With a 51-50 vote, Senate Democrats passed a sweeping $739 billion bill Aug. 7 that furthers some of the largest changes to healthcare in years.
Titled the Inflation Reduction Act, the bill touches energy, tax reform and healthcare. The House is expected to take it up Aug. 12, with Democrats aiming to approve it and send it to President Joe Biden’s desk.
Here are seven healthcare takeaways from the 755-page bill:
Drug pricing
1. For the first time, Medicare would be allowed to negotiate the price of prescription medicines with manufacturers. Negotiation powers will apply to the price of a limited number of drugs that incrementally increases over the next seven years. Ten drugs will be eligible for negotiations beginning in 2026; eligibility expands to 15 drugs in 2027 and 20 by 2029.
2. The HHS secretary will provide manufacturers of selected drugs with a written initial offer that contains HHS’ proposal for the maximum fair price of the drug and reasoning used to calculate that offer. Manufacturers will have 30 days to either accept HHS’ offer or propose a counteroffer.
3. Members of Medicare Part D prescription drug plan would see their out-of-pocket costs for prescription drugs capped at $2,000 per year, with the option to break that amount into monthly payments, beginning in 2025.
4. Democrats lost on a provision to place a $35 cap on insulin for Americans covered by private health plans. The provision to cap insulin at $35 dollars for Medicare enrollees passed by a of 57-43.
5. Drug companies will be required to rebate back price differences to Medicare if they raise prices higher than the rate of inflation, coined an “inflation rebate.”
6. The legislation makes all vaccines covered under Medicare Part D free to beneficiaries with no deductibles, co-insurance or cost-sharing, starting in 2023.
Tax subsidies
7. The legislation extends the Affordable Care Act’s federal health insurance subsidies, now set to expire at the end of the year, through 2025. Democrats say the extension will prevent an estimated 3.4 million Americans from losing health coverage.
Hospitals are forced to absorb inflationary expenses, particularly related to supporting their workforce, AHA says.
The Centers for Medicare and Medicaid Services’ increase in the inpatient payment rate for 2023 is welcome but not enough to offset expenses, according to the American Hospital Association.
CMS set a 4.1% market basket update for 2023 in its final rule released Monday, calling it the highest in the last 25 years. The increase was due to the higher cost in compensation for hospital workers.
The final rule gave inpatient hospitals a 4.3% increase for 2023, as opposed to the 3.2% increase in April’s proposed rule.
WHY THIS MATTERS
CMS used more recent data to calculate the market basket and disproportionate share hospital payments, a move that better reflects inflation and labor and supply cost pressures on hospitals, the AHA said.
“That said, this update still falls short of what hospitals and health systems need to continue to overcome the many challenges that threaten their ability to care for patients and provide essential services for their communities,” said AHA Executive Vice President Stacey Hughes. “This includes the extraordinary inflationary expenses in the cost of caring hospitals are being forced to absorb, particularly related to supporting their workforce while experiencing severe staff shortages.”
The AHA would continue to urge Congress to take action to support the hospital field, including by extending the low-volume adjustment and Medicare-dependent hospital programs, Hughes said.
In late July, Senate and House members urged CMS to increase the inpatient hospital payment.
Premier, which works with hospitals, also said the 4.3% payment update falls short of reflecting the rising labor costs that hospitals have experienced since the onset of the pandemic.
“Coupled with record high inflation, this inadequate payment bump will only exacerbate the intense financial pressure on American hospitals,” said Soumi Saha, senior vice president of Government Affairs for Premier.
THE LARGER TREND
Recent studies show hospitals remain financially challenged since the COVID-19 pandemic’s effect on revenue and supply chain and labor expenses. Piled onto that has been inflation that has added to soaring expenses.
Hospital margins were up slightly from May to June, but are still significantly lower than pre-pandemic levels, according to a Flash Report from Kaufman Hall.
The effects of the pandemic on the healthcare industry have been profound, resulting in the creation of new business models, according to a report from McKinsey.
Transformational change is necessary as hospitals have been hit hard by eroding margins due to cost inflation and expenses, Fitch found.
The national uninsured rate reached an all-time low of 8 percent in the first quarter of 2022, according to an HHS report released Aug. 2.
The report analyzed data from the National Health Interview Survey and the American Community Survey, according to an Aug. 2 HHS news release.
Three things to know:
1. The previous record low uninsured rate was 9 percent, set in 2016.
2. The uninsured rate among adults ages 18-64 was 11.8 percent in the first quarter of 2022. The uninsured rate for children ages 0-17 was 3.7 percent.
3. About 5.2 million people have gained health coverage since 2020. Gains in coverage are concurrent with the implementation of the American Rescue Plan’s enhanced ACA Marketplace subsidies, the continuous enrollment provision in Medicaid, several state Medicaid expansions and enrollment outreach efforts.
Mark Cuban’s pharmacy, Cost Plus Drug Co., has hundreds of drugs marked at discounted prices, but some pharmacy experts say there’s a larger problem that needs fixing, CNBC reported July 28.
The online pharmacy launched in January with about 100 drugs, and by its one-year anniversary, plans to have more than 1,500 medications, according to the company’s website. The business model, which allocates for a $3 pharmacy dispensing fee, $5 shipping fee and a 15 percent profit margin with each order, aims to uproot the pharmaceutical industry, which has faced criticism for years about its opaque business practices.
Gabriel Levitt, the president of PharmacyChecker, a company that monitors the cheapest drug prices, told CNBC there’s more to be done.
“As much as I support the venture, what they’re doing does not address the big elephant in the room,” Mr. Levitt said. “It’s really brand-name drugs that are increasing in price every year and forcing millions of Americans to cut back on medications or not take them at all.”
Brand-name drugs are 80 percent to 85 percent more expensive than generics since brand-name drugs have to repeat clinical tests to prove efficacy, according to the FDA. Cost Plus Drug Co. only offers generics. Mr. Cuban told CNBC he hopes to sell brand-name medications “within six months,” but added that it’s a tentative timeline.
Despite the hype, accountable care organizations (ACOs) and other Medicare-driven payment reform programs intended to improve quality and lower healthcare spending haven’t bent the cost curve to the extent many had hoped.
A recent and provocative opinion piece in STAT News, from health policy researcher Kip Sullivan and two single-payer healthcare advocates, calls for pressing pause on value-based payment experimentation. The authors argue that current attempts to pay for value have ill-defined goals and hard-to-measure quality metrics that incentivize reducing care and upcoding, rather than improving outcomes.
The Gist: We agree with the authors that current value-based care experiments have been disappointing.
The intention is good, but the execution has been bogged down by entrenched industry dynamics and slow-to-move incumbents. One fair criticism: ACOs and other “total cost management” reforms largely focus on the wrong problem. They address utilization, rather than excessive price.
But we’re having a price problem in the US, not a utilization problem.Europeans, for example, have more physician visits each year than Americans, yet spend less per-person on healthcare. It’s our high prices—for everything from physician visits to hospital stays to prescription drugs—that drive high healthcare spending.
The root cause: our third-party payer structure actively discourages real efforts to lower price—every player in the value chain, including providers, brokers, and insurers, does better economically as prices increase. That’s why price control measures like reference pricing or price caps have been nonstarters among industry participants.
Recent reforms that increase price transparency, while not the entire solution, at least shine a light on the real challenges our healthcare system faces.
A recent Wall Street Journal analysis, published this week, provides further evidence that large, nonprofit health systems often offer less charity care than their for-profit peers. It found that, on average, nonprofit systems spent 2.3 percent of their net patient revenue on financial aid for patients, whereas for-profit hospitals spent 3.4 percent.
The American Hospital Association criticized the analysis, arguing that it doesn’t fully capture the broader community benefits that nonprofit hospitals provide. Earlier this year the Lown Institute, a Boston-based think tank, also found that most nonprofit hospitals invest less in their communities and spend less on charity care than the amount they receive from tax exemptions.
The Gist: The issue of whether hospital systems should continue to enjoy tax-exempt status is a perennial stalking horse in the health policy community. The topic often gets conflated with whether nonprofit systems are truly “nonprofit”, since many larger systems make robust profits.
There’s no question that nonprofit systems enjoy a huge economic advantage from not being subject to taxation, in return for which we should expect them to provide “community benefit” at a level commensurate with the status.
The difficulty is in defining and measuring community benefit— for example, should serving Medicaid patients count? Is it fair to count discounts for the uninsured as “charity care”, if we know prices are artificially inflated in the first place? These are thorny questions with no obvious answers, but ones that would benefitfrom clearer guidance and more transparency from policymakers.
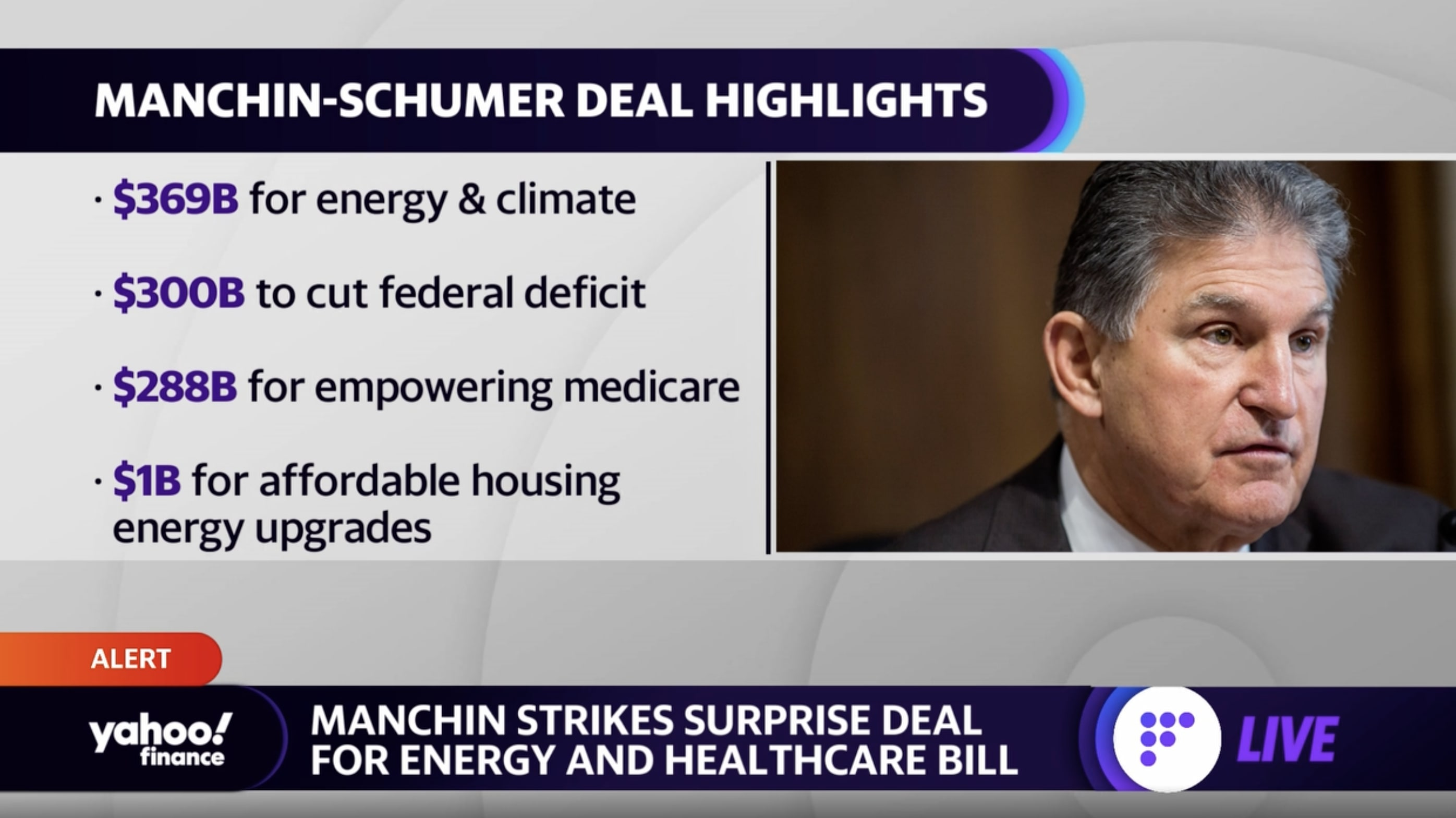
Senate Majority Leader Chuck Schumer (D-NY) and Senator Joe Manchin (D-WV) surprised everyone Wednesday night by announcing they reached a deal on a legislation package called the Inflation Reduction Act of 2022. The deal is a revival of portions of President Biden’s “Build Back Better” plan, more narrowly scoped to meet the demands of Sen. Manchin.
On the healthcare front, the bill would allow Medicare to negotiate prices for certain prescription drugs starting in 2026, and limit seniors’ annual out-of-pocket spending on Part D prescriptions to $2,000. It also includes $64B to extend the enhanced tax credits for Affordable Care Act exchange plans through 2025, avoiding health plan rate increases for millions of Americans.
The Gist: While several Senate Democrats have announced support for the legislation, the party can’t afford any holdouts given its razor-thin majority. If all Democrats get on board, this legislation will fulfill the party’s longtime promise to lower prescription drug prices. But it stops well short of other major healthcare measures being discussed last year, including expanding Medicare coverage to include dental, vision, and hearing coverage, and closing the so-called Medicaid coverage gap.
After a few years of relatively unchanged monthly premiums, a Kaiser Family Foundation analysis of 72 rate filings for 2023 finds a median 10 percent increase. Insurers say the biggest driver is rising medical costs, driven by higher rates for provider services and pharmaceuticals, as well as a return to pre-pandemic utilization levels. Insurers aren’t expecting COVID-19 or federal policy changes—including a potential extension of enhanced subsidies—to have much of an impact on rates.
The Gist:High inflation and the growing wage-price spiral have left providers with much higher costs, which is sure to drive up the overall cost of healthcare. Where provider systems have the leverage to demand higher rates from insurers, this will inevitably drive up premiums—an effect that is already starting to show up in the individual insurance market.
If Congressional Democrats are able to extend ACA subsidies, most ACA enrollees won’t actually feel these premium increases, but as contracts in the group market come up for renewal, we’d expect inflation in employer-sponsored premiums as well. Given the cost-sharing now built into most benefit plans, individual consumers will likely see healthcare join gas, food, and housing as household costs that are experiencing unsustainable inflationary increases.
Healthcare costs are becoming an increasing source of stress for older Americans, leading to some paring back on treatment, medicines or other spending on food and utilities — or skipping them altogether — to cover medical costs, according to new research conducted by Gallup in partnership with West Health.
The survey of U.S. adults released Wednesday found that almost half of adults aged 50 to 64 and more than a third of adults 65 and older are concerned they won’t be able to pay for needed healthcare services in the next year. That’s nearly 50 million older Americans.
About 80 million adults above age 50 see healthcare costs as a financial burden. Becoming eligible for Medicare seems to assuage those worries slightly, however: 24% of adults aged 50 to 64, who are not yet eligible for the federal health insurance, said health costs were a major burden. That percentage fell to 15% for those aged 65 and above.
Dive Insight:
The West Health-Gallup survey, conducted in September and October of 2021, is the latest vignette of how exorbitant healthcare costs in the U.S. are increasingly impacting the financial stability of Americans, especially those of retirement age who are more likely to have expensive medical needs.
Out-of-pocket healthcare expenses for adults aged 65 and older increased 41% from 2009 to 2019, according to HHS data. That population spends on average almost double their total expenditures on healthcare costs compared with the general population, despite Medicare coverage.
That cost problem is only likely to worsen amid surging inflation raising the cost of groceries, gas and other needed items. Additionally, U.S. demographics shifts are an added stressor. By 2030, the percentage of Americans 65 years and older will outweigh those under the age of 18, a first in the country’s history, according to Census Bureau projections.
“As sizable numbers of Americans 65 and older face tangible tradeoffs to pay for healthcare, many more Americans in the next decade will incur health and financial consequences because of high costs,” researchers wrote in the report.
The West Health-Gallup poll found about one in four adults aged 65 and above cut back on food, utilities, clothing or medication to cover healthcare costs. That’s compared to three in 10 for adults aged 50 to 64.
Older women and Black adults were more likely to forgo basic necessities to pay for healthcare than other demographics.
More than 20 million Americans aged 50 years and above said there was a time within the last three months when they or a family member was sick, but didn’t seek treatment due to cost.
More than 15 million Americans said they or a family member skipped a pill or dose of prescribed medicine in order to save money.
Researchers urged policymakers to act to improve efficiency and reduce the costs of medical care and prescription drugs in the U.S. Congress has yet to take meaningful action to lower medical costs, despite rising support for government intervention and high-profile proposals from the Biden administration.
The rise of the BA.5 variant is spurring new calls for funding for an Operation Warp Speed 2.0 to accelerate development of next-generation COVID-19 vaccines that can better target new variants.
The BA.5 subvariant of omicron that now makes up the majority of U.S. COVID-19 cases is sparking concern because it has a greater ability to evade the protection of current vaccines than past strains of the virus did.
Pfizer and Moderna are working on updated vaccines that target BA.5 that could be ready this fall, but experts say that by the time they are ready, a new variant very well could have taken hold.
As alternatives to vaccine makers chasing each variant, experts point to research on “pan-coronavirus” vaccines that are “variant-proof,” targeting multiple variants, as well as nasal vaccines that could drastically cut down on transmission of the virus.
There is ongoing research on these next-generation vaccines, but unlike in 2020, when the federal government’s Operation Warp Speed helped speed the development of the original vaccine, there is less funding and assistance this time around.
COVID-19 funding that could help develop and manufacture new vaccines more quickly has been stalled in Congress for months.
“There’s no Operation Warp Speed,” said Eric Topol, professor of molecular medicine at Scripps Research. “So it’s moving very slowly. But at least it’s moving.”
Leana Wen, a public health professor at George Washington University, wrote in a Washington Post op-ed this week that the U.S. needs “urgent investment” in next-generation vaccines and “we need an ‘Operation Warp Speed Part 2.’”
Pfizer and Moderna are working on updated vaccines that target BA.5 that could be ready this fall, but experts say that by the time they are ready, a new variant very well could have taken hold.
As alternatives to vaccine makers chasing each variant, experts point to research on “pan-coronavirus” vaccines that are “variant-proof,” targeting multiple variants, as well as nasal vaccines that could drastically cut down on transmission of the virus.
There is ongoing research on these next-generation vaccines, but unlike in 2020, when the federal government’s Operation Warp Speed helped speed the development of the original vaccine, there is less funding and assistance this time around.
COVID-19 funding that could help develop and manufacture new vaccines more quickly has been stalled in Congress for months.
“There’s no Operation Warp Speed,” said Eric Topol, professor of molecular medicine at Scripps Research. “So it’s moving very slowly. But at least it’s moving.”
Leana Wen, a public health professor at George Washington University, wrote in a Washington Post op-ed this week that the U.S. needs “urgent investment” in next-generation vaccines and “we need an ‘Operation Warp Speed Part 2.’”
Administration health officials pointed to funding when asked about next-generation vaccines at a press briefing on Tuesday.
“We need resources to continue that effort and to accelerate that effort,” said Anthony Fauci, the government’s top infectious disease expert. “So although we’re doing a lot and the field looks promising, in order to continue it, we really do need to have a continual flow of resources to do that.”
But COVID-19 funding has been stuck in Congress for months. Republicans have long said they do not see any urgency in approving the money. Democrats, while generally calling for the funding, have been caught up in their own internal divisions, like when a group of House Democrats objected to a way to pay for the new funding in March.
“Of course more funding would accelerate some parts of the development,” Karin Bok, acting deputy director of the National Institutes of Health’s (NIH) Vaccine Research Center, said in an interview.
She also cautioned that development of next-generation vaccines like nasal vaccines would take longer than the original vaccines, because less groundwork has been laid over the preceding years.
Experts stress that even for BA.5, the current vaccines still provide important protection against severe disease and hospitalization, and are urging people to get their booster shots now. But there is potential for further improvement in the vaccines as well.
Aside from funding, another obstacle is obtaining copies of the existing COVID-19 vaccines for use in research, said Pamela Bjorkman, a California Institute of Technology professor working on a next-generation vaccine.
“I would say we’ve wasted at least six months,” with various procedural hurdles on that front, she said. “It’s just ridiculous.”
For example, she said at one point when her team was able to get access to the AstraZeneca COVID-19 vaccine, it then took two or three months to get an import permit to send it from the United Kingdom.
“This is a hot topic,” Bok, of the NIH, said of access to existing vaccine doses for researchers. “The government is working very hard on an agreement with the companies to provide it to us and to all the investigators…that are funded by NIH.”
Asked about providing vaccine doses for researchers and any talks with the administration on that front, a Moderna spokesperson said: “We do provide vaccine in certain investigator-initiated studies where physicians and scientists propose research they have designed and want to conduct with our support,” pointing to a South African study as an example.
More broadly, the White House says it is working on accelerating next-generation vaccine research and will have more announcements soon.
“Let me be very clear: We clearly need a true next-generation vaccine,” White House COVID-19 response coordinator Ashish Jha told reporters on Tuesday.
“You’ll hear more from us in the days and weeks ahead,” he added. “This is something that we have been working quite assiduously on.”