In the era of great awakening, leaders have to step up and be conscious about building trust with people they work with.
The old rules and hierarchies, that were already becoming obsolete, have now been thrown out of the window. People look for integration of work and well-being knowing that work is what you do, not a place you go to.
Opportunities are abound and excellent people have ample choices (they always had). It is high time that organizations and leaders think this through carefully to first align their own mindset to this new reality and then take conscious actions to build teams, practices and processes that are not just high-performing but also have a strong fabric of trust woven in.
Employees, after all, are volunteers who exercise their choice of working with you. Effective leadership is about making it worth for them.
Building high-trust environment means putting the human back at the center of how a business functions and building everything – purpose, culture, processes, structures, rituals, systems, tools and mindsets – around it.
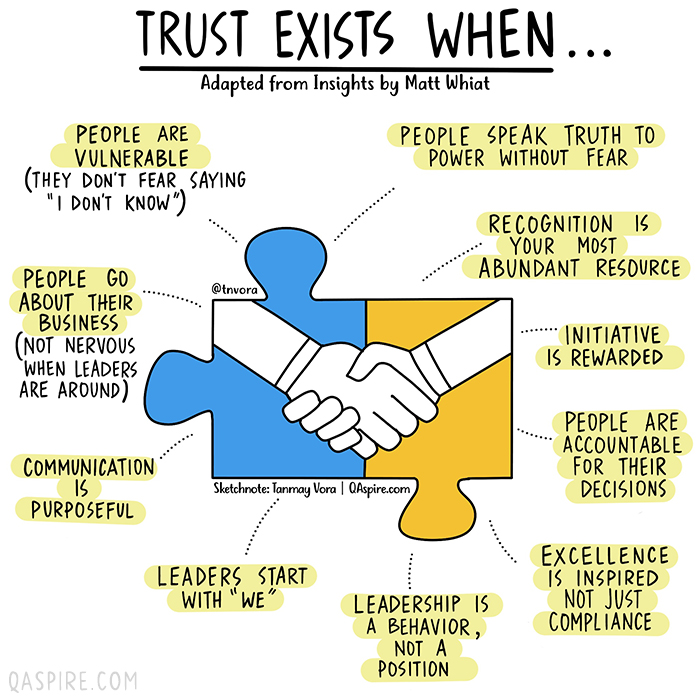
How would we know if we are working in an environment where we can trust others and that we are trusted? We can always answer this based on our intrinsic feeling but if you are a leader who is working hard to build trust, here are a few vital signs that you need to look for.
The healthcare industry’s staffing shortage crisis has had clear consequences for care delivery and efficiency, forcing some health systems to pause nonemergency surgeries or temporarily close facilities. Less understood is how these shortages are affecting care quality and patient safety.
A mix of high COVID-19 patient volume and staff departures amid the pandemic has put hospitals at the heart of a national staffing shortage, but there is little national data available to quantify the shortages’ effects on patient care.
The first hint came last month from a CDC report that found healthcare-associated infections increased significantly in 2020 after years of steady decline. Researchers attributed the increase to challenges related to the pandemic, including staffing shortages and high patient volumes, which limited hospitals’ ability to follow standard infection control practices.
“That’s probably one of the first real pieces of data — from a large scale dataset — that we’ve seen that gives us some sense of direction of where we’ve been headed with the impact of patient outcomes as a result of the pandemic,” Patricia McGaffigan, RN, vice president of safety programs for the Institute for Healthcare Improvement, told Becker’s. “I think we’re still trying to absorb much of what’s really happening with the impact on patients and families.”
An opaque view into national safety trends
Because of lags in data reporting and analysis, the healthcare industry lacks clear insights into the pandemic’s effect on national safety trends.
National data on safety and quality — such as surveys of patient safety culture from the Agency for Healthcare Research and Quality — can often lag by several quarters to a year, according to Ms. McGaffigan.
“There [have been] some declines in some of those scores more recently, but it does take a little while to be able to capture those changes and be able to put those changes in perspective,” she said. “One number higher or lower doesn’t necessarily indicate a trend, but it is worth really evaluating really closely.”
For example, 569 sentinel events were reported to the Joint Commission in the first six months of 2021, compared to 437 for the first six months of 2020. However, meaningful conclusions about the events’ frequency and long-term trends cannot be drawn from the dataset, as fewer than 2 percent of all sentinel events are reported to the Joint Commission, the organization estimates.
“We may never have as much data as we want,” said Leah Binder, president and CEO of the Leapfrog Group. She said a main area of concern is CMS withholding certain data amid the pandemic. Previously, the agency has suppressed data for individual hospitals during local crises, but never on such a wide scale, according to Ms. Binder.
CMS collects and publishes quality data for more than 4,000 hospitals nationwide. The data is refreshed quarterly, with the next update scheduled for October. This update will include additional data for the fourth quarter of 2020.
“It is important to note that CMS provided a blanket extraordinary circumstances exception for Q1 and Q2 2020 data due to the COVID-19 pandemic where data was not required nor reported,” a CMS spokesperson told Becker’s. “In addition, some current hospital data will not be publicly available until about July 2022, while other data will not be available until January 2023 due to data exceptions, different measure reporting periods and the way in which CMS posts data.”
Hospitals that closely monitor their own datasets in more near-term windows may have a better grasp of patient safety trends at a local level. However, their ability to monitor, analyze and interpret that data largely depends on the resources available, Ms. McGaffigan said. The pandemic may have sidelined some of that work for hospitals, as clinical or safety leaders had to shift their priorities and day-to-day activities.
“There are many other things besides COVID-19 that can harm patients,” Ms. Binder told Becker’s. “Health systems know this well, but given the pandemic, have taken their attention off these issues. Infection control and quality issues are not attended to at the level of seriousness we need them to be.”
What health systems should keep an eye on
While the industry is still waiting for definitive answers on how staffing shortages have affected patient safety, Ms. Binder and Ms. McGaffigan highlighted a few areas of concern they are watching closely.
The first is the effect limited visitation policies have had on families — and more than just the emotional toll. Family members and caregivers are a critical player missing in healthcare safety, according to Ms. Binder.
When hospitals don’t allow visitors, loved ones aren’t able to contribute to care, such as ensuring proper medication administration or communication. Many nurses have said they previously relied a lot on family support and vigilance. The lack of extra monitoring may contribute to the increasing stress healthcare providers are facing and open the door for more medical errors.
Which leads Ms. Binder to her second concern — a culture that doesn’t always respect and prioritize nurses. The pandemic has underscored how vital nurses are, as they are present at every step of the care journey, she continued.
To promote optimal care, hospitals “need a vibrant, engaged and safe nurse workforce,” Ms. Binder said. “We don’t have that. We don’t have a culture that respects nurses.”
Diagnostic accuracy is another important area to watch, Ms. McGaffigan said. Diagnostic errors — such as missed or delayed diagnoses, or diagnoses that are not effectively communicated to the patient — were already one of the most sizable care quality challenges hospitals were facing prior to the pandemic.
“It’s a little bit hard to play out what that crystal ball is going to show, but it is in particular an area that I think would be very, very important to watch,” she said.
Another area to monitor closely is delayed care and its potential consequences for patient outcomes, according to Ms. McGaffigan. Many Americans haven’t kept up with preventive care or have had delays in accessing care. Such delays could not only worsen patients’ health conditions, but also disengage them and prevent them from seeking care when it is available.
Reinvigorating safety work: Where to start
Ms. McGaffigan suggests healthcare organizations looking to reinvigorate their safety work go back to the basics. Leaders should ensure they have a clear understanding of what their organization’s baseline safety metrics are and how their safety reports have been trending over the past year and a half.
“Look at the foundational aspects of what makes care safe and high-quality,” she said. “Those are very much linked to a lot of the systems, behaviors and practices that need to be prioritized by leaders and effectively translated within and across organizations and care teams.”
She recommended healthcare organizations take a total systems approach to their safety work, by focusing on the following four, interconnected pillars:
Culture, leadership and governance
Patient and family engagement
Learning systems
Workforce safety
For example, evidence shows workforce safety is an integral part of patient safety, but it’s not an area that’s systematically measured or evaluated, according to Ms. McGaffigan. Leaders should be aware of this connection and consider whether their patient safety reporting systems address workforce safety concerns or, instead, add on extra work and stress for their staff.
Safety performance can slip when team members get busy or burdensome work is added to their plates, according to Ms. McGaffigan. She said leaders should be able to identify and prioritize the essential value-added work that must go on at an organization to ensure patients and families will have safe passage through the healthcare system and that care teams are able to operate in the safest and healthiest work environments.
In short, leaders should ask themselves: “What is the burdensome work people are being asked to absorb and what are the essential elements that are associated with safety that you want and need people to be able to stay on top of,” she said.
To improve both staffing shortages and quality of care, health systems must bring nurses higher up in leadership and into C-suite roles, Ms. Binder said. Giving nurses more authority in hospital decisions will make everything safer. Seattle-based Virginia Mason Hospital recently redesigned its operations around nurse priorities and subsequently saw its quality and safety scores go up, according to Ms. Binder.
“If it’s a good place for a nurse to go, it’s a good place for a patient to go,” Ms. Binder said, noting that the national nursing shortage isn’t just a numbers game; it requires a large culture shift.
Hospitals need to double down on quality improvement efforts, Ms. Binder said. “Many have done the opposite, for good reason, because they are so focused on COVID-19. Because of that, quality improvement efforts have been reduced.”
Ms. Binder urged hospitals not to cut quality improvement staff, noting that this is an extraordinarily dangerous time for patients, and hospitals need all the help they can get monitoring safety. Hospitals shouldn’t start to believe the notion that somehow withdrawing focus on quality will save money or effort.
“It’s important that the American public knows that we are fighting for healthcare quality and safety — and we have to fight for it, we all do,” Ms. Binder concluded. “We all have to be vigilant.”
Conclusion
The true consequences of healthcare’s labor shortage on patient safety and care quality will become clear once more national data is available. If the CDC’s report on rising HAI rates is any harbinger of what’s to come, it’s clear that health systems must place renewed focus and energy on safety work — even during something as unprecedented as a pandemic.
The irony isn’t lost on Ms. Binder: Amid a crisis driven by infectious disease, U.S. hospitals are seeing higher rates of other infections.
“A patient dies once,” she concluded. “They can die from COVID-19 or C. diff. It isn’t enough to prevent one.”
A lot of communication in the workplace is conducted electronically. However, it is essential for hospital and health system leaders to have face-to-face conversations with employees in some situations.
Becker’s asked healthcare executives to share the interactions they prioritize when they’re in person at their organizations. Many expressed their preference for the deeper connections in-person interactions allow, citing inspiration and team building as reasons to facilitate face-to-face communication. Below are their responses:
Russell F. Cox. President and CEO of Norton Healthcare (Louisville, Ky.): Healthcare, by its very nature, requires in-person interactions.
With the onset of the COVID-19 pandemic, we made a quick and successful shift to virtual visits for the safety of our patients and providers. This enabled patients with a variety of time and transportation constraints to receive convenient care from a trusted provider. However, telemedicine will never completely replace in-person visits, and the opportunity for our patients and community to interact in-person with our patient care providers is very important to me, and to our team.
And, although the pandemic created the need for virtual meetings, I have always prioritized in-person interactions and meetings with all team members. Whether that be rounding in our hospitals and facilities, holding in-person meetings, celebrating employee accomplishments or milestones, or dropping by one of our community vaccine or testing centers — web meetings will never replace what can be accomplished face to face. It became even more important to interact in person with our caregivers and employees during the pandemic. It was important to show my support for their hard work and extraordinary sacrifices during this time. I’m thankful that with the vaccine, more in-person events, with proper safety precautions, are resuming.
Our motto has been and continues to be: Stay safe. Keep the faith.
Jim Dunn, PhD. Executive Vice President and Chief People and Culture Officer of Atrium Health (Charlotte, N.C.): Recognition is part of our organizational DNA, and in-person delivery is an essential component of that — especially as we continue working through the COVID-19 pandemic. One thing our teammates love is the “Surprise Patrol,” which we employ for some of our most special and meaningful awards, such as our annual Pinnacle Award — the highest award given by our organization to those who best exemplify our Culture Commitments: Belong, Work as One, Trust, Innovate and Excellence. Executives, leaders, teammates and loved ones come together to celebrate honorees with balloons, cupcakes, cheers and even a few happy tears. Our honorees are shocked, uplifted and proud to be recognized in-person for their outstanding accomplishments, and our “Surprise Patrol” participants are honored to be a part of such a special moment. Whether we’re celebrating small wins, personal successes, birthdays or prestigious awards, in-person recognition — where and when possible — is a vital part of the teammate experience and culture at Atrium Health.
Robert Gardner. CEO of Banner Ironwood Medical Center (Queen Creek, Ariz.) and Banner Goldfield Medical Center (Apache Junction, Ariz.): Over the past few years in particular, I’ve spent some time reflecting on the differences between motivation and inspiration. More often than not, it seems like leaders don’t know the differences and often confuse the two as being synonymous or interchangeable. Put in overly simplified terms, I see motivation as being the metaphorical carrot or the stick. We can motivate with reward (aka the carrot) and with discipline (aka the stick), and both are used frequently in life. Motivation tends to be more surface level. However, inspiration is something much deeper, more intimate, and therefore much more complex. Inspiration is getting to a point of genuinely desiring to change, do more, be better, etc.
For me, knowing the differences is critical when it comes to prioritizing being in person in the workplace. Virtual meetings, emails, newsletters and other forms of electronic communication can work incredibly well when it comes to items of motivation; and believe me, there are plenty of these items. However, when it comes time to inspire the team, I heavily prioritize these meetings to take place in person. Items that fall into this category will be mission-critical initiatives and overall reminders on living our mission, purpose values, etc. It’s so ironic to me that despite the increasing complexity, regulation, bureaucracy and proverbial red tape that healthcare has become famous for, that an inspirational dose of simplicity has more effect on change than any other bestseller leadership book on how to motivate performance through some sort of complicated multistep process.
Brian Koppy. Chief Financial Officer of Cano Health (Miami): As a rapidly growing primary care provider, we have found that face-to-face interactions at our offices are as essential as they are in our medical centers. Our providers provide the best care when they see patients in person because it builds lifelong bonds that improve patient outcomes. In our offices, our team members feel more connected and integrated into the Cano Health family when we are together, both formally and informally. This, of course, does not mean we do not have a flexible work environment, which we do. It simply means our priority is on the employee benefits and outcomes that come from working in the office.
At the beginning of the pandemic, we moved many corporate employees to remote work and moved about 95 percent of our patient interactions to televisits. That did not last long, however. Within a month or two, our employees were asking to come back to the office. Our medical centers never closed their doors, and our visits rapidly returned to mostly in person.
It’s the seemingly inconsequential daily interactions that often have the greatest impact on a company’s employees and their connection to the mission, values and culture of the organization. The quick stop-ins to someone’s workstation, the chance hallway encounters, the team lunches — these are so important in developing relationships and, in turn, maximizing efficiency. Employees who know and personally interact with each other work better together. They discuss ideas, they strategize freely, and they execute on the company’s goals together and more effectively.
At Cano Health, our high-touch approach to primary care is key to our success. And we believe that daily face-to-face interactions among employees are equally important to create a rewarding experience for our employees, but also expanding Cano Health’s services across the country.
Christopher O’Connor. President and incoming CEO of Yale New Haven (Conn.) Health:We are prioritizing one-on-one meetings and small groups. With our vaccination mandate, we feel it is critical to have that in-person contact and fill that void that video can’t replicate. This is a relationship business, and spending the time to build and nurture those relationships is critical.
Thomas J. Senker. President of MedStar Montgomery Medical Center (Olney, Md.): Before and especially during the pandemic our priority has been the well-being and engagement of our front-line staff and essential personnel. And while in-person activities have been limited, our executive team makes regular rounds visiting each unit, expressing gratitude, providing snacks and refreshments, and sharing important hospital updates directly. We believe these face-to-face interactions are critical opportunities to gain feedback and focus on areas of improvement across different areas of MedStar Montgomery Medical Center’s operations.