A new report from the Georgetown University Health Policy Institute says the number of uninsured children in the U.S. increased by more than 400,000 between 2016 and 2018.
Some key findings from the report:
The number of uninsured children rose above 4 million by the end of 2018.
Insurance coverage losses are concentrated in 15 states — Alabama, Arizona, Florida, Georgia,
Idaho, Illinois, Indiana, Missouri, Montana, North Carolina, Ohio, Tennessee, Texas, Utah, West Virginia.
States that have not expanded Medicaid, as allowed by the Affordable Care Act, have seen much larger increases in uninsured rates.
Children in non-expansion states are nearly twice as likely to be uninsured compared to states that have expanded Medicaid.
White and Latino children saw the largest increases in the uninsured rate.
Households with low to moderate income – $29,000 to $53,000 per year for a family of three – were the hardest hit.
The report’s authors said it’s no coincidence that the increases in the number of uninsured children have occurred since President Trump took office in 2017.
“This serious erosion of child health coverage is likely due in large part to the Trump Administration’s actions that have made health coverage harder to access and have deterred families from enrolling their eligible children in Medicaid and CHIP,” they wrote in their conclusion. “These actions include attempting to repeal the ACA and deeply cut Medicaid, cutting outreach and advertising funds, encouraging states to put up more red tape barriers that make it harder for families to enroll or renew their eligible children in Medicaid or CHIP (or ignoring it when they do), eliminating the ACA’s individual mandate penalty, and creating a pervasive climate of fear and confusion for immigrant families.”
Supporters of Medicaid expansion in Oklahoma said they submitted more than enough signatures on Thursday to get the measure on the ballot in 2020.
The “Yes on 802” campaign said it submitted more than 313,000 signatures, far more than the roughly 178,000 it needed, to qualify to get Medicaid expansion on the ballot in Oklahoma next year.
Campaign manager Amber England said in a statement that her group had “a mandate from a record-breaking number of Oklahoma voters who want the chance to bring more than a billion of our tax dollars home from Washington every single year to deliver healthcare to our neighbors, keep our rural hospitals open, and boost our economy.”
Oklahoma is one 14 GOP-controlled states that have not accepted the expansion of Medicaid under ObamaCare. Republicans have traditionally raised concerns about the cost of the program.
More states have been expanding recently, however. Utah, Idaho and Nebraska voters approved ballot measures approving Medicaid expansion in last year’s elections.
The Yes on 802 campaign estimates almost 200,000 people in Oklahoma would gain coverage if expansion were adopted in next year’s election.
The Oklahoma Council of Public Affairs, a conservative think tank in the state, has vowed an opposition effort.
“There will obviously be significant opposition once it gets to the campaign stage,” the group’s president, Jonathan Small, told The Oklahoman earlier this month.
The Republican Study Committee (RSC), a group of 145 House GOP lawmakers, rolled out a new healthcare plan to counter Democrats’ call for “Medicare for All.”
However, the plan itself closely resembles the Affordable Care Act (ACA) repeal bill called the American Health Care Act (AHCA) that the House passed in 2017 and contributed greatly to the loss of the GOP House majority in 2018.
For the plan to become law, Republicans would have to retake the House in 2020, and President Donald Trump would need to be reelected. However, if those victories happen, the plan could be a blueprint for how a GOP-controlled Congress would move forward on healthcare, as the committee counts among its members both GOP leadership and rank and file.
Here are three takeaways from the plan:
Shifting to high-risk pools
The plan would retain the ACA’s requirement that individual market plans cover pre-existing conditions. However, it takes out provisions that ensure patients with pre-existing conditions get affordable coverage such as requirements that prevent plans from charging sicker people higher premiums than healthy customers.
The plan does introduce high-risk pools that would be used by people with high healthcare costs, a commonly deployed tactic by states for the individual market before the ACA. The high-risk pools would be funded by repackaging the funding used for the ACA’s subsidies and the Medicaid expansion.
However, the plan doesn’t identify the full amount that should be devoted to high-risk pools, which segregate high-cost customers on the individual market.
The plan cites a 2017 report from consulting firm Milliman that estimated a federally supported high-risk pool could require $3.3 billion to $16.7 billion a year. The AHCA also called for high-risk pools but only gave $2.5 billion a year to help states fund them.
While the “$17 billion annual price tag may not seem ideal, it sets up a sustainable path for the individual market,” the RSC report said.
The desire for more funding for high-risk pools is likely a nod to Democratic attacks during the 2018 midterms that the AHCA threatened pre-existing condition protections. The nonpartisan Congressional Budget Office said the AHCA, which let states waive pre-existing condition protections, would lead to people in those states not getting affordable coverage for their pre-existing conditions.
While the AHCA had funding for high-risk pools, experts across the healthcare spectrum said that it wasn’t enough. It would remain to be seen how much more funding would be needed.
Doubling down again on health savings accounts
Bolstering health savings accounts has been a very popular reform idea among Republicans, and that enthusiasm is clear in the RSC plan.
The plan proposes to increase how much an employee can contribute to a health savings account. Currently, an individual can contribute $3,500 and a family can contribute $7,000.
A 2018 bill that passed out of the House but didn’t make it through Congress increased the contribution cap to $6,650 for an individual and $13,300 for a family.
Now, the RSC plan wants to increase the figures again, this time to $9,000 per individual and $18,000 for families, in line with a proposal from libertarian think tank Cato Institute.
“The RSC plan would also expand health savings accounts so that they could be used for a number of health services and products that currently must be paid for with after-tax dollars,” the plan said.
Replace Medicaid expansion with a block grant
This is another common reform in ACA repeal plans. The bill would phase out the enhanced federal matching rate for the Medicaid expansion to pre-expansion levels.
In addition, the bill would replace the existing open-ended federal match with a fixed amount in a block grant.
But the plan has a new twist in a new “flex-grant” that would give more funding to states that adopt a work requirement. However, half of the funding for any flex-grant must go toward supporting the purchase of private plans for low-income individuals.
So far, 12 states have gotten approval from the Trump administration to install work requirements for their Medicaid expansion population. But of those 12 states, three have had their work requirement programs struck down by legal challenges.
Some states are also considering installing their own block grants. Tennessee has released a draft proposal for a block grant but has yet to get federal approval.
There has been confusion over estimates, like ours, that measure the effect of single-payer (i.e., Medicare for All) proposals on both federal spending and total national health spending.
The two are not the same, and too frequently, people use estimates of both and make misleading apples-to-oranges comparisons.
Federal spending versus national spending
Federal health care spending is the money the federal government spends on health care, whereas national health spending includes all health spending, regardless of who pays for it.
Federal health care spending includes spending on Medicare, Medicaid, the Children’s Health Insurance program, Affordable Care Act Marketplace premium subsidies, the Veterans Administration, US Department of Defense health care programs, support for health care professionals and hospitals providing uncompensated care, as well as other federal programs.
Changes in federal health spending represent amounts that would either need to be added to the federal budget (and funded through tax increases or additional government debt) or which would lead to cuts in other federal programs to free up sufficient federal funds.
National health care spending includes spending by the federal government, state and local governments, households, and employers. National health expenditures (NHE) are estimated annually by the Centers for Medicare and Medicaid Services (CMS) as the National Health Expenditure Accounts. Using our models’ projections and extending the CMS’s estimate for spending categories we do not model, we estimate that NHE for the 10-year period from 2020 to 2029 will total approximately $52 trillion dollars under current law.
What increases or decreases in these estimates mean
It is possible, for example, for federal spending to increase while national health spending decreases, if new federal programs take over some of the expenses currently paid for by employers and households and do it at a lower cost.
But if a federal program takes over some of the private spending and ends up providing more generous benefits, total national spending could still increase. Regardless, it is important to separate changes in federal spending from changes in national spending to understand the implications of any health care reform approach.
In our most recent report, we estimate that a broad single-payer reform (referred to as Reform 8: Enhanced Single Payer in the report) would increase federal government spending by $34 trillion over the 2020–29 period, $34 trillion beyond what the federal government already spends on health care.
However, this reform would shift almost all of the spending currently done by households, employers, and state governments over to the federal government. All people, regardless of whether they have insurance coverage today, would be covered by the new federal program.
How single-payer reform would affect federal and national spending
Under the single-payer enhanced reform, the new federal government program would provide more covered benefits than typical insurance offers today (including typical medical benefits but adding a new home- and community-based long-term services and supports benefit and adult dental, vision, and hearing benefits). All the costs would be covered by the federal government; no one would pay premiums or out-of-pocket costs (i.e., no deductibles and no copayments or coinsurance), including undocumented residents.
As a result, many people would get insurance for the first time, and many others would get significantly more generous insurance than they currently have. And with their new or improved insurance, many people would use more medical care than they do today.
The federal government would limit the fees paid to doctors, hospitals, and prescription drug manufacturers, which would help lower the program’s costs, compared with what it would be otherwise. In addition, the system would be simpler than our current “patchwork” system, so the administrative costs of running the program would be lower than in most private insurance plans; this also helps offset some of the new costs.
However, by our estimates, the increase in spending for people with this new generous coverage would outweigh the savings from lower prices for health care providers and lower administrative costs. As a result, total national spending would increase, even taking into account greatly reduced household, employer, and state government spending.
For this approach to reform, federal spending would increase by $34 trillion over 10 years, but health spending by individuals, employers, and state governments would decrease by $27 trillion, so national health spending would increase by $7 trillion over the same 10-year period, from $52 to $59 trillion.
The figure below illustrates our estimates. In the first bar, we divide the $52 trillion estimated current-law spending on health care over 2020–29 into three pieces: $17 trillion in federal spending; $27 trillion in private spending and state and local government spending for medical care and dental care that would be subsumed into the new single-payer program; and $8 trillion in spending (a mix of government and private spending) that would not be affected by a single-payer program.
The $8 trillion includes costs associated with an array of expenses, such as medical care for members of the military and their families while military members are deployed, services provided to foreign visitors, acute care provided to people living in institutions (e.g., prisons and nursing homes), and the value of new construction and equipment put in place by the medical sector. This spending also includes long-term services and supports by states and individuals that would continue under reform. For our purposes here, we refer to this $8 trillion in spending as “spending not affected by single-payer.”
The taller second bar shows that the total national spending under a single-payer program would be higher than under current law. The $17 trillion in federal spending under current law would be shifted to help fund the new program, and the federal government would take over the $27 trillion in current health care spending by employers, households, and state and local governments.
Fully funding a new single-payer program would require an additional $7 trillion in federal spending beyond that repurposed $44 trillion. The $8 trillion in spending not affected by the single-payer program would continue to be funded by a mix of government and private sources.
Thus, it is not appropriate to compare an estimated increase in federal spending of $34 trillion over 10 years with a current-law level of national health spending of $52 trillion over the same period and conclude these are savings in national health spending.
And although many advocates believe that a single-payer system would increase federal spending but with the benefit of reducing national health spending, our estimates contradict that. According to our analysis, a broad single-payer reform, similar to current Medicare for All bills, would increase federal spending and increase national spending.
But as our full report also shows, a single-payer program can be designed to decrease national health spending, as can other approaches to achieving universal coverage.
From deaths and injuries caused by extreme heat and stronger storms to longer growing seasons linked to an increased risk of mosquito- and tick-borne illnesses and wildfires, the healthcare impacts of climate change are costing the U.S. billions, a new analysis found.
Case in point: An analysis of a single year—2012—by researchers at the Natural Resource Defense Council and the University of California, San Francisco (UCSF) estimated a total of 10 climate-sensitive events in the U.S. that ultimately cost $10 billion.
That estimate stems from costs associated with 917 deaths, 20,568 hospitalizations and 17,857 emergency room visits, researchers said in the study published in the journal GeoHealth.
Among the costs connected to “climate-sensitive events” in 2012, researchers pointed to:
$252 million in Wisconsin: A heatwave led to several record temperatures were broken over the span of a week in July 2012. Researchers analyzed costs from an estimated 27 deaths, 155 hospitalizations and 1,620 emergency room visits that summer.
$1.6 billion in Colorado and $2.3 billion in Washington: Longer fire seasons in the western U.S. have resulted from higher temperatures and changes in seasonal rainfall patterns. Researchers examined costs from direct wildfire deaths and impacts attributed to wildfire smoke in 2012. There were 174 deaths, 256 hospitalizations and 1,432 emergency room visits in Colorado and 245 deaths, 371 hospitalizations and 1,897 emergency room visits in Washington.
$3.1 billion in New Jersey and New York: Hurricane Sandy caused severe flooding and power outages for more than 20 million customers. Sea level rise is believed to have amplified the storm surge. Researchers estimate there were 273 hurricane-related deaths, 6,602 hospitalizations and 4,673 emergency room visits.
Researchers said mortality costs were estimated using a mortality risk valuation implemented by the U.S. Environmental Protection Agency in regulatory impact analyses, with each life lost valued at $9.1 million in 2018 dollars. They also factored direct morbidity costs for each event using hospital admissions and emergency department visits from the federal Healthcare Cost and Utilization Project data well as costs associated with outpatient visits, home health care costs and prescribed drugs from the federal Medical Expenditure Panel Survey.
They acknowledged several limitations of the study. For instance, they said, “despite record-setting weather conditions across the U.S. in 2012, our analysis was restricted to case studies for which there was adequate documentation of health impacts,” they said.
They only included mental health impacts from Hurricane Sandy despite evidence that other events like wildfires can also adversely impact mental health. They also said extreme heat and Lyme disease are routinely underreported health effects that could result in conservative estimates.
“As such, the $10 billion total we calculated is likely a conservative estimate of health-related costs for these studies,” researchers said in this study.
Still, these costs are not just theoretical, but tangible costs that should be factored into the policy conversation, said Wendy Max, co-director of the Institute for Health & Aging at UCSF.
“We wanted to look at who bears this cost and we found two-thirds of the cost are borne by the Medicaid and Medicare programs,” Max said. “In an era of concern about healthcare costs, this is an important message: Climate change is adding to the public healthcare cost burden. That’s a message we’re hoping will resonate with policymakers.”
Roughly 27.5 million people, or 8.5% of the U.S. population, had no health insurance at some point in 2018, according to new figures from the Census Bureau.
Why it matters: Last year’s uninsured rate increased from 7.9% in 2017 — the first time the uninsured rate has gone up since the Affordable Care Act has been in effect.
Between the lines: The uninsured population does not include the “underinsured,” or people who have medical coverage but face prohibitively high deductibles and out-of-pocket costs.
The figure also does not include people who have short-term plans, association plans and religious-based sharing ministries — policies the Trump administration has promoted, but that have holes in coverage that could leave people on the hook for high costs.
The intrigue: The type of coverage that witnessed the largest decline in 2018 was Medicaid, which fell 0.7 percentage points.
4 states where the uninsured rate had a statistically significant increase were Alabama, Idaho, Tennessee and Texas, all of which have not fully expanded Medicaid under the ACA.
The bottom line: The uninsured rate is still markedly lower before the ACA became law, but it’s an odd paradox to see more people lose health coverage even though the economy created more jobs.
States use the Commonwealth Fund’s 2019 Scorecard on State Health System Performance to identify places where their health care policies are on track and areas that need improvement. Using the Scorecard, states can compare their improvement to others, and see how they stack up. In the most recent edition, released in June, Rhode Island improved on the most health system performance indicators tracked over time, followed by Missouri, Washington, West Virginia, and Arkansas.
Rhode Island particularly made strides in the areas of coverage and behavioral health. The state uninsured rate among adults dropped from 17 percent in 2013 to 7 percent in 2015 and 6 percent in 2017. In addition, the percentage of adults with any mental illness reporting an unmet need dropped from 27 percent in 2010–11 to 18 percent in 2014–16. The state also saw significant reductions in the percentage of children with unmet mental health needs.
These improvements did not happen by chance. What actions did policymakers take to drive progress and what work lies ahead?
Making Progress Through Clear Priorities and State Leadership
In 2014, Governor Gina Raimondo came into office fully committed to the Affordable Care Act, including Rhode Island’s state-based health insurance marketplace and expanded Medicaid eligibility.
Another early administration priority was making sure behavioral health care was as available and affordable as medical care. The opioid epidemic was hitting Rhode Island hard, making access to treatment for mental health and substance use disorder a top concern.
Coverage expansion. The decision to create a state-based marketplace, HealthSource Rhode Island (HSRI), was instrumental in helping the state make gains in coverage and affordability. The state has its own funding for marketing and navigators who help people understand and choose health plans. This has helped shield residents from federal outreach cuts. The state’s commitment also helped when the Trump administration decided to end marketplace cost-sharing-reduction subsidies. The state’s Office of the Health Insurance Commissioner (OHIC) worked with the state marketplace HSRI to protect consumers by building price increases to cover the loss of subsidies into silver-level health plans and keeping premiums lower in the other plans. HSRI plans offered among the lowest state-based marketplace premiums in the country. During last year’s open-enrollment period, HSRI saw a 5 percent increase in new and overall customers.
Access to behavioral health. In 2015, Governor Raimondo issued an executive order to establish the Overdose Prevention and Intervention Task Force, which has guided state reforms. The opioid crisis also has led to more open conversations about mental health and to improved relationships between first responders and communities. To facilitate these relationships, Rhode Island now requires police officers receive training to recognize behavioral health issues and help connect individuals with the care they need.
Rhode Island experienced a decline in overall overdose deaths, from 336 in 2016 to 314 in 2018. Community programs and pharmacies have worked hard to get naloxone, used to counter the effects of opioid overdose, into the hands of people who need it. Rhode Island was also the first state to offer medication-assisted opioid treatment in prison. Community health workers follow up on inmates after release to ensure treatment is continued. Fatal overdoses declined by 60 percent among people leaving detention from 2016 to 2017, and continued to drop in 2018.
OHIC also has prioritized integrating behavioral health into the primary care setting as a cost-effective way of increasing access to such services. Studies have shown that integrated care improves depression and anxiety outcomes, along with quality of life, while reducing the total cost of care.
Additionally, OHIC has been working on encouraging parity between medical and behavioral health in the insurance market by reviewing insurers’ coverage documents. It is focusing on limiting mental health benefit exclusions and ensuring the states’ major carriers are in compliance with the laws related to coverage for mental health and substance use disorder treatment. As a result, the four major insurers have agreed to discontinue prior authorization requirements for certain medication-assisted treatments.
Maintaining Momentum
In 2018 an HSRI/OHIC workgroup was formed to develop policy options to mitigate the potential impact of federal changes on health coverage costs, consumer choice, and access. The group recommended pursuing a Section 1332 waiver to establish a reinsurance program to reduce premium increases in the individual market; implementing a state-level requirement that individuals have health insurance to offset the impact of the federal health insurance mandate penalty repeal; and establishing OHIC’s regulatory authority over short-term limited duration plans. All three recommendations were signed into law on July 5.
In addition, recent state legislation has expanded OHIC’s authority related to establishing behavioral health parity, such as a law giving it authority over health plans and third-party organizations that conduct benefit reviews.
Addressing population health challenges demands a concerted effort. Rhode Island is fortunate to have a culture of collaboration among health care leaders, coupled with strong political commitment to health system improvement.
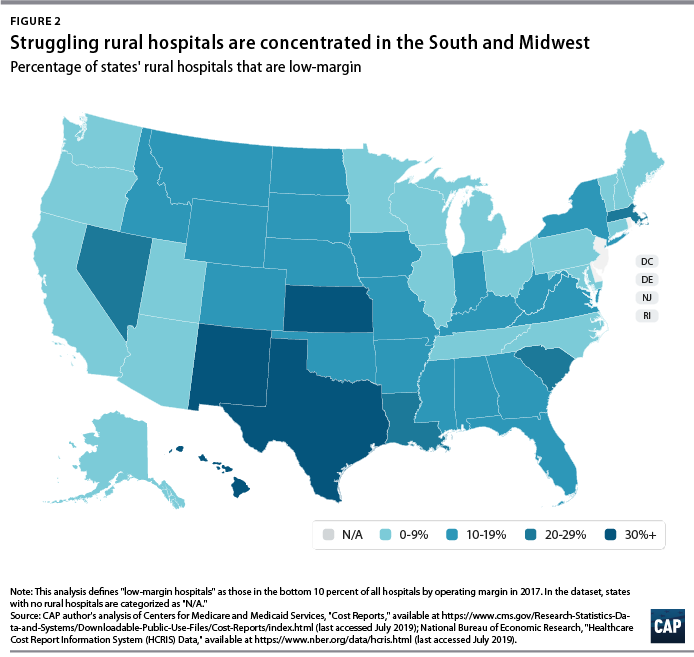
The number of rural hospital closures in the United States has increased over the past decade.1 Since 2010, 113 rural hospitals,2 predominantly in Southern states, have closed. This is a concerning trend, since hospital closures reduce rural communities’ access to inpatient services and emergency care.3 In addition, hospitals that are at risk financially are more likely to serve rural communities with higher proportions of vulnerable populations.4
Understanding the financial pressures facing rural hospitals is imperative to ensuring that America’s 60 million rural residents have access to emergency care.5 Rural hospitals are generally less profitable than urban ones, and those with the lowest operating margins maintain fewer beds and have lower occupancy rates. Low-margin rural hospitals are also more likely to be in states that have not expanded Medicaid under the Affordable Care Act (ACA). According to new analysis by the Center for American Progress, future hospital closures would reduce rural Americans’ proximity to emergency treatment. Among low-margin, rural hospitals—those most likely to close—the majority of those with emergency departments are at least 20 miles away from the next-closest emergency department.
This report first discusses the role that hospitals and emergency care play in rural health care as well as trends in hospital closures. It then uses federal data to examine differences in the financial viability of rural and urban hospitals and the availability of hospital-based emergency care in rural areas. The final section of this report offers policy recommendations to improve health care access and emergency care for rural residents.
Rural hospitals have been closing at an unprecedented rate
From 2013 to 2017, rural hospitals closed at a rate nearly double that of the previous five years.6 (See Figure 1) According to the Government Accountability Office (GAO), recent rural hospital closures have disproportionately occurred among for-profit and Southern hospitals. Southern states accounted for 77 percent of rural hospital closures over that time period but only 38 percent of all rural hospitals in 20137
Hospital closures may deepen existing disparities in access to emergency care. Closures are more likely to affect communities that are rural, low income, and home to more racial/ethnic minority residents.8 Although about half of acute care hospitals are located in rural communities and the other half are located in urban areas,9 rural residents live 10.5 miles from the nearest acute care hospital on average, compared with 4.4 miles for those in urban areas.10 According to a poll by the Pew Research Center, about one-quarter (23 percent) of rural residents said that “access to good doctors and hospitals” is a problem in their community, while only 18 percent of urban residents and 9 percent of suburban residents said it was a problem.11
A variety of factors influence hospitals’ sustainability. Thanks to medical and technological advances, conditions that once required hospitalization can now be treated in an ambulatory care center or a physician’s office. University of Pennsylvania professor and CAP nonresident senior fellow Ezekiel Emanuel has argued that one reason hospitals are closing is that “more complex care can safely and effectively be provided elsewhere, and that’s good news.”12 As a whole, the hospital industry remains highly profitable, and hospital margins are at their highest in decades.13
Evidence on the relationship between hospital closures and health outcomes is mixed. A 2015 study of nearly 200 hospital closures in Health Affairs found no significant changes in hospitalization rates or mortality in the affected communities, whether rural or urban.14 More recent studies have found an association between rural hospital closures and increased mortality. Harvard researcher Caitlin Carroll showed that rural hospital closures led to an overall increase in mortality rates for time-sensitive health conditions,15 and Kritee Gujral and Anirban Basu of the University of Washington found that rural hospital closures in California were followed by increases in mortality for inpatient stays.16
In rural areas, hospitals face additional challenges to their viability, including lower patient volumes; higher rates of uncompensated care; and physician shortages.17 In addition, rural patients tend to be older and lower income.18 Rural hospitals tend to be smaller, serve a higher share of Medicare patients, and have lower occupancy rates than urban hospitals.19 Rural hospitals commonly offer obstetrics, imaging and diagnostic services, emergency departments, as well as hospice and home care,20 but patients needing more complicated treatment are often referred to tertiary or specialized hospitals. In fact, rural patients are more likely to be transferred to another hospital than patients at urban hospitals.21
Most urban hospitals are reimbursed under the prospective payment systems (PPS) for Parts A and B of Medicare. Through both the inpatient and outpatient PPS, the Centers for Medicare and Medicaid Services (CMS) reimburse hospitals at a predetermined amount based on diagnoses, with adjustments—including those for local input costs and patient characteristics.22However, rural hospitals often face higher costs due to lower occupancy rates and provide care to a higher percentage of patients covered by Medicare, Medicaid, and the Children’s Health Insurance Program (CHIP). Such hospitals may be eligible to receive higher payments from Medicare if they qualify as a Sole Community Hospital (SCH) or Medicare-Dependent Hospital (MDH).23
Another form of financial relief for rural hospitals is obtaining designation as a Critical Access Hospital (CAH), which Medicare reimburses based on cost rather than on the PPS.24 To qualify as a CAH, a hospital must provide 24/7 emergency services; maintain no more than 25 beds; and serve a rural area that is 35 miles from another hospital.25 Medicare reimburses CAHs at 101 percent of reasonable costs, rather than through the inpatient and outpatient PPS structures.26 As of 2018, there were 1,380 CAHs nationwide,27 accounting for about two-thirds of all rural hospitals.28
Even with cost-based reimbursement, however, some CAHs are unable to sustain the costs required to maintain inpatient beds.29 The 25-bed limit for CAHs prevent participating hospitals from eliminating inpatient services and restrict their ability to expand in response to fluctuations in community populations or care volumes. Other challenges facing rural hospitals include lacking sufficient patient volume to maintain high-quality performance for certain procedures and pressure to drop high-value but poorly reimbursed services such as obstetrics while maintaining low-volume, high profit services such as joint replacement procedures. 30
A key way that states can support struggling rural hospitals is by expanding Medicaid under the ACA. Expanding Medicaid increases coverage among low-income adults, 31 which in turn reduces uncompensated care costs for hospitals32 and allows financially vulnerable hospitals to improve their viability.33 Consistent with other recent studies,34 the GAO concluded in a 2018 report on rural hospitals that those “located in states that increased Medicaid eligibility and enrollment experienced fewer closures.”35
Rural hospitals are cutting back on services
Rural hospitals in different states have responded to financial pressures in a variety of ways, trying to balance community needs with financial viability. For many hospitals this has meant cutting inpatient obstetric services, leaving more than half of rural counties without hospital obstetric services.36 For instance, in Wisconsin, falling birth rates led to 12 hospitals in the state closing their obstetric services in the past decade.37 In Grantsburg, Wisconsin, lower birth rates and an older community population led Burnett Medical Center to shut down its obstetrics services.38 In order to offer these services, Burnett Medical Center would have needed to keep a general surgeon on call to perform caesarean sections, and with just 40 deliveries in 2017, the hospital could not justify the expense.39 While the hospital will continue providing prenatal and postnatal care, it will refer patients to a facility in Minnesota for deliveries—a facility is almost 40 minutes away.40
In other communities, hospitals have been replaced by other types of health care facilities. For example, Appalachian Regional Healthcare System closed Blowing Rock Hospital in North Carolina in 2013. Three years later, it opened a 112-bed post-acute care center in Blowing Rock in response to demand for rehabilitation services and the aging population in the surrounding area.41
Financial data shows that rural hospitals are more likely to struggle
To compare the financial situations of rural and urban hospitals and examine how future rural hospital closures could affect the availability of emergency care, CAP analyzed data from the CMS Healthcare Cost Report Information System (HCRIS). The CMS requires all Medicare-certified hospitals to report their financial information annually. CAP used the HCRIS to examine the financial margins and other characteristics of 4,147 acute care hospitals for fiscal year 2017. Of these, 1,954 hospitals (47 percent) were in rural areas, while the remaining were in urban areas. Hospitals self-report their status in the HCRIS as either urban or rural, which the CMS defines as either inside or outside of a metropolitan statistical area, respectively.42 Further information about CAP’s hospital sample can be found in the Methodological appendix.
Hospital operating margins, which measure excess patient-related revenues relative to patient-related expenses, are often used as an indicator of financial health.43 A 2011 study by Harvard researchers Dan Ly, Ashish Jha, and Arnold Epstein found that the lowest 10 percent of hospitals by operating margin were 9.5 times more likely to close within two years compared to all others. 44 The same study concluded that hospitals with low operating margins were also more likely to be acquired or merge.45
In CAP’s hospital sample, the median operating margin was negative 2.6 percent among all hospitals, negative 0.1 percent for urban hospitals, and negative 4.9 percent for rural hospitals.46 Public hospitals and MDHs in the sample were more likely to have negative operating margins, consistent with what other studies have found.47 To analyze hospitals’ relative financial health across geographic areas, CAP ranked hospitals in the HCRIS sample based on operating margin, splitting them into three groups: the lowest 10 percent, the middle 80 percent, and the highest 10 percent. The range of operating margins for each group is shown in Table 1.
Rural hospitals are less likely to be financially healthy than urban hospitals. In 2017, rural hospitals comprised only 27.9 percent of the hospitals with operating margins in the highest decile but comprised 59.7 percent of the hospitals in the lowest decile. Southern and Midwestern states had the greatest proportion of rural hospitals with low operating margins, mimicking the geographic patterns in hospital closures that the GAO report identified. CAP finds that from 2015 through 2017, rural hospitals were consistently more likely than urban hospitals to fall in the bottom 10 percent of operating margins. CAP’s analysis also confirms that rural hospitals in states that expanded Medicaid had a higher median operating margin (negative 3.4 percent) than those in states that have not expanded Medicaid (negative 5.7 percent).
To examine commonalities among the hospitals most vulnerable to closure, CAP analyzed characteristics of the hospitals with low margins, defined as having an operating margin in the lowest 10 percent among all hospitals. Smaller, low-occupancy rural hospitals were most likely to struggle financially: nearly 1 in 6 (15 percent) of hospitals with 25 or fewer beds had low margins, and nearly one-fifth (17 percent) of hospitals with low-occupancy rates had low margins. (See Figure 3)
Emergency departments are on the front lines for rural health
In some emergency situations, hospital closures can be life-threatening, increasing the time and distance patients travel to receive care. Studies show that the probability of dying from a heart attack increases with distance from emergency care,48 and traumatic injuries are more likely to be fatal for rural residents than for urban ones.49
Rural residents are more likely than urban residents to visit the emergency department.50 A shortage of primary care providers; lack of public transportation infrastructure; shortages in preventive care; higher rates of smoking and obesity; and greater prevalence of chronic disease in rural areas all contribute to the greater utilization of emergency room care.51 As a result, emergency departments often stand in as the main source of care for vulnerable and low-income populations, especially for communities that face a shortage of primary care. 52 Among the dozens of rural hospitals that have closed in recent years, some served as the only emergency department in a community, according to MedPAC53
While freestanding emergency departments have proliferated,54 they are not filling the gap for rural emergency care. MedPAC found that, as of 2016, nearly all the country’s 566 stand-alone emergency departments were in urban areas and tended to be located in more affluent communities.55 Researchers at the North Carolina Rural Health Research Program found that the freestanding emergency department model was generally not viable in rural areas of the state due to low patient volumes, high rates of uninsured patients, and provider shortages.56 One limit on the growth of independent freestanding emergency centers is that they are not recognized in Medicare law and are therefore unable to bill the program, unlike hospital-affiliated off-campus emergency departments. 57
Future rural hospital closures would increase the distances that patients travel for emergencies
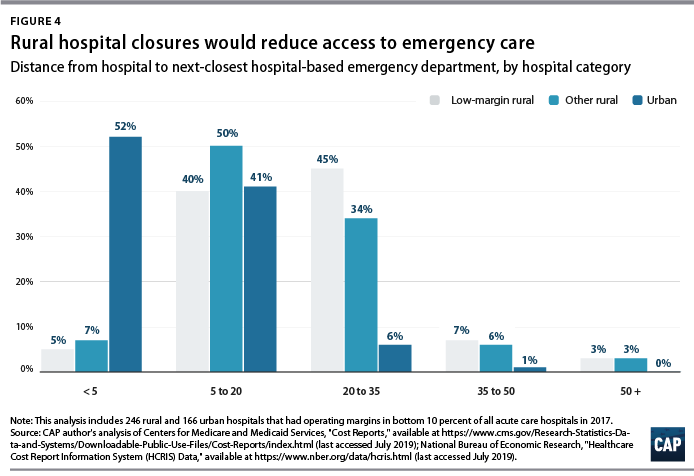
To better understand how future rural hospital closures could affect access to emergency care, CAP calculated hospitals’ distance to the next-closest hospital-based emergency department. CAP restricted its 2017 HCRIS data sample to the 3,616 acute care hospitals that provide 24-hour emergency services.58 Using addresses or coordinates provided in the HCRIS, CAP mapped each low-margin rural hospital to the next-closest hospital emergency department. Mapping strategies are detailed in the Methodological appendix.
Among the 222 low-margin rural hospitals, more than half (55 percent) were more than 20 miles away from the next-closest hospital-based emergency department, and one-tenth were more than 35 miles away. (See Figure 4). The average distance to the next-closest emergency department was 22 miles.
The disappearance of rural, low-margin hospitals would greatly increase patients’ travel distances for emergency care. Without other resources to fill the gap, some patients might forgo care they need and others would be forced to undertake an even longer journey to receive medical attention.
Policies to improve rural emergency and nonemergency care
As rural hospitals continue to close, it is crucial to preserve access to emergency care for rural Americans. The following section details a series of policy recommendations to support adequate emergency care and address care shortages in rural communities.
Expand Medicaid
Experience to date suggests that rural hospitals in those states that have not yet expanded their Medicaid programs under the ACA would benefit from Medicaid expansion through lower levels of uncompensated care and increased financial sustainability. Medicaid expansion is associated with improvements in health and a wide variety of other outcomes, including lower mortality, less uncompensated care, and lower rates of medical debt.59 According to the Kaiser Family Foundation, about 4.4 million adults would gain Medicaid eligibility if the remaining 14 nonexpansion states expanded their programs.60
Policymakers can also support rural communities and their hospitals by opposing efforts to repeal the ACA. If the Trump administration-backed lawsuit against the ACA were to succeed, 20 million Americans would lose health insurance coverage, and uncompensated care would rise by $50 billion, according to the Urban Institute.61
Create a greater number of rural emergency centers
To preserve access to emergency care, Congress could allow rural hospitals like CAHs to downsize to an emergency department and eliminate inpatient beds without giving up special Medicare reimbursement arrangements. Qualifying hospitals could transfer patients requiring inpatient admission to other hospitals, while continuing to offer some diagnostic imaging and other outpatient services.
One such proposal is the Rural Emergency Acute Care Hospital Act (REACH Act), bipartisan legislation proposed by Sen. Amy Klobuchar (D-MN) and Sen. Chuck Grassley (R-IA) that would create rural emergency centers.62 This designation would allow hospitals to provide only emergency care in rural communities and receive Medicare reimbursement at 110 percent of operating costs. Separately, MedPAC has recommended that rural hospitals located more than 35 miles from the nearest emergency department be allowed to convert to freestanding emergency departments while still being reimbursed at hospital rates.63
Institute global budgeting for rural hospitals
Under global budgeting, hospitals are paid a fixed amount rather than having their reimbursements based on the volume and types of services they provide.64 Global budgeting can reduce small, rural hospitals’ financial risk by providing them with a more predictable stream of revenue. In addition, payment reforms that include both hospital and nonhospital care can encourage communities to invest in services that are typically less generously reimbursed, such as preventive care.65
For example, in 2014, Maryland transitioned its acute hospitals from fee-for-service payments to a global budget.66 An evaluation of the global budget program showed that it reduced hospital expenditures relative to trend without transferring costs to other parts of the health care system.67 Future global budgets should emphasize improvements in population health and primary care,68 including ensuring that patients receive care in appropriate settings and reducing the number of avoidable hospital visits.
The Pennsylvania Rural Health Model is the first Medicare demonstration project to test the financial viability and community effects of a global budget for strictly rural hospitals.69 This six-year program aims to smooth out cash flow for 30 rural Pennsylvania hospitals on a monthly basis with the goal of enabling hospitals to meet community needs, especially for substance-use disorder and mental health services.70 With global budgets based on the previous year’s revenues, participating hospitals will have a more predicable stream of revenue. Importantly, the program allows hospitals to share in the savings that result from avoidable utilization.71
Improve transportation for rural residents
The lack of transportation infrastructure can lead rural residents to rely on ambulances and emergency rooms for nonemergency care. In nonemergency situations, patients often cite the lack of affordable transportation as a major barrier to care access.72 In order to fill the gap, payers and policymakers should consider efforts to utilize existing community transit resources for medical transportation or reimburse patients who use ride-sharing services in areas that lack public transit or taxi services. 73 Another option would be to formalize volunteer services for medical transit. Oregon offers a tax credit for volunteer rural emergency medical services (EMS) providers, who provide medical and transportation services analogous to those of volunteer firefighter programs.74 The CMS should also consider policies to better reimburse and expand the use of telehealth in remote areas to reduce patients’ burden of transportation.75Finally, the CMS should stop approving states’ requests to waive coverage of nonemergency medical transportation (NEMT) requirements under Medicaid.76 NEMT is vital to eligible beneficiaries’ access to care, including appointments for preventive care, chronic disease management, and substance-use disorder treatment.
Strengthen the rural health care workforce
Rural health care provider shortages contribute to poorer access to care and poorer quality of care in rural communities. While 20 percent of the U.S. population lives in rural areas, only 9 percent of primary care physicians practice in rural areas.77 Greater access to primary care providers in rural areas would improve quality of care and health outcomes while also reducing unnecessary emergency department visits.78
One way to assist rural areas would be to encourage health professionals to train and work in underserved communities. Federal funding for physician training should include reimbursements for community-based sites so that medical residents can rotate through nonhospital settings.79 Expanding the National Health Service Corps—which provides scholarships and student loan repayment for professionals who work in federally designated health professional shortage areas—could also help bolster the rural workforce. In addition, changes to immigration policy—such as expanding the Conrad 30 program that funnels immigrant doctors into rural and underserved communities, reforming H-1B visas to benefit high-need communities—could help alleviate rural areas’ shortage of medical professionals.80
Conclusion
Mounting closures of rural hospitals across the country are exacerbating the disparity in health care access between rural and urban areas. The financial vulnerability of the remaining rural hospitals suggests that the trend may continue, leaving shortages in emergency care and other hospital services.
Policymakers should support initiatives that allow remaining rural hospitals the flexibility to tailor their services to meet community needs and improve access to care for rural Americans.
Norfolk, Va.-based Sentara Healthcare improved its operating revenues and net income in the first half of fiscal year 2019, according to unaudited financial documents.
Sentara recorded total operating revenues of $3.3 billion in the six-month period ended June 30, up 6.7 percent from $3.1 billion reported in the same period a year prior. The health system said the increase was primarily driven by growth in net patient service revenue. Sentara’s expenses also increased year over year by 9.3 percent to $3.1 billion for the most recent six-month period.
Sentara’s health plan saw a $34.8 million decrease in premium and capitation revenue in the most recent six-month period, driven by a 46,000-member reduction in health maintenance organization individual enrollment. However, the decline was mostly offset by an increase in Medicaid and other membership of 48,000, thanks to the state’s recent Medicaid expansion.
Overall, Sentara saw its net operating income decline 19 percent year over year to $230.5 million, down from $284.8 million reported in the same period of fiscal 2018. After including nonoperating gains, Sentara ended the first half of the fiscal year with net income of $569.4 million, up 81.2 percent from $314.1 million recorded in the same period of the previous year.
Hospitals that care for a large share of Medicaid, low-income and uninsured patients stand to receive less funding from the federal government after the D.C. Circuit reconsidered how Medicaid disproportionate-share hospital reimbursement is calculated.
A three-judge panel of the U.S. Court of Appeals for the District of Columbia Circuit reversed a lower court and reinstated a 2017 rule establishing that payments by Medicare and private insurers are to be included in calculating a hospital’s DSH limit, ultimately lowering its maximum reimbursement.
In Tuesday’s ruling, U.S. Circuit Judge Karen LeCraft Henderson opined that the rule aligns with the intent of the Medicaid Act.
“By requiring the inclusion of payments by Medicare and private insurers, the 2017 rule ensures that DSH payments will go to hospitals that have been compensated least and are thus most in need,” Henderson wrote.
The case, brought by four children’s hospitals in Minnesota, Virginia and Washington and an association representing eight children’s hospitals in Texas, concerns the calculation of the uncompensated costs of treating Medicaid beneficiaries known as the “Medicaid shortfall.”
For instance, if a hospital spends $1 million on treating Medicaid patients who have no other healthcare coverage and Medicaid pays $600,000, then the Medicaid shortfall is $400,000. In some instances, Medicaid patients have additional third-party coverage such as Medicare or private insurance.
Hospitals cannot receive more money in Medicaid DSH payments than they spent to treat Medicaid beneficiaries or the uninsured. Part of the motivation behind that stipulation was to prevent hospitals from double dipping by collecting DSH payments to cover costs that had already been reimbursed. Previous cases also revealed that some states have made DSH payments to state psychiatric or university hospitals that exceed the net costs, or even total costs, of operating the facilities.
Providers successfully fought the 2017 rule that limited hospitals’ reimbursement. A federal judge sided with the hospitals that claimed the CMS overstepped its authority and essentially ignored payments by commercial insurers and Medicare. That was overturned Tuesday.
The Children’s Hospital Association of Texas said in a statement that it is exploring its options.
“We are disappointed with the result because it will reduce critical Medicaid funding to safety net providers like children’s hospitals,” the association said. “These hospitals are heavily reliant on Medicaid payments because between 50% and 80% of their inpatient days are covered by Medicaid. Children’s hospitals care for all children, and are, in fact, often the only place that children with complex conditions can get life-saving care.”