Congress cut billions of dollars in COVID-related funding from the broader government spending bill it just passed, jeopardizing President Biden’s plans for covering the costs of COVID testing and treatments, and making antiviral drugs available for free at pharmacies for those who test positive through the “test to treat” initiative.
However, a variety of other healthcare funding made it into the final package, including a five-month extension of COVID-era telehealth flexibilities for Medicare beneficiaries, and funds for pandemic preparedness. Congressional Democrats now plan to pass a separate COVID funding bill, although that effort will likely face stiff opposition from Senate Republicans.
The Gist: Removing COVID funding from the final spending package may signal the beginning of the end of federal pandemic relief spending, and could render the “test to treat” initiative, which has been praised by public health experts, dead on arrival.
Pharmacists, who have taken on a larger role in patient care during the pandemic, assisting with testing and vaccination of millions of Americans, have pushed for the ability to prescribe new antiviral therapies, but the American Medical Association criticized the initiative, maintaining that physicians should control the prescribing. Although the drug interactions and side effects cited by the AMA are important to manage, pharmacy-based “test to treat”would reduce time to treatment for those with COVID, and provide a sustainable mechanism for managing future surges of the disease.
The House passed a sweeping spending bill last night that omitted billions in Covid-19 aid. Biden administration officials had said the funds were urgently needed to maintain supplies of essential treatments and support further vaccine development, but Republicans disagreed. Some public health experts have expressed dismay that the pandemic relief money was cut, given the likelihood that new variants will continue to emerge. After all, viruses keep evolving until they run out of hosts to infect, and there are billions of people around the world—and millions in the US—who haven’t been vaccinated against Covid-19.
Cases continue to decline in the US, and a number of top voices in public health recently put out a report mapping when and how the country can transition out of the pandemic. Their recommendations include vaccinating at least 85 percent of the US population by 2023, improving indoor air quality in public buildings, and allocating additional funding for Covid-19 response and to prepare for future pandemics.
Welcome to Friday’s Health 202, where today we have a special spotlight on the pandemic two years in.
🚨 The federal government is about to be funded. The Senate sent the long-term spending bill to President Biden’s desk last night after months of intense negotiations.
Two years since the WHO declared a pandemic, what health-care system changes are here to stay?
Nurses screened patients at a drive-through testing site in March 2020. (Win McNamee/Getty Images)
Exactly two years ago, the World Health Organizationdeclared the coronavirus a pandemic and much of American life began grinding to a halt.
That’s when the health-care system, which has never been known for its quickness, sped up. The industry was forced to adapt, delivering virtual care and services outside of hospitals on the fly. Yet, the years-long pandemic has exposed decades-old cracks in the system, and galvanized efforts to fix them.
Today, as coronavirus cases plummet and President Biden says Americans can begin resuming their normal lives, we explore how the pandemic could fundamentally alter the health-care system for good. What changes are here to stay — and what barriers are standing in the way?
A telehealth boom
What happened: Telehealth services skyrocketed as doctors’ offices limited in-person visits amid the pandemic. The official declaration of a public health emergency eased long-standing restrictions on these virtual services, vastly expanding Medicare coverage.
But will it stick? Some of these changes go away whenever the Biden administration decides not to renew the public health emergency (PHE). The government funding bill passed yesterday extends key services roughly five months after the PHE ends, such as letting those on Medicare access telehealth services even if they live outside a rural area.
But some lobbyists and lawmakers are pushing hard to make such changes permanent. Though the issue is bipartisan and popular, it could be challenging to pass unless the measures are attached to a must-pass piece of legislation.
“Even just talking to colleagues, I used to have to spend three or four minutes while they were trying desperately not to stare at their phone and explain to them what telehealth was … remote patient monitoring, originating sites, and all this wonky stuff,”said Sen. Brian Schatz (D-Hawaii), a longtime proponent of telehealth.
“Now I can go up to them and say, ‘So telehealth is great, right?’ And they say, ‘yes, it is.’ ”
A new spotlight on in-home care
What happened: The infectious virus tore through nursing homes, where often fragile residents share rooms and depend on caregivers for daily tasks. Ultimately, nearly 152,000 residents died from covid-19.
The devastation has sparked a rethinking of where older adults live and how they get the services they need — particularly inside their own homes.
“That is clearly what people prefer,” said Gail Wilensky, an economist at Project HOPE who directed the Medicare and Medicaid programs under President George H.W. Bush. “The challenge is whether or not it’s economically feasible to have that happen.”
More money, please: Finding in-home care — and paying for it — is still a struggle for many Americans. Meanwhile, many states have lengthy waitlists for such services under Medicaid.
Experts say an infusion of federal funds is needed to give seniors and those with disabilities more options for care outside of nursing homes and assisted-living facilities.
For instance, Biden’s massive social spending bill included tens of billions of dollars for such services. But the effort has languished on Capitol Hill, making it unclear when and whether additional investments will come.
A reckoning on racial disparities
What happened: Hispanic, Black, and American Indian and Alaska Native people are about twice as likely to die from covid-19 than White people. That’s according to age-adjusted data from a recent Kaiser Family Foundation report.
In short, the coronavirus exposed the glaring inequities in the health-care system.
“The first thing to deal with any problem is awareness,” said Georges Benjamin, the executive director of the American Public Health Association. “Nobody can say that they’re not aware of it anymore, that it doesn’t exist.”
But will change come? Health experts say they hope the country has reached a tipping point in the last two years. And yet, any real systemic change will likely take time. But, Benjamin said, it can start with increasing the number of practitioners from diverse communities, making office practices more welcoming and understanding biases.
We need to, as a matter of course, ask ourselves who’s advantaged and who’s disadvantaged” when crafting new initiatives, like drive-through testing sites, Benjamin said. “And then how do we create systems so that the people that are disadvantaged have the same opportunity.”
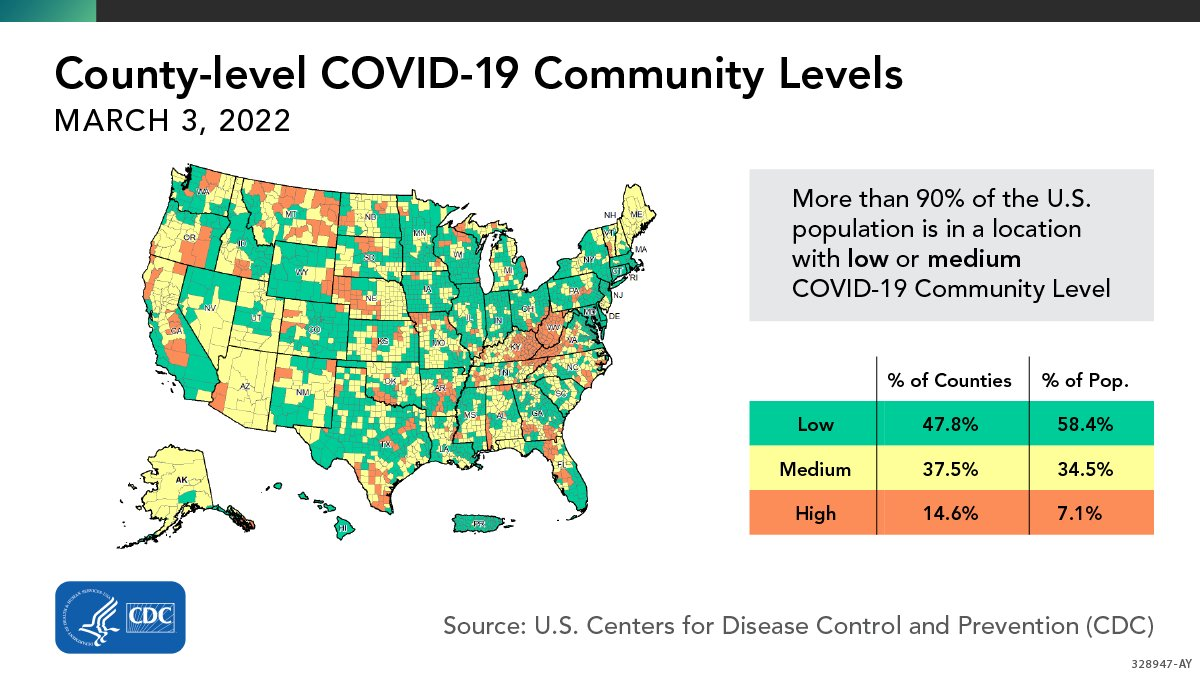
More than 90% of the U.S. population lives in an area with a “low” or “medium” risk of COVID-19, the U.S. Centers for Disease Control and Prevention (CDC) announced yesterday. Last week, the CDC changed the way it assesses county-level COVID-19 risk, using data on hospitalizations and health care capacity in addition to case counts. The CDC now recommends universal indoor masking only for counties that are at “high” risk under this system—which means that the vast majority of Americans are not currently advised to wear masks inside.
In May 2020, a 33-year-old mother of three in North Carolina started experiencing symptoms of COVID-19. Four days later, a different set of symptoms set in. She stopped sleeping well and started having paranoid delusions that people were tracking her through her cell phone—culminating in a frantic scene at a fast-food restaurant, in which she tried to pass her children through the drive-through window, where they’d be safe from the phones and other dangers.
A restaurant employee called 911, and emergency medical services workers arrived, gathered up the family, and hurried to the nearby emergency department of the Duke University Medical Center in Durham, where the mother was quickly attended to by physicians. “She was physically in the room, but she wasn’t making consistent eye contact,” says Dr. Colin Smith, who is now chief resident of the hospital’s internal medicine psychiatry program but was a second-year resident when he took care of the patient. “She was not really engaging all that much. Her thought processes were disorganized.”
Despite that, the patient acknowledged two things to Smith and the other doctors: She knew her behavior was out of character, and the changes all happened quickly after she was diagnosed with COVID-19.
There’s growing evidence that COVID-19 and new psychotic episodes are connected. The North Carolina case, reported in the British Medical Journal in August 2020, joins a slew of case reports published in medical journals during the pandemic that detail psychotic episodes following a COVID-19 diagnosis. In the July 2020 issue of BJPsyh Open, researchers reported that a 55-year old woman in the U.K., with no history of mental illness, arrived at a hospital days after recovering from a severe case of COVID-19 with delusions and hallucinations, convinced that the nurses were devils in disguise and that monkeys were jumping out of the doctors’ medical bags. In April 2021, other researchers wrote in BMJ Case Reports of a middle-aged British man, also with no prior mental health disorders, who had appeared at a London hospital experiencing auditory and visual hallucinations and banging his head against walls until he bruised his skin. (Weeks before, he had recovered from a bout with COVID-19 that had landed him in the intensive care unit.) In yet another case, published in the Journal of Psychiatric Practice in March 2021, a 57-year-old-man turned up at Columbia University’s New York Presbyterian Hospital insisting that his wife was poisoning him, that cameras had been planted throughout his apartment, and that the patients in the hospital’s emergency department were being secretly murdered.
“The situation was strikingly similar to one we’d expect from someone who had a schizophrenia spectrum illness,” says Dr. Aaron Slan, now a fourth-year psychiatry resident at Columbia University, who cared for the patient and co-authored the report. But this patient too had no history of mental health disorders and was too old for a first-onset case of schizophrenia, which typically occurs between ages 20 and 30 for men, Slan notes. What the patient did have, as a test in the hospital revealed, was COVID-19.
COVID-19-related psychotic breaks are rare—though researchers say that it’s too early to say exactly how rare—and plenty of experts believe that the connection between the two conditions, if any, is not causal. In a review published in 2021 in Neurological Letters, a group of researchers in the U.K. casts doubt on the emerging body of work on the COVID-19-psychosis link as “beset by both small sample size, and inadequate attention to potential confounding factors,” such as heightened stress, substance abuse, and socioeconomic hardship.
Still, researchers are investigating the link. One U.K. study published in the Lancet in October 2020 found that of 153 people who were diagnosed with COVID-19 early in the pandemic, 10 suffered new-onset psychotic episodes following their COVID-19 diagnosis, and seven exhibited the onset of psychiatric disorders, including catatonia and mania.
A study published last August in General Hospital Psychiatry took a broad view of the phenomenon, analyzing 40 scientific articles, which included 48 adults from 17 different countries who suffered psychotic episodes associated with COVID-19 infection, and tried to find commonalities among them. As with the Neurological Letters paper, the authors of this study found plenty of other variables that might muddy the link between COVID-19 and psychosis—like stress, substance use, and medications—but the relationship still held.
“We see post-infectious neuroinflammatory disorders associated with a variety of different viral illnesses,” says Dr. Samuel Pleasure, a neurology professor at the University of California, San Francisco (UCSF). “Normally we see it in very small numbers, but here we have [COVID-19] infecting tens of millions of people at the same time.” Even rare cases of psychiatric conditions will start to show themselves when the sample group of infected people is so large.
There are more questions than answers at this point. It’s still unclear whether the severity of COVID-19 symptoms plays any role in the likelihood of a psychotic break. “There seem to be clearly cases of neuropsychiatric consequences of COVID that are linked to cases that are not severe,” Pleasure says. “I believe that the quality of the studies at this point are so preliminary, and the ability to really capture these patients to study is really at early stages, so it’s hard to be definitive.” Similarly, Pleasure says, it’s impossible to say whether people suffering from Long COVID—symptoms that last for months after the infection is over—are more susceptible to psychotic symptoms.
There are multiple possible mechanisms at work, any one of which—or a combination—could be contributing to the neuropsychiatric symptoms associated with COVID-19. The most straightforward would be direct infection of brain tissue itself, according to Pleasure. If that’s so, the number of COVID-19 patients who suffer loss of the sense of taste and smell would suggest that the brain’s olfactory bulb may be struck by the virus first.
“There are documented cases where people have done MRIs early in the [COVID-19 disease] process and have seen some local inflammation in the olfactory bulb,” Pleasure says. “That has contributed further to the idea that maybe that’s the portal of entry.” Once that portal has been breached, the brain at large could be exposed.
Just how the COVID-19 infection reaches the brain is unclear, but Pleasure and his colleague Dr. Michael Wilson, associate professor of neurology at UCSF, conducted lumbar punctures of three teens with COVID-19 who had developed neuropsychiatric symptoms to examine their cerebrospinal fluid. In two cases, they found antibodies in the fluid that target neural antigens. That presented an apparent puzzle: the patients had SARS-CoV-2; if anything, they should be exhibiting antibodies to the virus, not to their own neural tissue. But Pleasure cites one study he conducted with a group from Yale University showing that antibodies specific to the coronavirus spike protein could also cross-react with nerve cells, attacking them as well.
“There was molecular mimicry between the spike protein and a neural antigen,” he says. “One of the main hypotheses is that if there’s an antibody that targets the virus, then, out of bad luck, you also see damage to the host.” In other words, he says, you start with an immune response adaptive to fighting the virus, and that turns into an autoimmune response.
That’s just one theory. There are still other routes by which COVID-19 can affect the brain. Upper respiratory infections can, on occasion, cause the immune system to go awry and develop antibodies against parts of the brain known as NMDA (N-methyl-D-aspartate) receptors, which are the main excitatory receptors that react to neurotransmitters. A broad attack on receptors spread throughout the brain can lead to quick and severe symptoms, says Dr. Mudasir Firdosi, a Consultant Psychiatrist at the Kent and Medway NHS and Social Care Partnership Trust and a co-author of the 2021 BMJ paper.
“[NMDA involvement] presents a very, very florid way to be psychotic,” Firdosi says. Slan agrees: “When someone has an abrupt onset of psychosis following a viral illness, NMDA antibodies are frequently invoked,” he says.
Yet another suspect in the development of neuropsychiatric symptoms is the so-called cytokine storm that often follows infection with SARS-CoV-2. Cytokines are proteins critical for cell signaling that are produced by the immune system and give rise to inflammation that in turn can fight infection. But if cytokine production spins out of control, extreme body-wide inflammation can follow, and brain tissue would not be spared the impact.
“The neurons themselves are not being invaded,” says Slan, “but what happens is that the systemic inflammatory response causes both stress and changes in signaling throughout the body. That includes the brain, and can precipitate these types of [psychotic] symptoms.”
One other bit of evidence that COVID-19 is linked to psychotic breaks comes not from the current scientific literature, but from history. Following the influenza pandemic of 1918 and 1919, there was a spike in what was called encephalitis lethargica, which was essentially a form of early-onset Parkinson’s disease that often didn’t appear for a number of years after the infection—but left patients in what was effectively a state of catatonia.
“That flu virus caused a post-infection inflammation that killed brain cells that in turn led to the Parkinson’s,” says Pleasure. The book and movie Awakenings, about patients who temporarily recovered consciousness and lucidity after treatment with l-dopa—a precursor of the neurotransmitter dopamine—was based on cases of people suffering from that form of Parkinson’s.
The good news is that unlike more chronic forms of psychosis, most cases seemingly related to COVID-19 do not appear to last. The symptoms can respond to antipsychotic medications like Risperdal (risperidone) and Zyprexa (olanzapine), say Smith and Slan. Intravenous immunoglobulin infusions—which reduce the overall load of abnormal cells and inflammatory agents—and steroids, which also reduce inflammation, can be effective as well.
By no means is the case for virus-triggered psychosis closed. Even Slan, who has first-hand experience treating a patient suffering from a seemingly virus-linked psychotic break believes that there is more work to be done—and acknowledges the doubts of the researchers who believe other psychological factors might be at play.
“Given the stress of COVID,” he says, “given the concerns about mortality, seclusion, all of these things represent huge psychosocial stressors, and they have the potential to precipitate oftentimes short-lived psychotic symptoms.”
Of course, even a transitory psychosis is still a psychosis—something no one wants to experience even fleetingly. That puts a premium on avoiding infection in the first place. “The best way to treat COVID-19 and the risk of psychosis is to prevent it,” says Smith. “Even if neurological complications are rare, getting vaccinated remains the smartest choice.”
As COVID-19 cases fall and hospitals tiptoe out from yet another surge, the nation is left collectively asking one major question: What comes next?
By now, health experts have made it clear COVID-19 will always be around in some capacity but have stressed uncertainty about the potential scope and severity of future surges.
While difficult to predict what the pandemic’s next act could look like, several potential scenarios have emerged in recent months.
Below are four possible paths the pandemic could take in the future, as outlined by physicians, epidemiologists and global health officials:
1. Delta rebound. Delta has seemingly fallen out of the collective pandemic lingo amid omicron’s dominance in recent months, though there is still a chance delta — thought to be the deadliest strain thus far — makes a comeback.
In a Jan. 24 op-ed for The Washington Post, Ashish Jha, MD, dean of Brown University’s School of Public Health in Providence, R.I., said “It is possible, though unlikely, that the delta variant returns and co-circulates with omicron in different populations, contributing to ongoing infections and hospitalizations.”
It’s important to note that delta is still dominant in some parts of the world, health experts toldThe Atlantic, adding that while unlikely, there is a chance it could morph into something that catches up with omicron, allowing the two to tag-team — a dangerous combination given delta’s brutality and omicron’s transmissibility.
2. COVID-19 may become a seasonal virus. Dr. Jha said this scenario is likely, whether delta makes a comeback or not.
“That means we are likely to see surges in Southern states this summer (as people there spend more time indoors) and in Northern states next fall and winter as the weather turns cold again,” he wrote in a Jan. 24 op-ed for The Washington Post.
Emerging evidence suggests COVID-19 may be a seasonal disease, though the research is still preliminary. A July 2021 study from the University of Pittsburgh projected a seasonal COVID-19 pattern in North America with three repeating waves: one starting in New England in the spring, the second starting in the South in the summer, and the third kicking off in the Dakotas in the fall. Based on these findings, researchers predicted the U.S. would see a summer 2021 wave in the South and a fall 2021 wave in North-Central states, which is similar to what happened with the delta and omicron surges. As of November 2021, the study had not been peer reviewed.
3. A new variant emerges. If there’s one thing on this list that’s near certain, it’s that there will be new variants in the future. Global health officials have said they expect future variants to be even more transmissible than omicron.
“Omicron will not be the last variant that you will hear us talking about,” Maria Van Kerkhove, PhD, the World Health Organization’s technical lead on COVID-19, said Jan. 25. “The next variant of concern will be more fit, and what we mean by that is it will be more transmissible, because it will have to overtake what is currently circulating.”
Health officials aren’t so much concerned about the emergence of new variants themselves but whether they will cause more or less disease severity. WHO officials have warned against assuming the virus will become milder as it continues to mutate.
“There is no guarantee of that,” Dr. Van Kerkhove said. “We hope that is the case, but there is no guarantee of that and we can’t bank on it,” she added, emphasizing the importance of interventions such as ramping up global vaccination coverage to prevent the emergence of new variants.
Health experts are also concerned white-tailed deer may become a reservoir for the virus to mutate and spread to other animals or back to humans in the form of a new variant.
“This is a top concern right now for the United States,” said Casey Barton Behravesh, who directs the CDC’s One Health Office, which focuses on connections among human, animal and environmental health. “If deer were to become established as a North American wildlife reservoir — and we do think they’re at risk of that — there are real concerns for the health of other wildlife species, livestock, pets and even people,” she told The New York Times.
Preliminary findings recently found white-tailed deer on New York’s Staten Island infected with omicron, the first time the strain has been detected in wild animals in the U.S. Scientists are still exploring a number of questions regarding the virus’s spread among deer, such as how they contract the virus, how the pathogen might mutate inside the host, and whether deer could pass the virus back to humans.
4. The omicron subvariant may spread globally, prolonging the current COVID-19 surge in some parts of the world.
Research shows BA.2 is more transmissible than BA.1, the original omicron strain, though there is no evidence to suggest the subvariant causes more severe illness. The WHO said it expects cases of the omicron subvariant to increase globally due to its growth advantage over BA.1.
“We expect to see BA.2 increasing in detection around the world,” Dr. Kerkhove said during a Feb. 8 media briefing.
In late January, Nathan Grubaugh, PhD, an epidemiologist at the Yale University School of Public Health in New Haven, Conn., toldThe New York Times he was “fairly certain” the subvariant will become dominant in the U.S. but is unclear on “what that would mean for the pandemic.”
The BA.2 variant could spur a new surge, but it’s more likely that U.S. cases will continue to decrease, according to Dr. Grubaugh. If anything, the variant may simply slow the decline.
Overall, most experts told the Times that BA.2’s presence would not significantly alter the course of the pandemic, and so far, data backs this up. COVID-19 cases have been falling nationwide since peaking in mid-January, and modeling from Rochester, Minn.-based Mayo Clinic predicts this trend will continue over the next 14 days.
The weekly number of BA.2 sequences identified in the U.S. has also fallen since mid-January, according to a Feb. 11 U.K. Health Security Agency’s report. The U.S. confirmed 191 BA.2 sequences in the week of Jan. 17, which fell to 116 in the week of Jan. 24. In the week of Jan. 31, just four sequences were confirmed, according to supplemental data from the report.
The U.S. may see an end to all pandemic restrictions, including mandatory mask-wearing, in the coming months, Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, told the Financial Times Feb. 8.
He said he hopes that the end to these restrictions will come soon and explained that the response to the pandemic going forward will be concentrated at a local level.
“As we get out of the full-blown pandemic phase of COVID-19, which we are certainly heading out of, these decisions will increasingly be made on a local level rather than centrally decided or mandated. There will also be more people making their own decisions on how they want to deal with the virus,” he told the FT.
The National Institute for Allergy and Infectious Diseases is preparing for the next pandemic by monitoring viruses that are known to cause severe illness.
Data from federal, state, and local health agencies show COVID-19 case, hospitalization, and death rates are much lower for vaccinated Americans than they are for the unvaccinated.
The first week of December 2021, when Omicron was first detected in the US, unvaccinated adults were nearly 25 times more likely to be hospitalized than vaccinated adults. While Omicron caused a big spike in COVID-19 cases, vaccinated people continued to be less likely to be hospitalized than the unvaccinated.
In King County, Wash., which includes Seattle, unvaccinated people were 13 times more likely to be hospitalized for coronavirus since December than people who were fully vaccinated.
New York City was one of the first areas in the US to get hit with Omicron. During the week ending January 15, 0.6% of all unvaccinated people were hospitalized with COVID-19 , compared with 0.02% of all vaccinated people.
These two areas have some of the most up-to-date data that illustrates the differences in susceptibility and severity of coronavirus based on vaccination status. But other state and local health agencies as well as the Centers for Disease Control and Prevention (CDC) also provide data that shows vaccine effectiveness.
As of January 26, 210 million Americans, or 64% of the population, were considered fully vaccinated after completing the initial series of COVID-19 shots. Twenty-six percent of Americans had received a booster dose.
National data isn’t as recent but shows lower hospitalization risks among the boosted.
CDC data compiled from hospitals in 12 states shows that, in the week before Christmas, unvaccinated people ages 50 to 64 were 32 times more likely to be hospitalized with COVID-19 than people in the age range who got a booster shot. They were eight times more likely to be hospitalized with COVID-19 than fully vaccinated people without a booster.
Unvaccinated people 65 and older were about 50 times more likely to be hospitalized than those who were fully vaccinated and received a booster.
More recent data from across the country suggests vaccinated people continue to experience lower hospitalization rates.
Georgia and North Dakota are two states publishing recent data on hospitalizations for people who have received a booster shot.
These comparisons do not account for age, so they don’t directly show the effectiveness of boosters. But the available data suggests vaccinated people are hospitalized at lower rates than unvaccinated people, just like before the Omicron wave.
In the first week of December, the combination of Georgia’s unvaccinated population and those receiving only one dose of the vaccine were 10 times more likely to be in a hospital with COVID-19 than the boosted population.
Georgia counts anyone in a hospital who tests positive for COVID-19 as a COVID-19 hospitalization.
Hospitalization rates in the state increased for everyone regardless of vaccination status during the Omicron wave. But the gap between the boosted population and the unvaccinated or partially vaccinated remained.
As of mid-January, the weekly hospitalization rate for Georgia’s booster group was a third of the rate for the combined unvaccinated and not fully vaccinated population. As of January 31, 48% of Georgians were not fully vaccinated, while 17% had received a booster.
During the same period in North Dakota, unvaccinated and partially vaccinated people were about twice as likely to be hospitalized with COVID-19 compared with the vaccinated. The hospitalization gap was three times greater for those with boosters.
Several other states published data on hospitalizations through mid-January. They all show vaccinated Americans at much lower risk.
Covid-19 death rates in the United States are “eye-wateringly” high compared with other wealthy nations—a problem that several health experts say underscores the shortfalls of the country’s pandemic response.
U.S. Covid-19 death rates exceed those of other wealthy nations
According to CDC data, over 880,000 Americans have died from Covid-19 since the beginning of the pandemic—a death toll greater than that of any other country. And during the current omicron wave, Covid-19 deaths are now greater than the peak number seen during the delta wave and more than two-thirds as high as record numbers seen last winter before vaccines were available, the New York Times reports.
Moreover, since Dec. 1, when omicron was first detected in the United States, the proportion of Americans who have died from Covid-19 has been at least 63% higher than other large, wealthy countries, including Britain, Canada, France, and Germany, according to a Times analysis of mortality figures.
Currently, the daily Covid-19 death rate in the United States is nearly double that of Britain and four times that of Germany. The only large European countries to surpass the United States’ Covid-19 death rates have been the Czech Republic, Greece, Poland, Russian, and Ukraine—all of which are less wealthy nations where the most effective treatments may be limited.
“Death rates are so high in the States—eye-wateringly high,” said Devi Sridhar, head of the global public health program at the University of Edinburgh. “The United States is lagging.”
Similarly, Joseph Dieleman, an associate professor at the University of Washington, said the United States “stands out” with its high Covid-19 death rate. “There’s been more loss than anyone wanted or anticipated,” he said.
Vaccination shortfalls plague the U.S.
Lagging Covid-19 vaccination rates among Americans likely contributed to the country’s outsized death toll compared with other nations, several health experts said.
Currently, around 64% of the U.S. population has been fully vaccinated. However, several peer countries, including Australia (80%), Canada (80%), and France (77%), have achieved higher vaccination rates.
Unvaccinated people make up the majority of hospitalized Covid-19 patients, according to the Times, but lagging vaccination and booster rates among vulnerable groups, such as older Americans, has also led to increased hospitalizations.
Around 12% of Americans ages 65 and older are not fully vaccinated, and among those who are fully vaccinated, 43% still have not received a booster shot, leaving them with waning immunity against the omicron variant. In comparison, only 4% of Britons ages 65 and older are not fully vaccinated, and only 9% have not had a booster shot.
“It’s not just vaccination—it’s the recency of vaccines, it’s whether or not people have been boosted, and also whether or not people have been infected in the past,” said Lauren Ancel Meyers, director of the University of Texas at Austin’s Covid-19 modeling consortium.
Similarly, former FDA Commissioner Scott Gottlieb said that the United States‘ lagging vaccination rates compared to the U.K.’s, particularly for boosters, may be due to “protracted wrangling” that “may have sowed confusion, sapping consumer interest.”
How the U.S. could fare in future Covid-19 waves
According to some scientists, the gap between the United States and other wealthy nations may soon begin to narrow. Although U.S. vaccination rates have been slow, the delta and omicron waves have infected so many people that overall immunity against the coronavirus has increased—which could potentially help blunt the effect of future waves.
“We’ve finally started getting to a stage where most of the population has been exposed either to a vaccine or the virus multiple times by now,” said David Dowdy, an epidemiologist at the Johns Hopkins Bloomberg School of Public Health. “I think we’re now likely to start seeing [American and European Covid-19 death rates] be more synchronized going forward.”
However, other experts noted that the United States has other disadvantages that could make future Covid-19 waves difficult. For example, many Americans have chronic health problems, such as diabetes and obesity, that increase the risk of severe Covid-19 outcomes.
Overall, health experts said the impact of future Covid-19 waves will depend on what new variants emerge, as well as what level of death people decide is tolerable.
“We’ve normalized a very high death toll in the U.S.,” said Anne Sosin, who studies health equity at Dartmouth University. “If we want to declare the end of the pandemic right now, what we’re doing is normalizing a very high rate of death.”
The Food and Drug Administration fully approved Moderna’s mRNA COVID-19 vaccine on Monday, saying it meets its safety and manufacturing requirements.
Why it matters: Moderna’s vaccine, which will now be marketed as Spikevax, is the second coronavirus vaccine to receive full approval after the FDA approved Pfizer-BioNTech’s vaccine in August.
Hundreds of millions of doses of Moderna’s vaccine have already been administered in the U.S. under the FDA’s emergency use authorization.
What they’re saying: “The public can be assured that Spikevax meets the FDA’s high standards for safety, effectiveness and manufacturing quality required of any vaccine approved for use in the United States,” acting FDA Commissioner Janet Woodcock said in a statement.
“The totality of real-world data and the full [Biologics License Application] for Spikevax in the United States reaffirms the importance of vaccination against this virus,” Moderna CEO Stéphane Bancel said.
The big picture: The rise of the Omicron variant forced vaccine makers to reevaluate the effectiveness of their vaccines, which were developed based on eaarlier forms of the virus.
Studies show that Moderna and Pfizer-BioNTech’s vaccines still overwhelmingly prevent severe disease and hospitalizations, especially when the first two doses are reinforced with a booster shot.