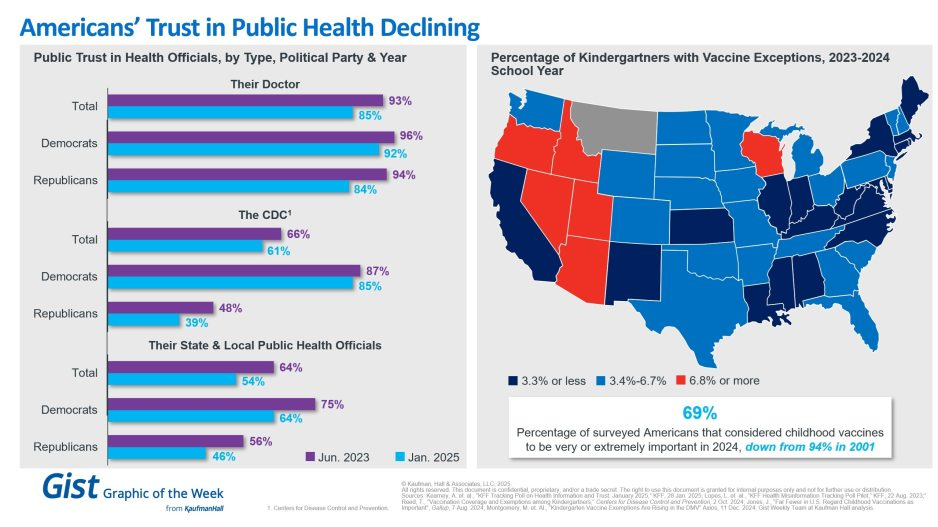
In light of the recent confirmation of Secretary Kennedy to lead HHS and new survey data on trust in public health, this graphic highlights Americans’ declining positive perception of public health officials. Among respondents’ personal doctors, the CDC and their state and local public health officials, trust in all three, regardless of political identification, has decreased from June 2023 to January 2025.
Respondents trusted their doctors more than public health officials, and there is less difference by political identification. In 2025, only 61% of surveyed Americans reported that they trusted the CDC. That prevalence drops to 39% among Republicans and increases to 85% among Democrats.
Another important public health indicator, the percentage of kindergarteners with vaccine exemptions, also illustrates the challenging place in which public health officials find themselves. During the 2023-2024 school year, about 3.3% of kindergartners received an exemption, an increase from 2022-2023 that still does not provide a complete picture. Exemption rates vary widely by state, with 6 states having exemption rates more than double the median. These differences are a reflection of how easy it is to receive an exemption in some states rather than a clear trend.
The shift also underscores how easily an outbreak could occur in some states. Alarmingly, the perceived importance of vaccines has dramatically decreased, from 94% in 2001 to 69% in 2024.
We will have to wait and see what Kennedy, long considered a vaccine skeptic, does regarding vaccines, but amid immense distrust in the healthcare system, providers’ role of giving thorough, honest information to their patients is more important than ever.
In May 2024 a set of articles were published in the journal Science that focused on the intersection of misinformation and social media. The results, while preliminary in the grand scheme of things, were really interesting (and maybe a little alarming).
In the last 2 weeks, the Affordable Care Act (ACA) has been inserted itself in Campaign 2024 by Republican aspirants for the White House:
On Truth Social November 28, former President Trump promised to replace it with something better:“Getting much better Healthcare than Obamacare for the American people will be a priority of the Trump Administration. It is not a matter of cost; it is a matter of HEALTH. America will have one of the best Healthcare Plans anywhere in the world. Right now, it has one of the WORST! I don’t want to terminate Obamacare, I want to REPLACE IT with MUCH BETTER HEALTHCARE. Obamacare Sucks!!!!”
Then, on NBC’s Meet the Press December 3, Florida Governor Ron DeSantis offered “We need to have a healthcare plan that works,” Obamacare hasn’t worked. We are going to replace and supersede with a better plan….a totally different healthcare plan… big institutions that are causing prices to be high: big pharma, big insurance and big government.”
It’s no surprise. Health costs and affordability rank behind the economy as top issues for Republican voters per the latest Kaiser Tracking Poll. And distaste with the status quo is widespread and bipartisan: per the Keckley Poll (October 2023), 70% of Americans including majorities in both parties and age-cohorts under 65 think “the system is fundamentally flawed and needs major change.” To GOP voters, the ACA is to blame.
Background:
The Affordable Care Act (aka Obamacare aka the Patient Protection and Affordable Care Act) was passed into law March 23, 2013. It is the most sweeping and controversial health industry legislation passed by Congress since Lyndon Johnson’s Medicare and Medicaid Act (1965). Opinions about the law haven’t changed much in almost 14 years: when passed in 2010, 46% were favorable toward the law vs. 40% who were opposed. Today, those favorable has increased to 59% while opposition has stayed at 40% (Kaiser Tracking Poll).
Few elected officials and even fewer voters have actually read the law. It’s understandable: 955 pages, 10 major sections (Titles) and a plethora of administrative actions, executive orders, amendments and legal challenges that have followed. It continues to be under-reported in media and misrepresented in campaign rhetoric by both sides. Campaign 2024 seems likely to be more of the same.
In 2009, I facilitated discussions about health reform between the White House Office of Health Reform and the leading private sector players in the system (the American Medical Association, the American Hospital Association, America’s Health Insurance Plans, AdvaMed, PhRMA, and BIO). The impetus for these deliberations was the Obama administration’s directive that systemic reform was necessary with three-aims: reduce cost, increase access via insurance coverage and improve the quality of care provided by a private system. In parallel, key Committees in the House and Senate held hearings ultimately resulting in passage of separate House and Senate versions with the Senate’s becoming the substance of the final legislation. Think tanks on the left (I.e. the Center for American Progress et al.) and on the right (i.e. the Heritage Foundation) weighed in with members of Congress and DC influencers as the legislation morphed. And new ‘coalitions, centers and institutes’ formed to advocate for and against certain ACA provisions on behalf of their members while maintaining a degree of anonymity.
So, as the ACA resurfaces in political discourse in coming months, it’s important it be framed objectively. To that end, 3 major considerations are necessary to have a ‘fair and balanced’ view of the ACA:
1-The ACA was intended as a comprehensive health reform legislative platform. It was designed to be implemented between 2010 and 2019 in a private system prompted by new federal and state policies to address cost, access and quality. It allowed states latitude in implementing certain elements (like Medicaid expansion, healthcare marketplaces) but few exceptions in other areas (i.e.individual and employer mandates to purchase insurance, minimum requirements for qualified health plans, et al). The CBO estimated it would add $1.1 trillion to overall healthcare spending over the decade but pay for itself by reducing demand, administrative red-tape and leveraging better data for decision-making. The law included provisions to…
To improve quality by modernizing of the workforce, creating an Annual Quality Report obligation by HHS, creating the Patient Centered Outcome Research Institute and expanding the the National Quality Forum, adding requirements that approved preventive care be accessible at no cost, expanding community health centers, increasing residency programs in primary care and general surgery, implementing comparative effectiveness assessments to enable clinical transparency and more.
To increase access to health insurance by subsidizing coverage for small businesses and low income individuals (up to 400% of the Federal poverty level), funding 90% of the added costs in states choosing to expand their Medicaid enrollments for households earning up to 138% of the poverty level, extending household coverage so ‘young invincibles’ under 26 years of age could stay on their parent’s insurance plan, requiring insurers to provide “essential benefits” in their offerings, imposing medical loss ratio (MLR) mandates (80% individual, 85% group) and more.
To lower costs by creating the CMS Center for Medicare and Medicaid Innovation to construct 5-year demonstration pilots and value-based purchasing programs that shift provider incentives from volume to value, imposing price and quality reporting and transparency requirements and more.
The ACA was ambitious: it was modeled after Romneycare in MA and premised on the presumption that meaningful results could be achieved in a decade. But Romneycare (2006) was about near-universal insurance coverage for all in the Commonwealth, not the triple aim, and the resistance calcified quickly among special interests threatened by its potential.
2-The ACA passed at a time of economic insecurity and hyper-partisan rancor and before many of the industry’s most significant innovations had taken hold. The ACA was the second major legislation passed in the first term of the Obama administration (2009-2012); the first was the $831 billion American Recovery and Reconstruction Act (ARRA) stimulus package that targeted “shovel ready jobs” as a means of economic recovery from the 2008-2010 Great Recession. But notably, it included $138 billion for healthcare including requirements for hospitals and physicians to computerize their medical records, extension of medical insurance to laid off workers and additional funding for states to offset their Medicaid program expenses. The Obama-Biden team came to power with populist momentum behind their promises to lower health costs while keeping the doctors and insurance plans they had. Its rollout was plagued by miscues and the administration’s most popular assurances (‘keep your doctor and hospitals’) were not kept. The Republican Majority in the 111th Congress’ (247-193)) seized on the administration’s miss fueling anti-ACA rhetoric among critics and misinformation.
3-Support for the ACA has grown but its results are mixed. It has survived 7 Supreme Court challenges and more than 70 failed repeal votes in Congress. It enjoys vigorous support in the Biden administration and among the industry’s major trade groups but remains problematic to outsiders who believe it harmful to their interests. For example, under the framework of the ACA, the administration is pushing for larger provider networks in the 18 states and DC that run their own marketplaces, expanded dental and mental health coverage, extended open enrollment for Marketplace coverage and restoration of restrictions on “junk insurance’ but its results to date are mixed: access to insurance coverage has increased. Improvements in quality have been significant as a result of innovations in care coordination and technology-enabled diagnostic accuracy. But costs have soared: between 2010 and 2021, total health spending increased 64% while the U.S. population increased only 7%.
So, as the ACA takes center stage in Campaign 2024, here are 4 things to watch:
1-Media attention to elements of the ACA other than health insurance coverage. My bet: attention from critics will be its unanticipated costs in addition to its federal abortion protections now in the hands of states. The ACA’s embrace of price and quality transparency is of particular interest to media and speculation that industry consolidation was an unintended negative result of the law will energize calls for its replacement. Thus, the law will get more attention. Misinformation and disinformation by special interests about its original intent as a “government takeover of the health system” will be low hanging fruit for antagonists.
2- Changes to the law necessary intended to correct/mitigate its unintended consequences, modernize it to industry best practice standards and responses to court challenges will lend to the law’s complex compliance challenges for each player in the system. New ways of prompting Medicaid expansion, integration of mental health and social determinants with traditional care, the impact of tools like ChatGPT, quantum computing, generative AI not imagined as the law was built, the consequences of private equity investments on prices and spending, and much more.
3-Public confusion. The ACA is a massive law in a massive industry. Cliff’s Notes are accessible but opinions about it are rarely based on a studied view of its intent and structure. It lends itself to soundbites intended to obscure, generalize or misdirect the public’s attention.
4-The ACA price tag. In 2010, the CBO estimated its added cost to health spending at $1.1 trillion (2010-2019) but its latest estimate is at least $3 trillion for its added insurance subsidies alone. The fact is no one knows for sure what its costs are nor the value of the changes it has induced into the health system. The ranks of those with insurance coverage has been cut in half. Hospitals, physicians, post-acute providers, drug manufacturers and insurers are implementing value-based care strategies and price transparency (though reluctantly) but annual health cost increases have consistently exceeded 4% annually as the cumulative impact of medical inflation, utilization, consolidation and price increases are felt.
Final thought:
I have studied the ACA, and the enabling laws, executive orders, administrative and regulatory actions, court rulings and state referenda that have followed its passage. Despite promises to ‘repeal and replace’ by some, it is more likely foundational to bipartisan “fix and repair’ regulatory reforms that focus more attention to systemness, technology-enabled self-care, health and wellbeing and more.
It will be interesting to see how the ACA plays in Campaign 2024 and how moderators for the CNN-hosted debates January 10 in Des Moines and January 21 in New Hampshire address it. In the 2-hour Tuscaloosa debate last Wednesday, it was referenced in response to a question directed to Gov. DeSantis about ‘reforming the system’ 101 minutes into the News Nation broadcast. It’s certain to get more attention going forward and it’s certain to play a more prominent role in the future of the system.
The ACA is back on the radar in U.S. healthcare. Stay tuned.
PS The resignations under pressure of Penn President Elizabeth Magill and Board Chair Scott Bok over inappropriate characterization of Hamas’ genocidal actions toward Jews are not surprising. Her response to Congressional questioning was unfortunate. The eventuality turned in 4 days, sparked by student outrage and adverse media attention that tarnished the reputations of otherwise venerable institutions like Penn, MIT and Harvard.
The lessons for every organization, including the big names in healthcare, are not to be dismissed: Beyond the issues of genocide, our industry is home to a widening number of incendiary issues like Hamas.
They’re increasingly exposed to public smell tests that often lead to more: Workforce strikes. CEO compensation. Fraud and abuse. Tax exemptions and community benefits. Prior authorization and coverage denial. Corporate profit. Patient collection and benevolent use policies. Board independence and competence and many more are ripe for detractors and activist seeking attention.
Public opinion matters. Reputations matter. Boards of Directors are directly accountable for both.
Misinformation. A recent and major problem facing us all, and one that is pervasive in many realms including medicine and healthcare, which are, of course, favorite realms around here. But is all this stuff recent? Is misinformation a new phenomenon in the world of medicine and health, or does it have a history?
The answer to that, thanks in part to funding from the National Institute for Healthcare Management, is the topic of this week’s Healthcare Triage.
With Medicare’s Annual Election Period (also known as Open Enrollment) beginning on October 15th, over 65 million adults across the United States will have until December 7th to decide whether they plan to renew or change their Medicare coverage. Beneficiaries choose between Traditional Medicare (TM) and a variety of Medicare Advantage (MA) plans and prescription drug coverage.
For this enrollment cycle, it is estimated that the average beneficiary will have over 40 plans to choose from, leading to complexity. For those who are dually eligible for both Medicare and Medicaid benefits, there is an even greater number of options for them to consider, especially if they live in areas where integrated options such as dual-eligible special needs plans and Medicare-Medicaid plans are available.
As the US population continues to age and the number of Medicare enrollees grow, it is important to understand how beneficiaries make their coverage decisions and ensure they are protected from any misinformation in the process.
Though already complex, the plan selection process for older adults is further complicated by the deceptive marketing tactics that brokers, agents, and third-party marketing organizations (TPMOs) have employed in recent years. In a recent study, the Commonwealth Fund identified how some of these practices are driven by the financial incentives associated with enrolling beneficiaries in particular MA plans.
Between robocalls and misleading television advertisements, many beneficiaries across the country have found themselves enrolled in MA plans they did not intend to enroll in, or that did not cover services or in-network providers that they were initially marketed. In a sweeping review of Medicare Open Enrollment-related television ads, Kaiser Family Foundation found that the majority of Open Enrollment-related advertisements last year promoted the Medicare logo and privately-operated hotlines, misleading beneficiaries into believing these were government sponsored ads and helplines.
Acknowledging the growing concerns and complaints among beneficiaries, the Centers for Medicare and Medicaid Services (CMS) announced that starting in 2024, Medicare-related television ads must be approved in advance of airing and cannot contain plan names or Medicare logos and images that misrepresent their organization or agency. Additional consumer protections included in the 2024 MA and Part D Final Rule will hold brokers, agents, and other TPMOs to higher standards of providing transparent, quality information. These activities include monitoring TPMO behavior, regulating how and when they market to beneficiaries, ensuring brokers review the full list of options and choices available to a beneficiary, and going through a detailed, standardized set of pre-enrollment questions. There is also an increased effort in getting beneficiaries to use some of the federally funded tools and resources available to assist in their coverage decisions.
Some of these tools include the Medicare.gov website, the CMS Medicare Plan Compare tool, and a 1-800-MEDICARE hotline to help inform beneficiaries about their benefits. However, a study by Hernandez et al. revealed that very few Medicare beneficiaries utilized these tools and often felt more comfortable discussing their options in-person with brokers or family members and friends, even though these sources may be biased or potentially inaccurate. Additionally, it is important to recognize that navigating these tools requires some degree of health literacy and technological proficiency, which may disproportionately affect those who are low-income, have lower levels of education, or are non-native English speakers.
The State Health Insurance Assistance Program (SHIP), however, is a free and unbiased resource for Medicare counseling that few beneficiaries are aware of. In 1990, the federal government implemented SHIPs to help support Medicare beneficiaries with free, one-to-one health insurance counseling and education within their communities. It is currently run by the Administration for Community Living (ACL). The ACL administers grants to states, who in turn provide funding to community-level subgrantees to maintain various networks of full-time, part-time, and/or volunteer counselors. The latest available data suggests that SHIPs provided assistance to 2.7 million Medicare beneficiaries from April 2018 through March 2019—just 4.5% of the eligible Medicare population.
While some states had greater success, serving over 10% of their eligible population, others were only able to reach as few as 2%. A 2018 evaluation of California’s SHIP, called HICAP (Health Insurance Counseling & Advocacy Program), highlighted the strengths of this community-based counseling system. HICAP reported high rates of engagement, citing their ability to deliver uniquely tailored counseling to beneficiaries in their native languages and through in-person or hybrid settings depending on the beneficiary’s condition or preferences. Moreover, strong marketing efforts via Spanish radio shows and mailing postcards were particularly effective in reaching “hard-to-locate” populations. However, the program did experience challenges given the variation in operations across locations, citing concerns over the recruitment, training and retention of volunteers and paid staff.
In recognition of SHIP’s potential to provide an unbiased alternative to brokers and combat misinformation, CMS finalized a requirement in the 2024 MA and Part D rule that TPMOs are to provide a disclaimer citing SHIP as an option for beneficiaries to obtain additional help (42 CFR § 422.2267(e )(41)). But despite SHIP’s promise, some beneficiary advocates have worried that the multi-tiered, volunteer, and part-time driven delivery model that characterizes most SHIPs leads to access and quality gaps. This is especially a concern among vulnerable beneficiaries who may live in low-income neighborhoods, have disabilities, or limited English proficiency. Given their historically low utilization rates and limited visibility, others have expressed concern that SHIPs may be ill-equipped to handle an increased demand for services in the coming year, due to more Medicare beneficiaries being advised of their existence through TPMO disclaimers. With the limited evidence about SHIP’s performance and outreach nationally, given the diffuse nature of the program, it will be important to understand some of the barriers and facilitators they face to delivering timely and accurate Medicare counseling.
The free and unbiased nature of the SHIP program presents a promising alternative to helping beneficiaries navigate complex plan choices for Open Enrollment. As MA enrollment increases and as plan choices become more complex, the SHIP program should be monitored for potential inequities in access to and quality of services based on area income.
For more information about your state’s SHIP program and to find a local Medicare counselor, please visit https://www.shiphelp.org/.
Amid a flurry of policy changes initiated by Elon Musk since his takeover of the social media company last month, Twitter has ceased its formal efforts to combat COVID misinformation. To date, Twitter had removed over 100K posts for violating its COVID policy. The company will now rely on its users to combat disinformation through its “Birdwatch” program, which lets users rate the accuracy of tweets and submit corrections. Many of the 11K accounts suspended for spreading COVID misinformation, including those of politicians like Rep. Marjorie Taylor Greene (R-GA), have also been reinstated.
The Gist: We’ve seen the damage caused by inaccurate or deliberately misleading COVID information, which has likely played a role in the US’s lower vaccination rates compared to other high-income countries. Around one in five Americans use Twitter, far fewer than Facebook or YouTube, but the platform is seen as highly influential, both for the reach of its content and also its moderation decisions.
This policy change is worrisome, not only because COVID is still taking the lives of hundreds of Americans daily, but also because COVID misinformation catalyzes broader healthcare misinformation, including antivax sentiments and an overall mistrust of medical experts.
The website for the group Physicians for Informed Consent (PIC) reads like an apolitical, educational resource that provides information on vaccines and why they shouldn’t be government-mandated. Its mission is “that doctors and the public are able to evaluate the data on infectious diseases and vaccines objectively, and voluntarily engage in informed decision-making about vaccination.”
The group’s accompanying social media accounts, however, tell a different story. On PIC’s Facebook, Twitter, Instagram, and LinkedIn feeds, you’ll find post after post about reasons to be scared of vaccines – especially for children – often highlighting selective portions of scientific research that contain vaccination risks.
Who’s Behind PIC?
The group was founded in 2015 after California passed a law that prohibited the use of personal belief exemptions from vaccinations required for children to attend any public or private school in the state.
Three years later, the number of waivers issued by doctors to parents seeking medical exemptions for their children tripled. As a result, another law was passed in 2019, cracking down on the inappropriate use of medical exemptions.
The group’s founder, Shira Miller, MD, is a concierge integrative medicine doctor based in Los Angeles, specializing in menopausal care. On her own Twitter profile, she describes herself as “Facebook’s Most Popular Menopause Doctor.”
Miller earned her medical degree in 2002 from Technion-Israel Institute of Technology in Haifa, Israel, and has reportedly been working as a concierge physician since 2010.
PIC’s leadership team also includes 20 physicians from a wide range of specialties, most of whom, like Miller, don’t specialize in infectious diseases.
Among its leaders is Paul Thomas, MD, an Oregon-based pediatrician. Thomas, who is listed as one of PIC’s founding directors, was issued an emergency suspension order of his medical license in 2021 by the state medical board, in which they cited at least eight cases of alleged patient harm. In line with PIC’s philosophy, Thomas maintains that he isn’t “anti-vax” – he’s pro-informed-consent.
Also on the team is Jane Orient, MD, internist and executive director of the Association of American Physicians and Surgeons (AAPS), a group that also opposes vaccine mandates. Orient received her medical degree from Columbia University and currently practices in Arizona. In 2020, the AAPS sued the federal government for withholding its stockpile of hydroxychloroquine from COVID patients, despite research showing that the drug is ineffective. The complaint was dismissed in September 2021.
Doug Mackenzie, MD, a plastic surgeon who graduated from Johns Hopkins University of Medicine, is PIC’s treasurer. He has previously identified himself as an “ex-vaxxer” rather than an anti-vaxxer when speaking on a panel in 2019.
The only RN on the team is Tawny Buettner. After California mandated vaccinations for healthcare workers, Buettner organized a protest outside of her place of work, Rady Children’s Hospital in San Diego; she later sued the hospital after she was dismissed from her job. According to the complaint, Buettner and the 36 other plaintiffs alleged that their requests for religious exemptions from the COVID-19 vaccine were all denied.
Kenneth Stoller, MD, also listed on the leadership team, graduated from the American University of the Caribbean School of Medicine and completed pediatric residency training at the University of California Los Angeles. Stoller was disciplined in 2019 for doling out medical exemptions to children without adequate evidence. According to state records, his license in California has since been revoked; he currently holds a medical license in New Mexico.
What’s PIC?
The most notable physician groups accused of spreading COVID-19 misinformation since the vaccine rollout have been affiliated with right-wing media, if not overtly proclaiming conservative, anti-vaccination beliefs.
For example,America’s Frontline Doctors, a group notorious for its support of hydroxychloroquine as a treatment for COVID-19, has made its values well-known. The group’s founder, Simone Gold, MD, JD, was arrested for participating in the Jan. 6 capitol riot and has openly opposed mask-wearing. Similarly, physician leaders of theFront Line COVID-19 Critical Care Alliance, known for promoting the use of ivermectin to treat COVID-19, tout their appearances on the ultra-conservative Newsmax on the website’s homepage.
PIC wants to be different. The group’s focus, according to its general counsel Greg Glaser, JD, of Copperopolis, California, is on the “authoritative citations that show, or calculate, the risks [of vaccines] to the public,” he told MedPage Today.
“We are pro-informed consent, pro-ethics, pro-health. PIC is not anti-vaccine, and PIC is not pro-vaccine – PIC is neutral,” Glaser said on behalf of the group.
In August 2021, Glaser submitted an amicus brief to the Supreme Court PIC’s behalf, arguing against the implementation of vaccine mandates. The document claims that “government statements confirm there is no evidence that COVID-19 vaccines prevent the spread of SARS-CoV-2 or COVID-19,” ignoring the breadth of existing literature that says otherwise.
The U.S. may have entered into a new phase of the COVID-19 pandemic, but the public health crisis is far from over. The nation’s hospitals and health systems will likely be dealing with its after effects for decades, according to new findings from Fitch Ratings.
Specifically, health implications related to the coronavirus will drive elevated health system utilization long after the acute phase of the pandemic has ended, likely leading to increasing costs and higher insurance premiums for years to come.
These costs will emerge from the necessary addition to outpatient capacity to deal with the ongoing treatment of chronic conditions related to what may be permanent damage caused by the virus.
WHAT’S THE IMPACT?
It’s nigh impossible to determine the magnitude of these effects, said Fitch. It will be dependent on tangential health issues related to deferred diagnostic testing and treatment during the pandemic. Since related conditions are likely to develop over time, Fitch doesn’t anticipate these issues to directly affect the credit profile of issuers in the U.S. healthcare system.
In the near term, health insurers have been able to incorporate expanding COVID-19 claims data, estimates of infection trends and pent-up demand for previously deferred care into 2021 premium rates, which should benefit cost management and pricing this year and next.
However, for healthcare providers, the expansion of the healthcare system over the long term will likely exacerbate traditional pressures on operating performance, such as tight labor and wage markets for experienced staff, rising pharmaceutical expenses and supply costs in general.
Although the U.S. has glimpsed signs of the pandemic’s potential end over the past couple of months, the ultimate story of the pandemic is still being told.
The infection rate is once again trending up, presumably due to a combination of factors, including a dramatic reduction in demand for new vaccinations, the rapid spread of the more infectious Delta variant and the reduction in mitigation measures.
THE LARGER TREND
The rising numbers of COVID-19 infections in the U.S. are occurring mostly in communities with low rates of vaccinations, with Centers for Disease Control and Prevention Director Dr. Rochelle Walensky saying in July that “This is becoming a pandemic of the unvaccinated.”
Data published by USA Today shows that cases are rising in all 50 states, with some startling increases in certain areas. Rhode Island, for example, saw cases almost triple in a one-week period, with Maine and Vermont following closely behind. Massachusetts, Alaska and Kentucky have seen their cases more than double in that time, followed by Minnesota, Florida and Texas.
Cases are rising fastest in Arkansas, Florida, Missouri and Nevada, all of which have low vaccination rates, according to Market Watch. In all four of those states, less than half of residents are fully vaccinated.
Vaccine hesitancy remains a problem, with many Americans reluctant to get their shots or unwilling to do so. In May, a Sermo poll showed that more than 72% of physicians surveyed said that patients continue to voice concerns over vaccine side effects.
Still others have reported ongoing misinformation discouraging people from getting vaccines. And close to 30% of physicians reported encountering patients who have skipped their second dose due to unpleasant side effects from the first dose, or concerns over side effects.
We’re a year into the coronavirus pandemic, so the math that undergirds its risks should by now be familiar. We all should know, for example, that the ability of the virus to spread depends on it being able to find a host, someone who is not protected against infection. If you have a group of 10 people, one of whom is infected and nine of whom are immune to the virus, it’s not going to be able to spread anywhere.
That calculus is well known, but there is still some uncertainty at play. To achieve herd immunity — the state where the population of immune people is dense enough to stamp out new infections — how many people need to be protected against the virus? And how good is natural immunity, resistance to infection built through exposure to the virus and contracting covid-19, the disease it causes?
The safe way to increase the number of immune people, thereby probably protecting everyone by limiting the ability of the virus to spread, is through vaccination. More vaccinated people means fewer new infections and fewer infections needed to get close to herd immunity. The closer we get to herd immunity, the safer people are who can’t get vaccinated, such as young children (at least for now).
The challenge the world faces is that the rollout of vaccines has been slow, relatively speaking. The coronavirus vaccines were developed at a lightning pace, but many parts of the world are still waiting for supplies sufficient to broadly immunize their populations. In the United States, the challenge is different: About a quarter of adult Americans say they aren’t planning on getting vaccinated against the virus, according to Economist-YouGov polling released last week.
That’s problematic in part because it means we’re less likely to get to herd immunity without millions more Americans becoming infected. Again, it’s not clear how effective natural immunity will be over the long term as new variants of the virus emerge. So we might continue to see tens of thousands of new infections each day, keeping the population at risk broadly by delaying herd immunity and continuing to add to the pandemic’s death toll in this country.
But we also see from the Economist-YouGov poll the same thing we saw in Gallup polling earlier this month: The people who are least interested in being vaccinated are also the people who are least likely to be concerned about the virus and to take other steps aimed at preventing it from spreading.
In the Economist-YouGov poll, nearly three-quarters of those who say they don’t plan on being vaccinated when they’re eligible also say they’re not too or not at all worried about the virus.
That makes some perverse sense: If you don’t see the virus as a risk, you won’t see the need to get vaccinated. Unfortunately, it also means you’re going to be less likely to do things like wear a mask in public.
Or you might be more likely to view as unnecessary precautions such as avoiding close-quarter contact with friends and family or traveling out of state.
About a quarter of adults hold the view that they won’t be vaccinated when eligible. That’s equivalent to about 64 million Americans.
Who are they? As prior polls have shown, they’re disproportionately political conservatives. At the outset of the pandemic, there was concern that vaccine skepticism would heavily be centered in non-White populations. At the moment, though, the rate of skepticism among those who say they voted for Donald Trump in 2020 and among Republicans is substantially higher than skepticism overall.
That shows up in another way in the Economist poll. Respondents were asked whose medical advice they trusted. Among those who say they don’t plan to get the vaccine, half say they trust Trump’s advice a lot or somewhat — far more than the advice of the Centers for Disease Control and Prevention or the country’s top infectious-disease expert Anthony S. Fauci.
If we look only at Republican skeptics, the difference is much larger: Half of Republican skeptics say they have a lot of trust in Trump’s medical advice.
The irony, of course, is that Trump sees the vaccine as his positive legacy on the pandemic. He’s eager to seize credit for vaccine development and has — sporadically — advocated for Americans to get the vaccine. (He got it himself while still president, without advertising that fact.) It’s his supporters, though, who are most hostile to the idea.
Trump bears most of the responsibility for that, too. Over the course of 2020, worried about reelection, he undercut containment efforts and downplayed the danger of the virus. He undermined experts such as Fauci largely out of concern that continuing to limit economic activity would erode his main argument for his reelection. Over and over, he insisted that the virus was going away without the vaccine, that it was not terribly dangerous and that America should just go about its business as usual — and his supporters heard that message.
They’re still listening to it, as the Economist poll shows. One result may be that the United States doesn’t reach herd immunity through vaccinations and, instead, some large chunk of those tens of millions of skeptics end up being exposed to the virus. Some of them will die. Some may risk repeat infections from new variants against which a vaccine offers better protection. Some of those unable to get vaccinated may also become sick from the virus because we haven’t achieved herd immunity, suffering long-term complications from covid-19.
Trump wants his legacy to be the rollout of the vaccine. His legacy will also probably include fostering skepticism about the vaccine that limits its utility in containing the pandemic.