As the first Americans receive COVID vaccines, supplies remain limited even for the highest-risk populations. And with doses now in the pipeline, states are facing more intense questions about how they will prioritize vaccine delivery across demographic and at-risk groups. The graphic above shows an estimated vaccination timeline, based on the Centers for Disease Control and Prevention’s (CDC) recommended schedule. It illustrates the relative size of different populations in each allocation phase, along with the likely difficulty of targeting them and verifying eligibility. The first phase is divided into three waves (1a, 1b, 1c) for at-risk populations and essential workers, while the second phase includes the rest of the adult population, as well as children (though pediatric clinical trials are still in early stages).
Unsurprisingly, the CDC recommends that those most at risk for infection and severe disease—healthcare workers and nursing home residents—receive the 20M doses available by year’s end.While most states are generally adhering to the initial recommendations on priority groups for phase 1a set by the CDC’s Advisory Committee on Immunization Practices (ACIP), several have made adjustments. At least three are including law enforcement personnel in phase 1a, and others are further categorizing healthcare workers into high-, medium-, and low-risk groups. This weekend, ACIP will reconvene to create its official recommendations for phases 1b and 1c, which include the much larger populations of adults over age 65, and those with high-risk medical conditions.
Beyond eligibility guidelines, larger questions loom. How would someone “verify” that they have a high-risk condition? Who will reach out to older Americans to let them know they are eligible, and where to access the vaccine? As vaccine rollout continues, providers should anticipate the role they will likely play in managing patients “in the queue”, documenting eligible conditions and establishing regular information channels to keep people informed about the current status of vaccine planning and access.
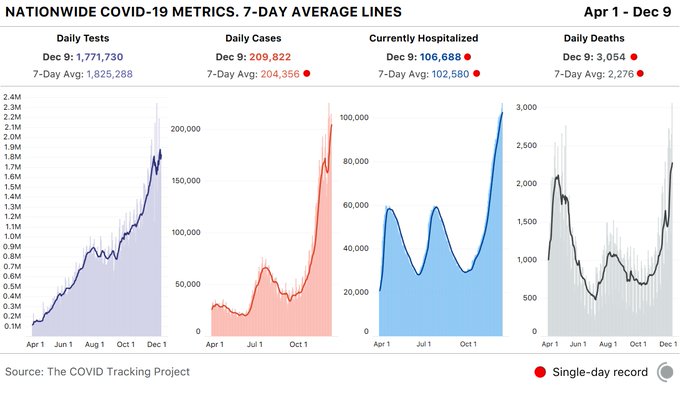
But first, we have a difficult period to get through. This week again saw record-breaking numbers of cases, hospitalizations, and deaths from COVID-19, with Thursday alone bringing more than 238,000 new cases—and a staggering 3,293 fatalities.
Nearly 115,000 Americans are currently hospitalized with COVID, a rise of 16 percent from just two weeks ago, and in many places a precarious capacity situation has turned perilous. Conditions have worsened precipitously in California, with only Tennessee, Oklahoma, and Rhode Island registering more daily COVID cases per 100,000 population than the Golden State, although cases are still on the rise across 80 percent of states and territories.
Intensive care availability in Southern California hit zero, with ICU volume there expected to double or triple by this time next month. The same stresses are playing out in dozens of markets across the country, leading to a staffing sustainability crisis that can’t be solved through paying overtime, cancelling vacations or looking to travel nurses to fill the gaps in a now nationwide crisis. With the Christmas and New Year’s holidays still ahead, experts predictCOVID cases won’t peak until sometime in mid-January, with a peak in hospitalizations and deaths following several weeks after.
Several states and cities tightened restrictions on gatherings and issued new stay-at-home orders, in an effort to keep new cases at a level that allows hospitals to manage through the next several weeks and maintain care quality and access for COVID and non-COVID patients alike. The coming weeks will require every American to take greater precautions than at any time during the course of this pandemic.
An Oregon physician who publicly spoke out against wearing a mask to slow the spread of COVID-19 has had his medical license suspended, according to The Washington Post.
In a written order Dec. 4, the Oregon Medical Board suspended the license of Steven A. LaTulippe, MD, a family medicine physician at South View Medical Arts in Dallas, Ore. The board alleges Dr. LaTulippe engaged in “conduct that is contrary to medical ethics and does or might constitute a danger to the health or safety of the public.”
It also accuses him of “gross negligence.”
Specific acts cited in the letter include the physician’s alleged advice to a Medicaid patient. According to the board, the patient contacted Dr. LaTulippe’s medical clinic in July for guidance on COVID-19 and was told asymptomatic people should not be tested, that wearing masks does not prevent virus transmission, and the patient was told not to self-isolate because exposure to others would provide COVID-19 immunity.
The board said the patient seeking the guidance from Dr. LaTulippe’s clinic was terminated as a patient after questioning the appropriateness of the guidance.
The board also contends workers in Dr. LaTulippe’s clinic refuse to wear masks at work and urge people who enter the clinic wearing masks to remove them.
Dr. LaTulippe “regularly tells his patients that masks are ineffective in preventing the spread of COVID-19 and should not be worn”; “directs patients to a YouTube video providing false information about mask-wearing” ; and “regularly advises, particularly for his elderly and pediatric patients, that it is ‘very dangerous’ to wear masks because masks exacerbate [chronic obstructive pulmonary disease] and asthma and cause or contribute to multiple serious health conditions,” according to the board.
The Post could not immediately reach Dr. LaTulippe for comment Dec. 5.
In a recent interview, Dr. LaTulippe told NBC News he believes there is “bad science behind” wearing masks.
“I have absolutely zero problems with infectivity, and I have completely successful treatments, so I ask, ‘What is the problem?’ Why would I be demonized if I know what I’m doing?” he told the news network.
The CDC has advocated wearing masks to combat COVID-19.
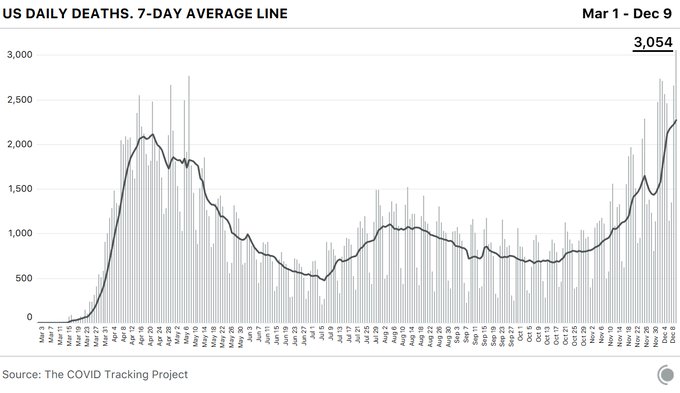
The coronavirus pandemic pushed the U.S. past another dire milestone Wednesday, the highest daily death toll to date, even while the mortality rate has decreased as health experts learn more about the disease.
The Covid Tracking Project, which tracks state-level coronavirus data, reported 3,054 COVID-19 related deaths — a significant jump from the previous single-day record of 2,769 on May 7.
The spread of the disease has shattered another record with 106,688 COVID-19 patients in U.S. hospitals. And overall, states reported 1.8 million tests and 210,000 cases. According to the group, the spike represents more than a 10% increase in cases over the last 7 days.
Additionally, California nearly topped its single-day case record at 30,851. It is the second highest case count since December 6, the organization reported.
The staggering spike in fatalities and infections has overwhelmed hospitals and intensive care units across the nation, an increase attributed by many experts to people relaxing their precautions at Thanksgiving.
Many hospitals are temporarily or permanently reducing the size of their workforce as they grapple with depleted revenues and the thorny question of when they can return to normal operating capacity. Here’s a tracker to follow the latest updates.
Hospitals across the country, financially battered as they face the dual challenges of sick COVID-19 patients and a precipitous decline in patient volume, are struggling to balance quickly shifting staffing needs. While some face and others brace for intense demand, many have announced furloughs of specialists and others that work in elective surgeries that have been drastically scaled back.
Thousands of healthcare workers at hospitals big and small have been asked not to return to work, and it’s still unclear how soon non-essential services will return. While some governors announce plans to reopen businesses, others have extended stay-at-home orders.
Most recent data from the U.S Bureau of Labor doesn’t cover the second half of March or early April, but during the first half of March, the healthcare industry shed 43,000 jobs — reversing a decade of growth in the sector. According to BLS data, the industry added 49,000 jobs in March 2019.
“Even our emergency room has seen a significant drop in patients coming in,” Sue Philips, an ICU nurse at Palomar Pomerado Health in Northern San Diego, told Healthcare Dive.
Phillips is a spokesperson with National Nurses United, the country’s largest nurses union. Palomar Health, which runs three medical centers in northern San Diego County, recently instituted 21-day temporary layoffs of 221 employees.
On April 28, Palomar announced that most of those layoffs were becoming permanent. The system laid off 5% of its workforce, eliminating 317 positions. Fifty of those employees were clinical RNs, mostly in part-time positions, and the rest spread across the organization ranging from clerical staff to technicians.
Due to a 50% decrease in patient volumes, Palomar lost $10 million in revenue in March alone, according to a statement. In April the system said it stands to lose $20 million or more.
“I’m an ICU nurse, so my job is pretty much protected,” Phillips said. “But you didn’t think you were expendable until you became expendable, and that’s a hard pill for nurses and caregivers to swallow.”
Congress has attempted to financially support struggling hospitals through ongoing coronavirus relief legislation, approving some $175 billion thus far. But without knowing what will come next, hospitals are attempting to remain nimble while reining in one of their most costly expenses — paying employees.
The following information is based on publicly reported data, along with interviews with hospital representatives and union members.
It’s not an exhaustive list, but features nonprofit and for-profit hospital systems that reported revenue above $10 billion in 2019. It also takes a look at smaller, more regionally based systems that have announced similar cutbacks.
Click on link above to use the dropdown to find a company.
Healthcare job losses reached staggering levels amid stay-at-home orders and the widespread cancellation of elective procedures when the COVID-19 pandemic first hit this spring. Dentists and ambulatory services were particularly hard hit.
While the industry has since recovered many of the 1.3 million jobs lost this April, it’s still 527,000 short from February levels, and monthly gains have slowed since, according to the latest data from the Bureau of Labor Statistics.
At the same time, some of the major hospitals that issued furloughs or layoffs early in the pandemic are now further reducing the size of their workforce.
The stagnation will likely continue, as companies “don’t hire as many people, then lay some people off to also try and save money, because worse times may be ahead,” said Erica Groshen, former BLS commissioner and senior labor economics adviser at Cornell’s School of Industrial and Labor Relations.
One example is Dallas-based Baylor Scott & White, which laid off 3% of its workforce, or 1,200 employees in May. It’s now laying off a third of its corporate finance staff, though some impacted employees are being offered positions with a third-party vendor, the system said in a Monday statement.
Providence Health & Serviceslaid off 183 employees in mostly administrative roles as a result of transitioning work to a third-party vendor, while five employees were laid off “as a result of business need,” according to a WARN notice letter the system sent to an Oregon state agency Nov. 16. It previously issued an unknown number of furloughs across its 51-hospital system.
And Utah-based Intermountain Healthsaid it would cut 250 business-related jobs by offering 750 employees voluntary separation packages on Oct. 13.
The moves come even while hospitals are stretched to the brink from the highest surge of coronavirus cases the country has yet seen. In the past few weeks, many have halted elective procedures and paid steep rates for temporary nursing staff, further straining finances.
And other healthcare establishments, such as some doctor’s offices and medical labs, are still struggling to get reluctant patients back in.
A recent Labor Department survey covering the onset of the pandemic through September found among all healthcare businesses, 64% experienced a decrease in demand while only 13% experienced an increase in demand.
In November, healthcare businesses overall added 46,000 jobs in — fewer than the 58,000 jobs added in October; 53,000 in September; and 75,000 in August, according to BLS data.
Hospitals added about 4,000 jobs in November and are about 100,000 jobs short from February.
The financial challenges caused by the COVID-19 pandemic have forced hundreds of hospitals across the nation to furlough, lay off or reduce pay for workers, and others have had to scale back services or close.
Lower patient volumes, canceled elective procedures and higher expenses tied to the pandemic have created a cash crunch for hospitals. U.S. hospitals are estimated to lose more than $323 billion this year, according to a report from the American Hospital Association.
Hospitals are taking a number of steps to offset financial damage. Executives, clinicians and other staff are taking pay cuts, capital projects are being put on hold, and some employees are losing their jobs. More than 260 hospitals and health systems furloughed workers this year and dozens of others have implemented layoffs.
Below are 15 hospitals and health systems that announced layoffs since Sept. 1, many of which were attributed to financial strain caused by the pandemic.
1. Minneapolis-based Children’s Minnesota is laying off 150 employees, or about 3 percent of its workforce. Children’s Minnesota cited several reasons for the layoffs, including the financial hit from the COVID-19 pandemic. Affected employees will end their employment either Dec. 31 or March 31.
2. Dallas-based Baylor Scott & White Health announced in early December that it will lay off 102 employees in finance and accounting roles. The duties of the affected workers will be outsourced to a third-party vendor in India.
3. Eastern Niagara Hospitalin Lockport, N.Y., announced in early November that it plans to end intensive care unit services and move surgical services from the hospital to a surgery center. The changes will result in the loss of 80 jobs.
4. Detroit Medical Centerconfirmed in November that it laid off employees but declined to disclose the number of employees affected. Clinical staff, administrative assistants and employees at the management level were affected by the layoffs, sources told Crain’s Detroit Business.
5. Mercy Iowa City (Iowa) laid off 29 employees in November to address financial strain tied to the COVID-19 pandemic.
6. NorthBay Healthcare, a nonprofit health system based in Fairfield, Calif., announced Nov. 2 that it is laying off 31 of its 2,863 employees as part of its pandemic recovery plan.
7. Brattleboro Retreat, a psychiatric and addiction treatment hospital in Vermont, notified 85 employees in late October that they would be laid off within 60 days.
8. Oakland, Calif.-based Kaiser Permanente notified the state of Hawaii in November that it planned to lay off 45 employees within 60 days. “The COVID-19 public health crisis has placed unprecedented demands on the entire health care system, including Kaiser Permanente,” a Kaiser spokesperson said in an email to Pacific Business News. “Even before the pandemic, we had been transparent in sharing that Kaiser Permanente Hawaii faced ongoing financial challenges and that we were on a path to address our internal structure in a way that ensured we would be able to continue to deliver high-quality, affordable care and coverage to our members in Hawaii for years to come.” The health system said most of the positions eliminated were administrative or in non-patient facing areas.
9. Citing a need to offset financial losses, Minneapolis-based M Health Fairview said in October it plans to downsize its hospital and clinic operations. As a result of the changes, 900 employees, about 3 percent of its 34,000-person workforce, will be laid off.
10. Lake Charles (La.) Memorial Health System laid off 205 workers, or about 8 percent of its workforce, in October as a result of damage sustained from Hurricane Laura. The health system laid off employees at Moss Memorial Health Clinic and the Archer Institute, two facilities in Lake Charles that sustained damage from the hurricane.
11. Burlington, Mass.-based Wellforcelaid off 232 employees in September as a result of operating losses linked to the COVID-19 pandemic. The health system, comprising Tufts Medical Center, Lowell General Hospital and MelroseWakefield Healthcare, experienced a drastic drop in patient volume earlier this year due to the suspension of outpatient visits and elective surgeries.
12. Baptist Health Floydin New Albany, Ind., part of Louisville, Ky.-based Baptist Health, eliminated 36 positions in late September. The hospital said the cuts, which primarily affected administrative and nonclinical roles, are due to restructuring that is “necessary to meet financial challenges compounded by COVID-19.”
13. Cincinnati-based UC Health laid off about 100 employees in September. The job cuts affected both clinical and non-clinical staff. A spokesperson for the health system said no physicians were laid off.
14. Springfield, Ill.-based Memorial Health System laid off 143 employees in September, or about 1.5 percent of the five-hospital system’s workforce. The health system cited financial pressures tied to the pandemic as the reason for the layoffs.
15. Watertown, N.Y.-based Samaritan Health announced Sept. 8 that it laid off 51 employees and will make other cost-cutting moves to offset financial stress tied to the COVID-19 pandemic.
Letter of Intent offered to acquire Rhode Island-based Care New England Health System
StoneBridge Healthcare, LLC (StoneBridge), an innovative company formed to buy, save and turn around distressed hospitals in the cities and suburbs of America, today announced it has presented a Letter of Intent (LOI) to purchase Rhode Island-based Care New England Health System. StoneBridge would make a significant investment in order to financially stabilize Care New England to allow the health system to continue its mission to transform the future of health care for the communities it serves.
“Care New England Health System has provided outstanding care to its patients for many years, and StoneBridge Healthcare is committed to the continuation of this high standard of care in Rhode Island,” said Joshua Nemzoff, Chief Executive Officer, StoneBridge Healthcare. “We believe that StoneBridge Healthcare is in a strong position to help Care New England to continue delivering cutting-edge care to the communities it serves for years to come.”
StoneBridge has offered a transaction value of $550 million with a purchase price of $250 million and a $300 million investment in capital improvements over six years to further transform the health system. The offer that StoneBridge has submitted includes a provision that will fully fund the employee’s pension plan at closing – a plan that is currently underfunded by more than $125 million. Care New England hospitals include the following: Butler Hospital, Kent Hospital, Women & Infants Hospital of Rhode Island, Care New England Medical Group, the VNA of Care New England, The Providence Center, and a certified accountable care organization (ACO) Integra.
“As the cost of care has risen and the COVID-19 pandemic has placed a tremendous strain on health systems across the nation, StoneBridge Healthcare is ready to assist Care New England during these challenging times to continue delivering an outstanding continuum of care to the region,” Nemzoff added. “StoneBridge Healthcare has the expertise and financial resources needed to help lead Care New England to a promising future.”
The LOI is not binding, and a Definitive Agreement would be finalized in a short period of time once comprehensive due diligence is performed. StoneBridge is a privately-owned company capitalized through a multi-layered composite finance group that includes nationally known debt and equity sources.
Earlier this year, StoneBridge submitted an offer to acquire the Erlanger Heath System in Tennessee for a transaction value of $475 million. StoneBridge is actively pursuing discussions related to this transaction, which is a system of similar size to Care New England and has also been devastated by the impact of the COVID-19 pandemic.
About StoneBridge Healthcare StoneBridge Healthcare is an innovative company formed to buy, save and turn around deeply distressed hospitals in the cities and suburbs of America. StoneBridge is capitalized through a multi-layered composite finance group that includes nationally known debt and equity sources. The company features a nationally recognized team of experts in healthcare operations, finance, acquisitions and turnarounds.
Our decades of experience, our financial investment and our commitment to expand primary care into the urban areas we serve make our company the only one of its kind. StoneBridge Healthcare plans to purchase and turn around acute care hospitals that are in significant economic distress and could otherwise be forced to close. StoneBridge will identify and buy hospitals that can be saved, and then work urgently to make sure these hospitals survive and succeed.
StoneBridge is committed to responding to the healthcare needs of the urban markets it operates in through an initiative that is known as “The Mission Project.” Using the hospitals it acquires as a base of operations, StoneBridge will bring much-needed services into the community. StoneBridge will listen to and work with local groups to understand the gaps in community care – and then put money and time into offering clinics or other life-changing help. The solutions may look different in each market, but the commitment will be consistent. The hospitals can provide the doctors, nurses, pharmacies, kitchens and vehicles to bring care and support to people where they live. For more information please visit: stonebridgehealthcare.com.
The South Dakota-based health system has suspended talks related to its planned merger with Utah-based Intermountain Healthcare after the sudden departure of its CEO, Kelby Krabbenhoft. Sanford and its new CEO will instead focus on organizational needs, the system said.
The decision to halt merger talks comes about two weeks after Sanford Health and President and CEO Kelby Krabbenhoft mutually agreed to part ways. Krabbenhoft led the 46-hospital system for 24 years, assuming the top position in 1996. A press release noted his contributions to the Sioux Falls, South Dakota-based organization’s growth from a community hospital into a large rural nonprofit spanning 26 states.
Sanford Health did not give an official reason for Krabbenhoft’s sudden departure, but days before the announcement, CNN obtained an email sent by the former CEO to health system staff telling them that he had contracted Covid-19 and recovered. He also said he would not be wearing a mask.
Krabbenhoft said there was “growing evidence” of immunity to the new coronavirus and that wearing a mask “sends an untruthful message that I am susceptible to infection or could transmit it. I have no interest in using masks as a symbolic gesture,” CNN reported. But evidence regarding immunity after recovery from Covid-19 is still limited and some reinfections have been reported.
Bill Gassen, previously serving as chief administrative officer, succeeded Krabbenhoft as the organization’s new leader.
The health system decided to stop merger activity to address other organizational needs as Gassen takes over, according to a press release.
“With this leadership change, it’s an important time to refocus our efforts internally as we assess the future direction of our organization,” Gassen said in the press release. “We continue to prioritize taking care of our patients, our people, and the communities we serve as we look to shape our path forward.”
Sanford and Intermountain declined to comment on whether the organizations are planning to resume talks in the future.
“We are disappointed but understand the recent leadership change at Sanford Health has influenced their priorities,” said Dr. Marc Harrison, president and CEO of Salt Lake City-based Intermountain Healthcare, in the press release. “There’s much to admire about the work that Sanford Health is doing. We continue to share a strong vision for the future of healthcare.”
Had the talks continued and the merger been approved, the combined organization would have included 70 hospitals, 435 clinics and 233 senior care locations. It was expected to generate about $15 billion in total annual revenue.
Intermountain’s Harrison was slated to serve as the combined system’s leader, while Krabbenhoft was to serve as president emeritus.
They have been at this for almost a year. While politicians argued about masks, superspreader weddings made the news, a presidential election came and went, and at least 281,000 Americans died, nurses reported for work. The Post asked seven ICU nurses what it’s been like to care for the sickest covid patients. This is what they want you to know.
As of Dec. 7, Idaho has seen 110,510 total confirmed cases, 1,035 deaths, and 477 people are currently hospitalized with the virus.
Kori Albi, 31
Covid unit intensive care nurse and unit supervisor, Saint Alphonsus Regional Medical Center
Our staff are getting sick. Our physicians are getting sick. And they’re not getting it from the hospital. They’re getting it from the community. We are almost lucky to care for the covid patients because we know who they are. Anytime we go into these rooms, we know exactly what we need to do. We have all the PPE we need. And as long as we are diligent and follow all the processes that are in place, we can keep ourselves safe. That’s not what worries me at all. Going out into the community is scarier than coming into work every day. Because you don’t know who has it.
This virus has caused this feeling, this sense of isolation. The covid unit is an isolated desert. Every door is shut. Every room has negative airflow. By the time you put your N95 mask on and then your surgical mask over the top of that, then you put your isolation gown on and your face shield on top of that, you can’t tell who is who. So much of health care is about that personal touch — now, our patients can’t even see our name badges because they are on under our gowns. All they see are our eyes through our face mask.
A lot of families are hesitant to have Zoom calls with patients because it can be uncomfortable and awkward. Especially if these patients are sedated and intubated. There’s always that awkwardness of: Can they hear you? Can they not hear you? Even as nurses, we feel like we’re talking to the wall. But we talk to them just as if they were awake. Allowing families to play their music that they like or pray with them or just talk to them can absolutely help. You see vital signs change.
One patient, all she wanted to do was have her son sing her a song. I think I spent over an hour in the room listening to him play the guitar and sing her a song. He sang her mostly hymns.
Death is a very intimate event that normally involves a lot of family members that help bring closure and that helps everyone process. In normal circumstances, health care providers form these relationships with the family at the bedside. All of that has been removed. And we now have to try to form those relationships over the telephone. It’s a traumatic experience. And it’s a long drawn-out process. A lot of people don’t make it out of here. It’s a slow, lonely death.
The amount of death with covid is profound. As nurses, we have learned to process death, but the amount of death has happened in such a short span of time — that’s what’s been overwhelming. I had a patient that we did a Zoom call with. His four-year-old granddaughter lived with him. And she brought tears to the room. The naivete of a four-year-old. Her grandfather was intubated so he couldn’t talk. But he could kind of look around the room. But the innocence of her, saying, “Come home, Pa. I miss you, Pa. I love you Pa,” all through a video screen. The 14-year-old that also lived with them couldn’t formulate words to say anything, and he didn’t know what to do or say in that video. But the four-year-old was telling Pa to come home.
JACKSON, MISS.
As of Dec. 7, Mississippi has seen 166,194 total confirmed cases, 3,961 deaths, and 1,157 people are currently hospitalized with the virus.
Catie Carrigan, 28
ICU, University of Mississippi Medical Center
There are some patients who have been in their younger 20s and their younger 30s, and I think maybe those are the hardest cases. They have families and they have kids just like I do, and it’s hard coming into work and taking care of them. Knowing they’re supposed to be going to college, they’re supposed to be getting married, they’re supposed to be having kids and, instead, they’re laying in a hospital bed on a ventilator fighting for their life.
They have their whole entire lives ahead of them, and then they get hit with this disease that everybody thinks is a hoax and then they die.
I worked in the ER a month ago, so I know exactly what’s going on down there, and now I work in the ICU, so I know exactly what’s going on on both sides of it. There are no ICU beds in the hospital. None. When there are no ICU beds, we hold them in the ER, or we hold them in the PACU (post-anesthesia care unit). The ER still has to treat our trauma patients, our car accidents, our gunshot victims. So when we have those ICU holds in the ER, it obviously makes the jobs of nurses and doctors in the ER way more difficult than it needs to be. We are treating patients in the hallway. They’re just trying to do the best they can with the resources that we have.
There is no room left, essentially, and I think that’s really what people don’t seem to understand. And I get it, when you’re not in health care you don’t really see our side of it, but we’re seeing the worst of it. It’s hard for us to convey that to the public because they don’t seem to want to take our word for it — but take our word for it. Take our word for it.
IOWA CITY
As of Dec. 7, Iowa has seen 244,844 total confirmed cases, 2,717 deaths, and 898 people are currently hospitalized with the virus.
Allison Wynes, 39
Medical intensive care unit, University of Iowa Hospitals and Clinics
I cry every day when I walk in to work, and I cry every day when I walk to my car after work.
You get it out of your system before you show up and you do your job and you’re fine. Then, you go home and you cry before you get home. And then you go home and be mom.
My 9-year-old daughter asks frequently, “Mommy, how many patients were there today? Mommy, how many sick ones were there today? Were you safe? Was everything okay? Do you have to go to work again? How many patients?” She gets it.
I think one thing that people do not appreciate is it’s not only the number or volume of patients that comes through — it’s the level of care that they require, which is so much greater than a standard patient in the ICU or a standard patient in the floor, because they can get very, very sick very quickly.
We were walking a patient who was on ECMO, which is extracorporeal membrane oxygenation, and it took five people to walk her. That’s not normal.
I work in the MICU, so it’s never like a party up in here, but it used to at least be, nine times out of ten, calm and controlled and tidy and clean. Occasionally stuff would go bad and we would all run and help, and then we would all go about our days. Now it just feels like, especially of late, there is equipment everywhere. There are gowns everywhere. There are gloves everywhere, there are people everywhere, and there are fires everywhere.
I’m actually scared, and I’ve never been scared at work before. I am scared that we will lose control.
It’s the human resources we are running low on. We can make a bed, we can find a ventilator, we have PPE. But it’s the human cost of caring for these patients that has been keeping me up at night the past couple of weeks and really making me nauseous every day.
I didn’t think it would be over by now, but I didn’t think we’d be getting hit this hard this late. I thought we’d still just be smoldering. I didn’t know that we would just be a raging fire at this point in time. We’re not prepared for that, but here we are.
After this, I’m going to take my kids to a beach or somewhere.
GLENVIEW, ILL.
As of Dec. 7, Illinois has seen 796,264 total confirmed cases, 14,216 deaths, and 5,190 people are currently hospitalized with the virus.
Luisa Alog Penepacker, 51
ICU, Glenbrook Hospital
I’ve taken care of a lot of husband-wife patients, unfortunately. One of the cases was one in which the husband had tested positive for covid first, but he was a mild case. She was a little bit more serious. She ended up on our unit.
The husband ended up in the hospital the next day, but he was on the step-down unit. When I admitted her, she was terrified, especially knowing that her husband was upstairs in another unit. She was having a hard time breathing, and she grabbed onto my hand and looked at me. She goes, “Am I gonna die?” I mean, I didn’t know what to say. And I just told her, “Not on my watch.” So we just kept on going. But unfortunately, she got intubated the next day.
Then I was sent to work upstairs on the step-down unit. I had her husband that next day, and he was actually quite happy that I saw her. He goes, “You took care of my wife, how is she? I heard that she’s not doing well.” I didn’t know what to say to him, either. I just said, “You know, she’s in the best of care. We’ll take really good care of her.” And he looked really relieved. He goes, “I’m just so glad that someone who had seen her is here now to talk to me.” And my heart broke with that.
She ended up passing. A few days after, he went home, and I didn’t see him, so I don’t know how he took it. He wasn’t able to see her before she passed.
We wear personal air purification respirators on our heads — these big white domes over our heads with a respirator hose going to a machine strapped around our waist, and we look like astronauts walking through the unit, going in and out of patients’ rooms with our plastic gowns and gloves.
It can be frightening to family members if they’re allowed to come to visit and definitely for patients because we’re kind of scary-looking. It can be frantic at times. You walk through the hall, and you see a lot of patients on ventilators. You hear a lot of beeping. People are rounding constantly to check on patients. It’s a busy place.
You don’t know what to tell family members when you see them. What can you say? You just say, “I’m sorry.” You can’t even hug them. I used to be able to hug family members, but you can’t with all the gear.
When patients are scared, I will hold their hand even though I’m wearing gloves. I look them in the eyes as much as I can because really, that’s all you can see. You can’t see our faces. You can barely even hear past the mask. So I’ll make sure to look at them. I try to make an effort to smile with my eyes and to just hold their hand if they need it.
MURRAY, UTAH
As of Dec. 7, Utah has seen 215,407 total confirmed cases and 939 deaths.
Tammy Kocherhans, 41
Respiratory ICU, Intermountain Healthcare
These patients are different than the typical patient. They’re very complex. They can change in the blink of an eye. And it’s very hard as a nurse when you wrap your heart and soul into taking care of these patients. I started noticing that I was emotionally tired. I was physically completely exhausted. And I was beginning to question whether or not I could continue forward being a nurse at all. I was past my physical capacity.
I happened to be working a day where another health care worker who was a veteran said that this was like a combat zone, and for some reason in my head, that validated the way that I was feeling. So I reached out to one of my best friends who is a veteran, a flight medic, and he said, “I meditate and do yoga.”
Once I started doing that, I was able to handle the emotional crises, the physical pain of working so, so many long, hard hours. We do something called proning, where you take patients and flip them over onto their bellies. And that sounds really easy, but it takes a team of a minimum of five people. It is extremely taxing on your body. It hurts. And I lift weights! The meditation and yoga really has saved my life, my mental capacity, my spiritual capacity, my physical capacity, everything that is required to give to these patients.
Hopefully by 8 p.m., I’m out in the parking lot and spend a minute in my car to unload from my day. It’s all about taking a moment to breathe for myself and then going through whatever came up that day that I need to let go of. It depends on how complicated my patient was that day, whether I can let my whole day go or if I have to spend time to go through each piece and work it down to: What did I do right? Did I miss something? Sometimes I just can’t let some details go quickly, and I have to work them down to allow myself to say I did everything that I possibly could for this individual this day, in this time, in this situation. And whatever the outcome was or is, I followed protocol. I did everything that I knew how to do. And it’s going to be OK.
I find it very frustrating when I go out and about on my days off and I see people very blatantly not wearing masks or trying to tell me how come they don’t work or telling me that this pandemic isn’t real. I find it completely disrespectful to the work we do to save people’s lives, to have people think that this pandemic isn’t real, to show utter disregard for people around them, not trying to do their part.
And I really wish that I could take people on a day with me so that they can see what I see. So that they can feel your feet ache so bad that you wish they’d just fall off, because you’re on that concrete for so many hours. Your back aches because you’re wearing equipment to save your life — so that you can save somebody else’s life. And your head hurts. I’ve never had so many headaches in my life because part of the equipment sits on your head, and after 12 hours, it starts to exert so much pressure that you start to have a headache, and you’re dehydrated.
Early in the pandemic, I remember walking into this room, and this young patient was crying and asked me if they were going to die. And I’m a mom of teenagers. For me, that was awful because this patient was all alone, and we as staff were minimizing contact because we didn’t want to get the virus.
This patient started physically trembling in the bed. I couldn’t take it anymore, and I went over and just held this patient because that’s what I’d want somebody to do for my children. That was my first patient that I held like that. And there have been many since.
MURRAY, UTAH
As of Dec. 7, Utah has seen 215,407 total confirmed cases and 939 deaths.
Nate Smithson, 28
Respiratory ICU, IntermountainHealthcare
A few weeks ago, my wife and I were on a date at a restaurant. And in the middle of nowhere, I had this panic attack and went and hid in the bathroom stall for half an hour. I have no idea what brought it on. I just couldn’t handle being there right then, which was weird for me. That’s the first time anything like that has happened. But since then, it’s happened multiple times, where the anxiety and stress is overwhelming, and I can’t handle it. So I have to go and excuse myself for a little bit.
Balancing work and life is something that used to seem possible. Now it doesn’t seem like there is any difference between the two. I fall asleep and I dream about my patients.
When we got our first covid patient in February in the hospital, in the ICU, we all kind of thought it was a little bit of a joke, to be honest. I had this patient, and he was sitting there with minimal amounts of oxygen in the room just watching TV. He’s like, “I’m fine. I don’t know why everyone’s freaking out about this.” And I thought the same thing. And then a few hours later, he stands to go pee, and I’m looking at his monitor. And it drops down to the low 90s. Ninety-two is about as low as you want to go. And then it starts dropping down lower, to about the 70s. Then it gets down into the 60s and 50s. And that’s dangerous territory. That’s where brain cells start dying and you start having some serious problems.
I run into the room. We get him back into bed and throw all the oxygen that we have in the room on him, crank everything up, and he’s not recovering from it. We had to intubate right then and there. And about an hour later, he finally starts recovering a little bit. But at this point, he’s sedated, he’s on the ventilator. Everything is worse. And that’s the first time where it’s like: Oh, crap, this is serious. This is something else. I’ve never seen anything like that before.
If a patient’s heart stops or if they stop breathing, we call a code blue, and that’s when the doctor, respiratory therapist, nurses, everybody comes into the room. We start chest compressions or CPR or that kind of stuff. This one patient’s heart is not working. So I call the code blue. We all get in there. We start doing the chest compressions. Five minutes later, we get the patient back. We all go back about our work. Twenty minutes later, same thing happens again. We start doing the chest compressions. We start pushing medications as fast as we can to get the patient back again.
The spouse comes into the hospital. I explain: “Just so you know, this is what happened before. It could possibly happen again. If it does, I’m going to need you to step outside of the room.” And as I’m explaining this, sure enough, it happens again. We lose the pulse. We lose the heartbeat. So I ask her to leave the room. Everyone gets in there, and we start going for it. We went for almost two hours: chest compressions, pushing medications, shocking the patient’s heart.
The doctor is ultimately the one who makes the decision about when we stop, and they call time of death. But typically in situations like that, where it’s unexpected and sudden, they want to make sure that everybody can go home that night feeling OK about what they did, knowing that they did everything. And after an hour, he stops, turns to the room and asks: Does anyone have a problem with us stopping?
I didn’t have a problem, but then as he’s saying that, I look out the window, and the patient’s wife is just watching us. She’s been sitting out there watching us for an hour, and no one’s saying anything.
And I ask them to keep going.
So we did. We went almost for another hour after that, and we didn’t get the patient back. He ended up dying.
But I think for me, that was important — to keep going. Not because we thought we would get them back, but so that his wife would know that we did everything we could.
I still go to bed with her face kind of burned into my mind, of just seeing her sitting out there watching us, and that’s what kills me.
COLUMBUS, OHIO
As of Dec. 7, Ohio has seen 475,024 total confirmed cases and 6,959 deaths.
Kahlia Anderson, 32
ICU, Ohio State University Wexner Medical Center
I graduated from nursing school in May 2019. I started here at the Wexner in August. Our orientation is a 20-week program, and so I came out on my own Jan. 12, 2020. The pandemic hit us at the end of February.
In nursing school, I think your biggest fears are making med errors, or harming your patient in some way, or just not knowing how to do everything. Did I check my patient’s blood pressure before I gave this blood pressure medication, or did I give the correct dose of a specific medication? I had heard stories about that on the unit, like make sure you’re careful with the needle stick, or make sure you’re careful with this medication. And I don’t even think about those kinds of things anymore.
Now it’s the fear of the unknown. It’s the fear that anything could happen because of this virus and my patient could die regardless of what I do.
When I got my first covid-positive patient, I remember thinking: Somebody did the assignment wrong because there’s no way that they believe that I should be taking care of this patient. I can remember the feeling. I can remember the day. It was a weekend. I was on a day shift. And I was thinking to myself: Who trusted me, the new nurse to take care of a covid-positive patient? How am I going to do this? How am I going to keep this patient safe? How am I going to keep myself safe? Am I safe? Wait, who cares about me? Let’s get back to the patient. What do they need?
At the time, I didn’t even understand some of the ventilator settings because I was still that new, and it was still that fresh to me. And I thought: This machine is doing that much work for them, and I don’t know enough about it, but I’m going to make sure that I get it done and I’m going to figure it out today to make sure that this patient gets everything that they need. And I’m going to call their family and double check with them and check in with them and call them.
That patient is alive. That patient is no longer in the hospital. As far as I know, that patient is home and safe with family.
I would feel like: There’s someone more experienced. There’s someone more adequate to deal with this. And I was like — oh, it’s me. This is me, I’m doing this, and I’ve been doing it ever since.
I saw new nurses come out of orientation, and I saw the type of assignments that they would get. So my mind fixated on like: I’m going to get patients that are ready to transfer out. They can talk, they can eat. They’re just waiting for a bed on another unit. Or maybe it’s a patient who needs long-term care. So they’re waiting to go to a facility to be discharged. And so I was thinking to myself: I’m going to get my feet wet. It’s going to be great. I’m going to build up this experience, and then I’m going to start getting sicker patients, and I’m going to be ready.
Once covid hit, there was no room for those types of patients anymore. Everyone had covid, everyone was sick, everyone was intubated or approaching intubation.
And for me, I just wanted my first experience. I wanted to have the simple experience of building and getting better. But that’s not what was in store. And I can’t say that I’m upset about it today. I’m grateful for this experience. I don’t wish this pandemic on anyone. I wish it was not here. I wish that it was different. But as a nurse, as a new nurse, these experiences are unique to me. It’s making me a better nurse. It’s made me a better person, and I can only continue to just be.
We did cry in the beginning, and now not so much. I think we all struggled when we had a young death. Someone in their 20s was very difficult for us. Because you think: That was a young life. What a young life that was, and they’re not here anymore. Because of a virus. That’s hard. It’s very hard.