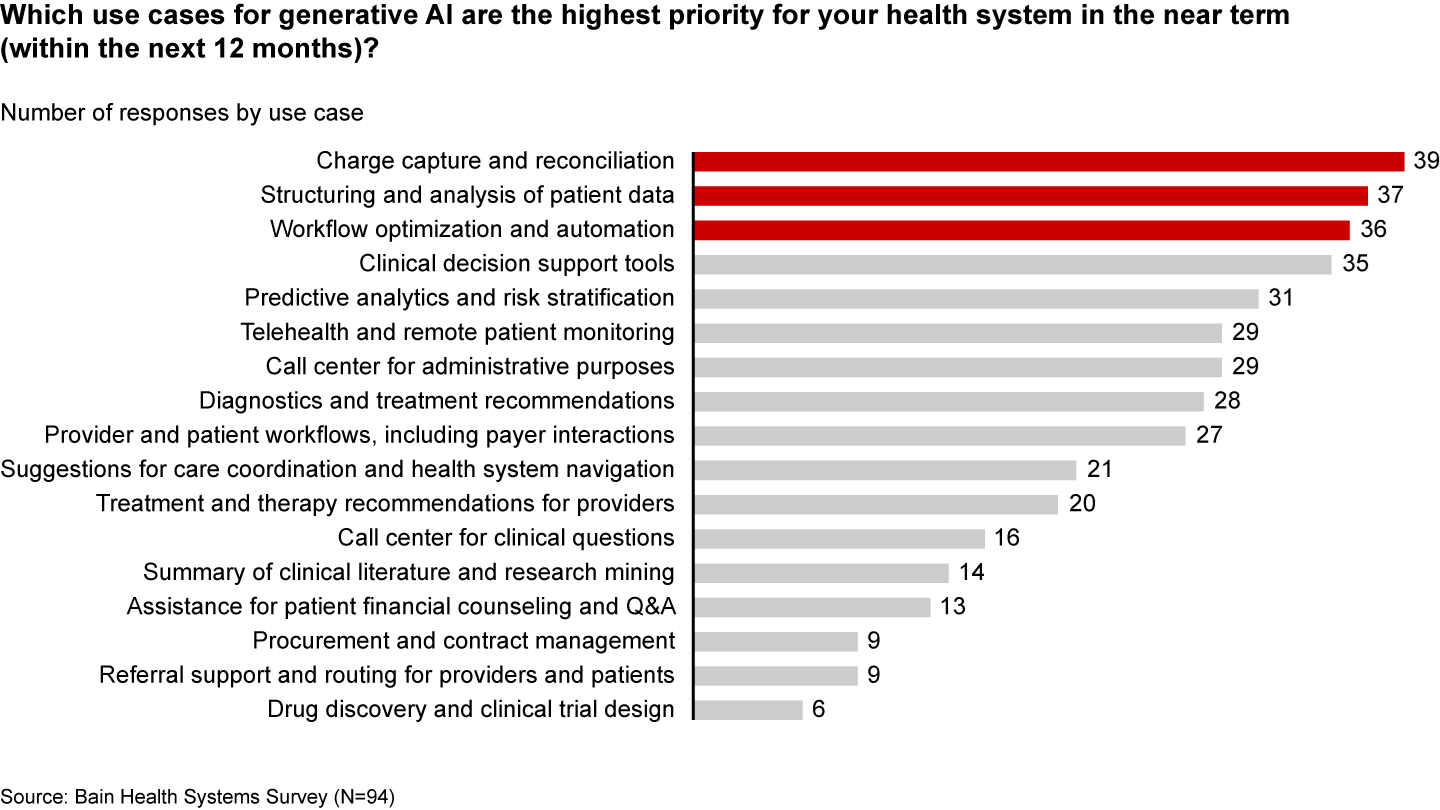
Many health systems are eyeing imminent opportunities to reduce administrative burdens and enhance operational efficiency. They rank improving clinical documentation, structuring and analyzing patient data, and optimizing workflows as their top three priorities (see Figure 1).
Figure 1
In the near term, generative AI can reduce administrative burdens and enhance efficiency
Some generative AI applications are already streamlining administrative tasks and allowing thinly stretched physicians to spend more time with patients. For instance, Doximity is rolling out a ChatGPT tool that can draft preauthorization and appeal letters. HCA Healthcare partnered with Parlance, a conversational AI-based switchboard, to improve its call center experience while reducing operators’ workload. And there are new announcements seemingly every week: Consider how healthcare software company Epic Systems is incorporating ChatGPT with electronic health records (EHRs) to draft response messages to patients, or how Google Cloud is launching an AI-enabled Claims Acceleration Suite for prior authorization processing.
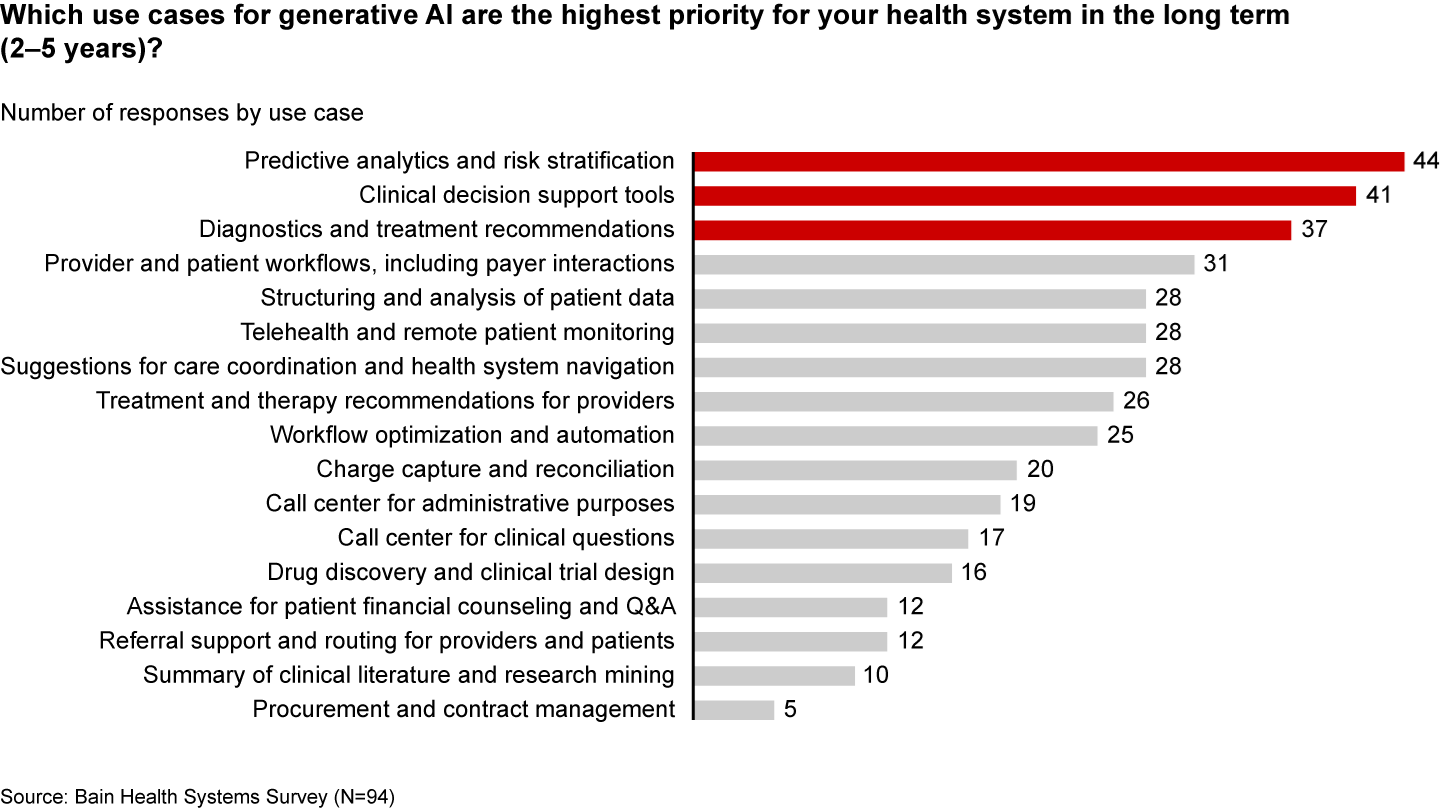
These applications only scratch the surface of potential. In the future, generative AI could profoundly transform care delivery and patient outcomes. Looking ahead two to five years, executives are most interested in predictive analytics, clinical decision support, and treatment recommendations (see Figure 2).
Figure 2
Predictive analytics, clinical decisions, and care recommendations are long-term generative AI priorities
It’s hard not to catch AI “fever.” But there are real challenges ahead. Some are already tackling the biggest questions: Organizations such as Duke Health, Stanford Medicine, Google, and Microsoft have formed the Coalition for Health AI to create guidelines for responsible AI systems. Even so, solutions to the greatest hurdles aren’t yet keeping up with the rapid technology development.
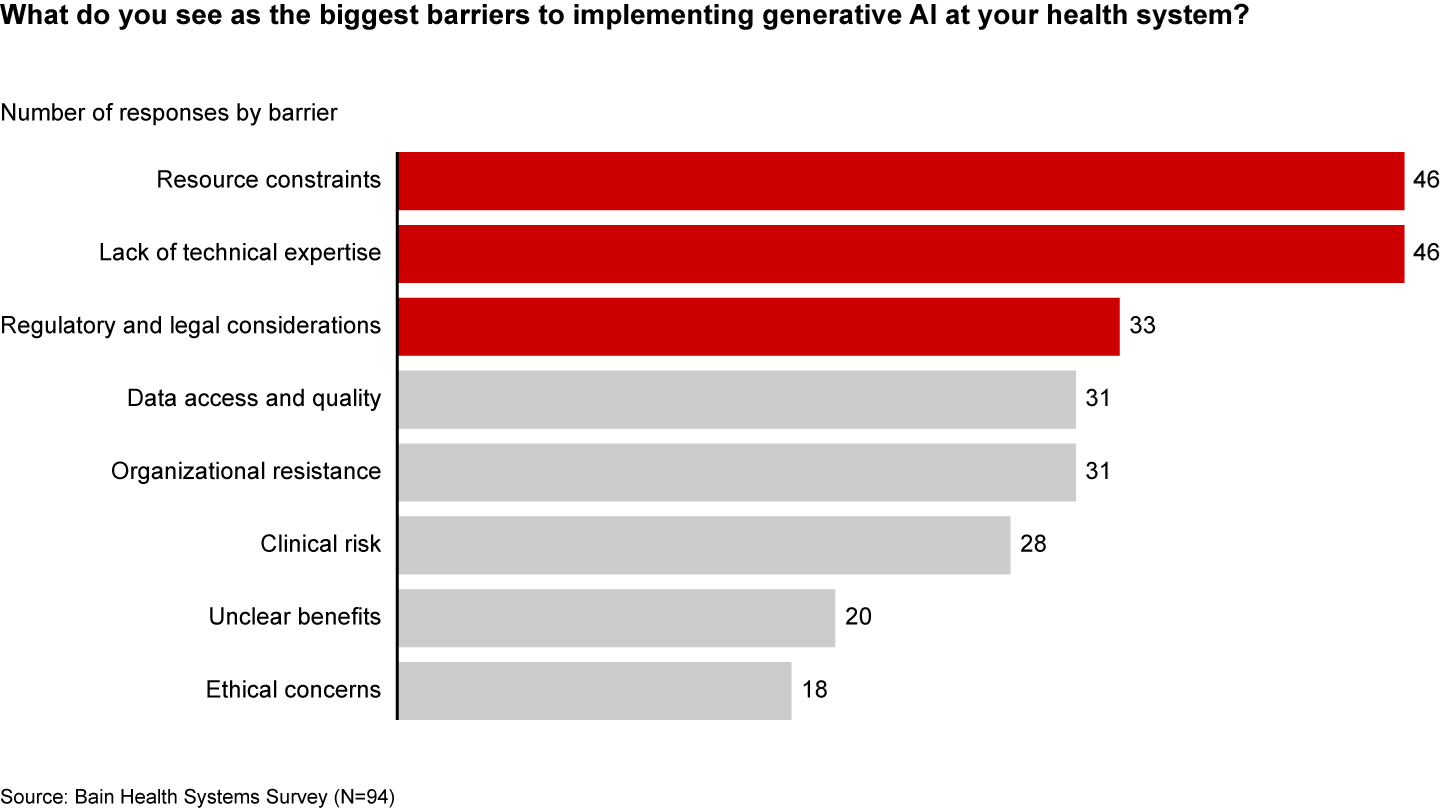
Resource and cost constraints, a lack of expertise, and regulatory and legal considerations are the largest barriers to implementing generative AI, according to executives (see Figure 3).
Figure 3
A lack of resources, expertise, and regulation are the biggest barriers to generative AI in healthcare
Even when organizations can overcome these hurdles, one major challenge remains: focus and prioritization. In many boardrooms, executives are debating overwhelming lists of potential generative AI investments, only to deem them incomplete or outdated given the dizzying pace of innovation. These protracted debates are a waste of precious organizational energy—and time.
Starting small to win big
Setting the bar too high is setting up for failure. It’s easy to get caught up, betting big on what seems like the greatest opportunity in the moment. But 12 months later, leaders often find themselves frustrated that they haven’t seen results or feeling as if they’ve made a misplaced bet. Momentum and investments slow, further hindering progress.
Leading companies are forming a more pragmatic strategy that considers current capabilities, regulations, and barriers to adoption. Their CEOs and CFOs work together to enforce four guiding principles:
Pilot low-risk applications with a narrow focus first. Tomorrow’s leaders are making no-regret moves to deliver savings and productivity enhancements in short order—at a time when they need it most. Gaining experience with currently available technology, they are testing and learning their way to minimum viable products in low-risk, repeatable use cases. These quick wins are typically in areas where they already have the right data, can create tight guardrails, and see a strong potential return on investment. Some, like call center and chatbot support, can improve the patient experience. However, given the current challenges around regulation and compliance, the most successful early initiatives are likely to be internally focused, such as billing or scheduling. Most importantly, executives prioritize initiatives by potential savings, value, and cost.
Decide to buy, partner, or build. CEOs will need to think about how to invest in different use cases based on availability of third-party technology and importance of the initiative.
Funnel cost savings and experience into bigger bets. As the technology matures and the value becomes clear, companies that generate savings, accumulate experience, and build organizational buy-in today will be best positioned for the next wave of more sophisticated, transformative use cases. These include higher-risk clinical activities with a greater need for accuracy due to ethical and regulatory considerations, such as clinical decision support, as well as administrative activities that require third-party integration, such as prior authorization.
Remember generative AI isn’t a strategy unto itself. To build a true competitive advantage, top CEOs and CFOs are selective and discerning, ensuring that every generative AI initiative reinforces and enables their overarching goals.
Some health systems are already seeing powerful results from relatively small, more practical investments. For instance, recognizing that clinicians were spending an extra 130 minutes per day outside of working hours on administrative tasks, the University of Kansas Health System partnered with Abridge, a generative AI platform, to reduce documentation burden. By summarizing the most important points from provider-patient conversations, Abridge is improving the quality and consistency of documentation, getting more patients in the door, and cutting down on pervasive physician burnout.
Although it will require some upfront investment, in the long run it will be more costly to underestimate the level and speed at which generative AI will transform healthcare. The next generation of leaders will start testing, learning, and saving today, putting them on a path to eventually revolutionize their businesses.
As first half 2023 financial results are reported and many prepare for a busy last half, strategic planning for healthcare services providers and insurers point to 4 issues requiring attention in every boardroom and C suite:
Private equity maturity wall:
The last half of 2023 (and into 2024) is a buyer’s market for global PE investments in healthcare services: 40% of PE investments in hospitals, medical groups and insurtech will hit their maturity wall in the next 12 months. Valuations of companies in these portfolios are below their targeted range; limited partner’ investing in PE funds is down 28% from pre-pandemic peak while fund raising by large, publicly traded, global funds dominate fund raising lifting PE dry powder to a record $3.7 trillion going into the last half of 2023.
In the U.S. healthcare services market, conditions favor well-capitalized big players—global private equity funds and large cap aggregators (i.e., Optum, CVS, Goldman Sachs, Blackstone et al) who have $1 trillion to invest in deals that enhance their platforms. Deals done via special purpose acquisition corporations (SPACS) and smaller PE funds in physicians, hospitals, ambulatory services and others are especially vulnerable. (see Bain and Pitchbook citations below). Addressing the growing role of large-cap PE and strategic investors as partners, collaborators, competitors or disruptors is table stakes for most organizations recognizing they have the wind at their backs.
Consolidation muscle by DOJ and FTC:
Healthcare is in the crosshair of the FTC and DOJ, especially hospitals and health insurers. Hospital markets have become increasingly concentrated: only 12% of the 306 Hospital Referral Regions is considered unconcentrated vs. 23% in 2008. In the 384 insurance markets, 23% are unconcentrated, down from 35% in 2020. Wages for healthcare workers are lower, prices for consumers are higher and choices fewer in concentrated markets prompting stricter guidelines announced last week by the oversight agencies. Big hospitals and big insurers are vulnerable to intensified scrutiny. (See Regulatory Action section below).
Defamatory attacks on nonprofit health systems:
In the past 3 years, private, not-for-profit multi-hospital systems have been targeted for excess profits, inadequate charity care and executive compensation. Labor unions (i.e., SEIU) and privately funded foundations (i.e., West, Arnold Venture, Lown Institute) have joined national health insurers in claims that NFP systems are price gaugers undeserving of the federal, state and local tax exemptions they enjoy. It comes at a time when faith in the U.S. health system is at a modern-day low (Gallup), healthcare access and affordability concerns among consumers are growing and hospital price transparency still lagging (36% are fully compliant with the 2021 Executive Order).
Notably, over the last 20 years, NFP hospitals have become less dominant as a share of all hospitals (61% in 2002 vs. 58% last year) while investor-owned hospitals have shown dramatic growth (from 15% in 2002 to 24% last year). Thus, the majority of local NFP hospitals have joined systems creating prominent brands and market dominance in most regions. But polling indicates many of these brands is more closely associated with “big business” than “not-for-profit health” so they’re soft targets for critics. It is likely unflattering attention to large, NFP systems will increase in the next 12 months prompting state and federal regulatory actions and erosion of public support. (See New England Journal citation in Quotables below)
Campaign 2024 healthcare rhetoric:
Republican candidates will claim healthcare is not affordable and blame Democrats. Democrats will counter that the Affordable Care Act’s expanded coverage and the Biden administration’s attack on drug prices (vis a vis the Inflation Reduction Act) illustrate their active attention to healthcare in contrast to the GOP’s less specific posturing.
Campaigns in both parties will call for increased regulation of hospitals, prescription drug manufacturers, health insurers and PBMs. All will cast the health industry as a cesspool for greed and corruption, decry its performance on equitable access, affordability, price transparency and improvements in the public’s health and herald its frontline workers (nurses, physicians et al) as innocent victims of a system run amuck.
To date, 16 candidates (12 R, 3 D, 1 I) have announced they’re candidates for the White House while campaigns for state and local office are also ramping up in 46 states where local, state and national elections are synced. Healthcare will figure prominently in all. In campaign season, healthcare is especially vulnerable to misinformation and hyper-attention to its bad actors. Until November 5, 2024, that’s reality.
My take:
These issues frame the near-term context for strategic planning in every sector of U.S. healthcare. They do not define the long-term destination of the system nor roles key sectors and organizations will play. That’s unknown.
What’s known for sure is that AI will modify up to 70% of the tasks in health delivery and financing and disrupt its workforce.
Black Swans like the pandemic will prompt attention to gaps in service delivery and inequities in access.
People will be sick, injured, die and be born.
And the economics of healthcare will force uncomfortable discussions about its value and performance.
In the U.S. system, attention to regulatory issues is a necessary investment by organizations in every state and at the federal level. Details about these efforts is readily accessible on websites for each organization’s trade group. They’re the rule changes, laws and administrative actions to which all are attentive. They’re today’s issues.
Less attention is given the long-term. That focus is often more academic than practical—much the same as Robert Oppenheimer’s early musings about the future of nuclear fusion. But the Manhattan Project produced two bombs (Little Boy and Fat Man) that detonated above the Japanese cities of Hiroshima and Nagasaki in 1945, triggering the end of World War II.
The four issues above should be treated as near and present dangers to the U.S. health system requiring attention in every organization. But responses to these do not define the future of the U.S. system. That’s the Manhattan Project that’s urgently needed in our system.
Pay attention to the media coverage around artificial intelligence, and it’s easy to get the sense that technologies such as chatbots pose an “existential crisis” to everything from the economy to democracy.
These threats are real, and proactive regulation is crucial. But it’s also important to highlight AI’s many positive applications, especially in health care.
Consider the Mayo Clinic, the largest integrated, nonprofit medical practice in the world, which has created more than 160 AI algorithms in cardiology, neurology, radiology and other specialties. Forty of those have already been deployed in patient care.
To better understand how AI is used in medicine, I spoke with John Halamka, a physician trained in medical informatics who is president of Mayo Clinic Platform. As he explained to me, “AI is just the simulation of human intelligence via machines.”
Halamka distinguished between predictive and generative AI. The former involves mathematical models that use patterns from the past to predict the future; the latter uses text or images to generate a sort of human-like interaction.
It’s that first type that’s most valuable to medicine today. As Halamka described, predictive AI can look at the experiences of millions of patients and their illnesses to help answer a simple question: “What can we do to ensure that you have the best journey possible with the fewest potholes along the way?”
For instance, let’s say someone is diagnosed with Type 2 diabetes. Instead of giving generic recommendations for anyone with the condition, an algorithm can predict the best care plan for that patient using their age, geography, racial and ethnic background, existing medical conditions and nutritional habits.
This kind of patient-centered treatment isn’t new; physicians have long been individualizing recommendations. So in this sense, predictive AI is just one more tool to aid in clinical decision-making.
The quality of the algorithm depends on the quantity and diversity of data. I was astounded to learn that the Mayo Clinic team has signed data-partnering agreements with clinical systems across the United States and globally, including in Canada, Brazil and Israel. By the end of 2023, Halamka expects the network of organizations to encompass more than 100 million patients whose medical records, with identifying information removed, will be used to improve care for others.
Predictive AI can also augment diagnoses. For example, to detect colon cancer, standard practice is for gastroenterologists to perform a colonoscopy and manually identify and remove precancerous polyps. But some studies estimate that 1 in 4 cancerous lesions are missed during screening colonoscopies.
Predictive AI can dramatically improve detection. The software has been “trained” to identify polyps by looking at many pictures of them, and when it detects one during the colonoscopy, it alerts the physician to take a closer look. One randomized controlled trial at eight centers in the United States, Britain and Italy found that using such AI reduced the miss rate of potentially cancerous lesions by more than half, from 32.4 percent to 15.5 percent.
Halamka made a provocative statement that within the next five years, it could be considered malpractice not to use AI in colorectal cancer screening.
But he was also careful to point out that “it’s not AI replacing a doctor, but AI augmenting a doctor to provide additional insight.” There is so much unmet need that technology won’t reduce the need for health-care providers; instead, he argued, “we’ll be able to see more patients and across more geographies.”
Generative AI, on the other hand, is a “completely different kind of animal,” Halamka said. Some tools, such as ChatGPT, are trained on un-curated materials found on the internet. Because the inputs themselves contain inaccurate information, the models can produce inappropriate and misleading text. Moreover, whereas the quality of predictive AI can be measured, generative AI models produce different answers to the same question each time, making validation more challenging.
At the moment, there are too many concerns over quality and accuracy for generative AI to direct clinical care. Still, it holds tremendous potential as a method to reduce administrative burden. Some clinics are already using apps that automatically transcribe a patient’s visit. Instead of creating the medical record from scratch, physicians would edit the transcript, saving them valuable time.
Though Halamka is clearly a proponent of AI’s use in medicine, he urges federal oversight. Just as the Food and Drug Administration vets new medications, there should be a process to independently validate algorithms and share results publicly. Moreover, Halamka is championing efforts to prevent the perpetuation of existing biases in health care in AI applications.
This is a cautious and thoughtful approach. Just like any tool, AI must be studied rigorously and deployed carefully, while heeding the warning to “first, do no harm.”
Nevertheless, AI holds incredible promise to make health care safer, more accessible and more equitable.