The Republican Study Committee (RSC), a group of 145 House GOP lawmakers, rolled out a new healthcare plan to counter Democrats’ call for “Medicare for All.”
However, the plan itself closely resembles the Affordable Care Act (ACA) repeal bill called the American Health Care Act (AHCA) that the House passed in 2017 and contributed greatly to the loss of the GOP House majority in 2018.
For the plan to become law, Republicans would have to retake the House in 2020, and President Donald Trump would need to be reelected. However, if those victories happen, the plan could be a blueprint for how a GOP-controlled Congress would move forward on healthcare, as the committee counts among its members both GOP leadership and rank and file.
Here are three takeaways from the plan:
Shifting to high-risk pools
The plan would retain the ACA’s requirement that individual market plans cover pre-existing conditions. However, it takes out provisions that ensure patients with pre-existing conditions get affordable coverage such as requirements that prevent plans from charging sicker people higher premiums than healthy customers.
The plan does introduce high-risk pools that would be used by people with high healthcare costs, a commonly deployed tactic by states for the individual market before the ACA. The high-risk pools would be funded by repackaging the funding used for the ACA’s subsidies and the Medicaid expansion.
However, the plan doesn’t identify the full amount that should be devoted to high-risk pools, which segregate high-cost customers on the individual market.
The plan cites a 2017 report from consulting firm Milliman that estimated a federally supported high-risk pool could require $3.3 billion to $16.7 billion a year. The AHCA also called for high-risk pools but only gave $2.5 billion a year to help states fund them.
While the “$17 billion annual price tag may not seem ideal, it sets up a sustainable path for the individual market,” the RSC report said.
The desire for more funding for high-risk pools is likely a nod to Democratic attacks during the 2018 midterms that the AHCA threatened pre-existing condition protections. The nonpartisan Congressional Budget Office said the AHCA, which let states waive pre-existing condition protections, would lead to people in those states not getting affordable coverage for their pre-existing conditions.
While the AHCA had funding for high-risk pools, experts across the healthcare spectrum said that it wasn’t enough. It would remain to be seen how much more funding would be needed.
Doubling down again on health savings accounts
Bolstering health savings accounts has been a very popular reform idea among Republicans, and that enthusiasm is clear in the RSC plan.
The plan proposes to increase how much an employee can contribute to a health savings account. Currently, an individual can contribute $3,500 and a family can contribute $7,000.
A 2018 bill that passed out of the House but didn’t make it through Congress increased the contribution cap to $6,650 for an individual and $13,300 for a family.
Now, the RSC plan wants to increase the figures again, this time to $9,000 per individual and $18,000 for families, in line with a proposal from libertarian think tank Cato Institute.
“The RSC plan would also expand health savings accounts so that they could be used for a number of health services and products that currently must be paid for with after-tax dollars,” the plan said.
Replace Medicaid expansion with a block grant
This is another common reform in ACA repeal plans. The bill would phase out the enhanced federal matching rate for the Medicaid expansion to pre-expansion levels.
In addition, the bill would replace the existing open-ended federal match with a fixed amount in a block grant.
But the plan has a new twist in a new “flex-grant” that would give more funding to states that adopt a work requirement. However, half of the funding for any flex-grant must go toward supporting the purchase of private plans for low-income individuals.
So far, 12 states have gotten approval from the Trump administration to install work requirements for their Medicaid expansion population. But of those 12 states, three have had their work requirement programs struck down by legal challenges.
Some states are also considering installing their own block grants. Tennessee has released a draft proposal for a block grant but has yet to get federal approval.







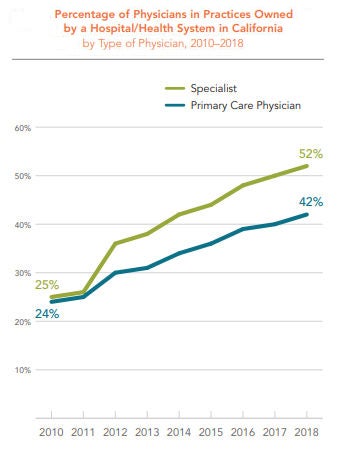
 The percentage of physicians in practices owned by a hospital or health system increased dramatically in California between 2010 and 2018 — from 24% in 2010 to 42% in 2018. The percentage of specialists in practices owned by a hospital or health system rose even faster, from 25% in 2010 to 52% in 2018.
The percentage of physicians in practices owned by a hospital or health system increased dramatically in California between 2010 and 2018 — from 24% in 2010 to 42% in 2018. The percentage of specialists in practices owned by a hospital or health system rose even faster, from 25% in 2010 to 52% in 2018.