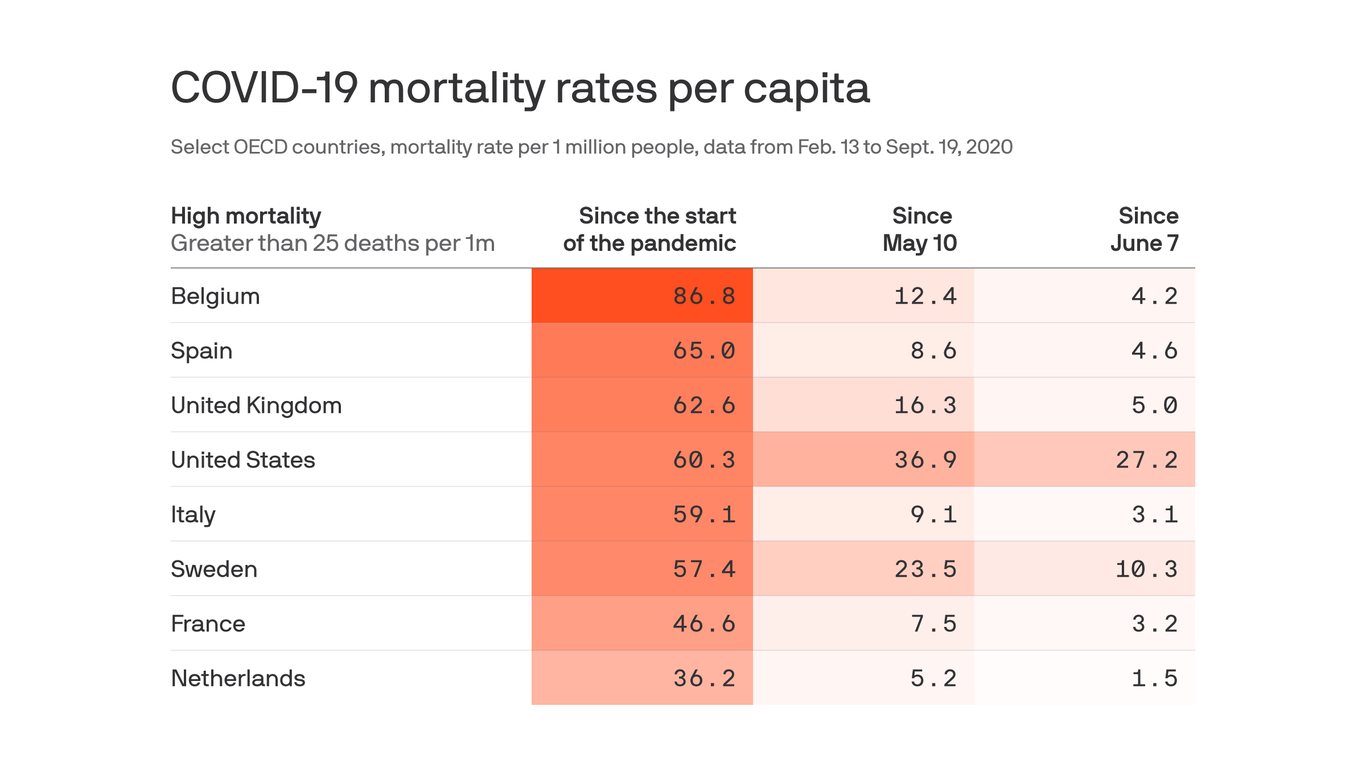
Although other wealthy countries have higher overall coronavirus mortality rates than the United States, the U.S. death rate since May is unrivaled among its peers, according to a new study published in JAMA.
Between the lines:After the first brutal wave of outbreaks, other countries did much better than the U.S. at learning from their mistakes and preventing more of their population from dying.
Why it matters:“If the U.S. had comparable death rates with most high-mortality countries beginning May 10, it would have had 44,210 to 104,177 fewer deaths,” the authors conclude.
Excess deaths have followed a similar pattern: The hardest-hit European countries had similar or higher rates of excess deaths of all causes to the U.S. early on, but these fell much lower than the America did after the first wave.
Yes, but: Death rates are not static, as this study proves, and outbreaks in several European countries have taken a turn for the worse lately.
The COVID-19 pandemic is rife with scientific and medical uncertainty, including debates about the ethics of using experimental treatments.
The big picture: As the global pandemic continues, the tension between providing the best available care for patients and performing trials to determine whether that care is effective risks complicating the medical response.
The big question: Is it unethical to withhold a possible treatment from someone who instead receives a placebo, or to continue to administer that treatment without having collected data on whether it works?
Driving the news: President Trump received an experimental monoclonal antibody cocktail via expanded access or “compassionate use,” which allows someone to access a treatment outside of a clinical trial before it is approved, provided their doctor, the drug company and the FDA agree.
Experts say his subsequent claims of the treatment being a cure risks reducing enrollment in clinical trials, flooding companies with requests for access to a limited number of doses andcreating false hope for patients.
“It’s important that we not say the president got access to a beneficial experimental intervention because we don’t know if it is beneficial or if there are adverse events associated with it,“ says Alex John London, director of the Center for Ethics and Policy at Carnegie Mellon University.
He and other ethicists say the president’s treatment highlights a broader question about the ethical obligation doctors have to the science needed to determine if those treatments are effective.
Between the lines: Offering patients experimental COVID-19 drugs via emergency use authorizations, expanded access programs and compassionate use can slow needed clinical trials.
Researchers have struggled to enroll people in clinical trials in which they may receive a placebo if patients can access a drug directly.
One example: “There’s been some hiccups with the expanded access use for convalescent plasma, because it was something that precluded people from enrolling in a randomized control trial, so it took longer, and we still don’t quite know how well convalescent plasma works,” says Amesh Adalja, an infectious disease physician and senior scholar at the Johns Hopkins Center for Health Security.
More than 100,000 COVID-19 patients at almost 2,800 U.S. hospitals received convalescent plasma from people who survived the virus and developed antibodies to it.
“It’s easy for people to say you enrolled 100,000 people, there should have been a trial. But a small number of those 2,800 hospitals would have been capable of doing those trials,” says the Mayo Clinic’s Michael Joyner, who leads the program.
There are now smaller trials taking place to answer questions about the effectiveness of plasma in treating the disease in different stages.
But if this happens again, Joyner says programs at academic medical centers should be peeled off earlier to form clinical trials run in parallel.
The gold standard for determining whether a treatment works is through randomized controlled trials in which people are randomly assigned to receive a treatment or to be in a control group.
In the uncertainty and urgency of a pandemic, some physicians argue randomizing people to receive a placebo goes against physicians’ ethics and that it is better to do something to help patients than do nothing.
“That’s a false dichotomy because the question is, what should we do?” says London.
From a doctor’s perspective, it’s important to weigh the collective value of theearly drug data and the individual needs of the patient, Adalja says.
“I do think you have to be extra careful when you’re thinking about drugs that you don’t have strong randomized control trial data for, or the data is incomplete or inconclusive,” he adds.
“What people have to ask themselves is what constitutes evidence or proof and where do you want to make the bets in a pandemic?” says Joyner.
“There is a moral, legal and public health obligation to do those trials before people use those products,” says Alison Bateman-House, a professor of medical ethics at NYU’s Grossman School of Medicine who co-chairs an international working group on pre-approval access to treatments.
She says she understands the emotional pull on doctors to help patients whose health is quickly deteriorating, “but it is not evidence-based medicine.”
“There is no ethical obligation to give anyone an unproven substance.”
— Alison Bateman-House, NYU Grossman School of Medicine
In a forthcoming paper, London argues that when medical professionals don’t have the knowledge they need to treat patients, it is their responsibility “to band together and run studies to get evidence to discharge [their] very ancient medical obligation.”
Medical ethics should be updated to include a responsibility to learn in the face of uncertainty, says London, who was part of a committee that called for research to be incorporated into the response to the Ebola outbreak in West Africa in 2014.
The U.K.’s large randomized RECOVERY trial is based in part on the Ebola experience, says London. “Because of it, we know dexamethasone is effective and hydroxychloroquine is not.”
What to watch: How the FDA’s handling of treatments during the pandemic influences other drugs and diseases once the pandemic ends.
The bottom line: “Medicine doesn’t have a good handle on uncertainty, and that is a problem,” says London.
The D.C. Health Department is trying to jump-start contact tracing efforts around the White House’s coronavirus outbreak. Tracing has been inadequate so far even as cases spread deeper into the city, Axios’ Marisa Fernandez writes.
The big picture:The White House has decided not to move forward with recommended public health protocols of contact tracing and testing since President Trump tested positive for the virus.
The state of play: Tracing has been done for people who had direct contact with Trump, White House spokesman Judd Deere told the Washington Post.
On Capitol Hill, there’s also no formalized contact tracing program in place, even as lawmakers themselves test positive.
Two infected staffers in Rep. Doug Lamborn’s (R-Colo.) office were told to not disclose to roommates they may have been exposed, WSJ reports.
The bottom line:The White House’s refusal to contact trace is “a missed opportunity to prevent additional spread,” Emily Wroe, a co-leader of a contact-tracing team at Partners in Health, told Nature.
The quarantining of most of the Joint Chiefs of Staff, coming on the heels of President Trump’s COVID-19 diagnosis, is raising fears that U.S. adversaries might seek to exploit a perceived weakness.
Few expect any sort of overt military action, but there are other ways to wreak havoc on the United States.
Chief among them is disinformation. Experts have been warning ever since Trump tested positive for the coronavirus last week that disinformation is likely to kick into overdrive.
Now, with six of the seven members of the Joint Chiefs of Staff waylaid at home, warnings are being amplified about the national security implications of the growing COVID-19 outbreak among U.S. leadership.
“All these kinds of things are just a huge distraction for us where our national security apparatus is consumed with matters domestic and internal,” former Director of National Intelligence James Clapper said at a Washington Post event after news broke of the Joint Chiefs quarantining. “So this is an ideal time for adversaries, particularly in adversary intelligence services, to look for ways to further confuse us, to distract us.”
Adding that “you can bet particularly our good friends the Russians are doing this,” Clapper warned of them “further sowing seeds of disinformation.”
“They will appeal to all the various tribes and continue to capitalize on the polarization in this country,” he said. “So it is a vulnerable time, and it’s an opportunity for them while we’re not looking and not being alert to further sow seeds of disinformation, casting doubt, discord, distrust in the country.”
The quarantining of top military officers stems from the Coast Guard’s No. 2 admiral contracting COVID-19. The Coast Guard announced Tuesday that its vice commandant, Adm. Charles Ray, tested positive for the coronavirus on Monday after feeling mild symptoms over the weekend.
The test result came after Ray met with most of the Joint Chiefs of Staff at the Pentagon on Friday.
That put Joint Chiefs of Staff Chairman Gen. Mark Milley into quarantine, as well as the chiefs of the Army, Navy, Air Force, Space Force and National Guard. The vice chairman, Gen. John Hyten, was also in the meetings and is quarantining.
The only member of the Joint Chiefs who didn’t meet with Ray was Marine Corps Commandant Gen. David Berger, who was traveling.
Berger’s deputy, Gen. Gary Thomas, met with Ray instead and went into quarantine Tuesday. The Marine Corps announced Wednesday evening that he has tested positive for the virus.
Gen. Paul Nakasone, commander of U.S. Cyber Command and director of the National Security Agency, also met with Ray and went into quarantine.
It’s unclear exactly where Ray caught the virus, but his schedule within the incubation period included a visit to the White House, which is now considered the epicenter of a coronavirus outbreak that includes Trump himself.
Ray — along with Milley, Defense Secretary Mark Esper and other top defense officials — attended a White House ceremony for Gold Star families on Sept. 27.
The event happened the day after Trump announced he was nominating Amy Coney Barrett for the Supreme Court, a gathering for which several attendees have since been diagnosed with COVID-19.
Since Trump’s diagnosis, the Department of Defense has sought to allay any national security concerns.
When Trump’s positive test was first announced last week, the Pentagon insisted there has been “no change to DoD alert levels.”
After news broke Tuesday of the Joint Chiefs quarantining, chief Pentagon spokesman Jonathan Hoffman reiterated that “there is no change to the operational readiness or mission capability of the U.S. Armed Forces.”
“Senior military leaders are able to remain fully mission capable and perform their duties from an alternative work location,” Hoffman said in a statement.
The military chiefs are well-equipped to work from home, and besides Ray and Thomas, none have tested positive for the virus yet.
But the development has raised questions about whether adversaries will try to take advantage of the situation nonetheless.
After the military quarantines were revealed, House Armed Services Committee Chairman Adam Smith (D-Wash.) said “the national security implications of the president’s recklessness cannot be overstated” even though the military “can still operate while leadership is quarantined.”
“Since announcing that he tested positive for the virus, the president’s antics have been downright reckless and harmful,” Smith said in a statement. “Our adversaries are always looking for any weakness to exploit. President Trump’s pathetic attempts to exude strength aren’t fooling anyone — Americans know he is weak and so do those who wish us harm.”
Rep. Jackie Speier (D-Calif.), another senior member of the Armed Services Committee, questioned why so many senior military leaders were meeting in person in the first place, as well as attending a White House reception in which they were pictured maskless.
“What if the Joint Chiefs’ responsibilities cannot be done remotely while they are isolating?” Speier wrote in a series of questions on Twitter. “How many other senior military leaders have tested positive? Why weren’t we safeguarding the health of senior military leaders like the natural security asset that it clearly is?”
Barry Pavel, senior vice president and director of the Atlantic Council’s Scowcroft Center for Strategy and Security, stressed that there is “no degradation in operational command and control” from the Joint Chiefs quarantining.
But, he added, adversaries such as Russia and China could misperceive that the United States is distracted and decide to act. For example, he cited concerns about China moving against Taiwan or Russia trying to grab more territory.
Pavel also listed what he called Russia’s “non-kinetic war” against the United States in the cybersecurity, influence and disinformation realm.
“This is a KGB officer’s most wildest dream coming true almost on a daily basis,” he said. “And so I think it’s a big threat. Who knows what proportion of our current public divisions are sown by Russian influence and bots or are just part of our current division. I don’t know the answer to that question. But they’re certainly right now exploiting it.”
To diminish those concerns, Pavel said, the Pentagon should keep emphasizing its military readiness, as well as demonstrating it by taking actions like publicizing a previously planned exercise.
“It’s probably a good idea to keep repeating those messages,” he said, “to be reiterating those messages, sending them publicly, privately, by third parties and through various forms of military activity so adversaries have no misunderstanding about our readiness and capabilities despite the chairman being quarantined in his quarters.”
The United States needs to “own up to the fact that we didn’t do a good job” up until this point of the Covid-19 pandemic, billionaire and philanthropist Bill Gates said during a Fox News Sunday interview, adding that the slow turnaround for testing results remains “outrageous.”
KEY FACTS
“Unfortunately we did a very poor job and you can just see that in the numbers,” Gates said.
Despite having around 4% of the world’s population, the U.S. has around 22% of all cases with 6,782,083 and about 21% of all reported deaths with 199,411.
The inability to create a testing structure as seen in countries like South Korea “led to us having not just a bad spring, we’ve had a pretty tough summer and sadly because of the seasonality, until we get these new tools, the fall is looking to shape up as pretty tough as well,” Gates said.
“Part of the reluctance I think to fix the testing system now is that nobody wants to admit that it’s still outrageous,” Gates said, adding, “The U.S. has more of these machines, more capacity than other countries by a huge amount, and so partly the reimbursement system is creating perverse incentive.”
After remaining fairly stagnant through the end of summer into September, the U.S. performed a record 1,061,106 Covid-19 tests on Saturday, according to Johns Hopkins University, but labs are still dealing with supply shortages and delays in results.
“We’ll have time to look at those mistakes, which in February and March were really super unfortunate, but we can’t pretend like we get a good grade even today,” Gates said.
CRUCIAL QUOTE
“Even today, people don’t get their results in 24 hours, which it’s outrageous that we still have that,” Gates said.
BIG NUMBER
4.7%. That’s the average positivity percentage in the past week, according to Johns Hopkins.
TANGENT
President Trump has excused the world-leading cases of the coronavirus as a result of the number of tests performed in the country, even saying that he instructed officials to slow testing down. The Centers for Disease Control and Prevention sparked outrage in August when it published new guidelines on testing, recommending people exposed to the virus but not showing symptoms should not get tested. Reports indicate that the guidance was dictated by the Health and Human Services and Trump administration as opposed to CDC scientists. The guidelines were changed again on Friday.
Freshman Sarah Anne Cook carries her belongings as she packs to leave the University of North Carolina at Chapel Hill, on August 18, because of a COVID-19 outbreak. All in-person undergraduate learning was canceled.
On August 10, students at the University of North Carolina at Chapel Hill (UNC) began the fall semester in person. Freshman Jasmine Baker was cautiously optimistic — as an incoming student in the Hussman School of Journalism, she was excited to experience college and get to know her suitemates. But she also worried that the university’s health and safety protocols would not prevent the spread of the coronavirus on campus.
Baker, an out-of-state student, learned about the change in learning plans while attending an in-person class. “The email was very vague about housing,” she told Slate. “There were no specifics. Everyone kind of started freaking out. . . . We learned about it at the same time the professors did.” To top it off, she and a roommate soon tested positive for COVID-19. “We were all in such close quarters,” Baker said. “I know people that barely left their dorms, and they still ended up catching it.”
Experts like Julia Marcus, PhD, MPH, an epidemiologist at Harvard Medical School, and Jessica Gold, MD, MS, a psychiatrist at Washington University, saw this coming from a mile away. “Students will get infected, and universities will rebuke them for it; campuses will close, and students will be blamed for it,” they warned in the Atlantic over the summer.“Relying on the self-control of young adults, rather than deploying the public-health infrastructure needed to control a disease that spreads easily among people who live, eat, study, and socialize together, is not a safe reopening strategy.”
If you put 10,000 [students] in a small space, eating, sleeping, and socializing together, there’ll be an explosion of cases. . . . I don’t know what colleges were expecting.
—UNC epidemiologist Whitney Robinson
As the Editorial Board of the Daily Tar Heel, UNC’s student newspaper, wrote one week into the semester, “Reports of parties throughout the weekend come as no surprise. Though these students are not faultless, it was the University’s responsibility to disincentivize such gatherings by reconsidering its plans to operate in person earlier on.” The local health department recommended that UNC implement remote learning for the first five weeks of the fall term, but administrators ignored that advice.
Lack of Guidelines for Safe Return
Throughout the summer, even as COVID-19 hot spots emerged across the country, President Donald Trump aggressively pushed for schools to reopen in person. Without federal guidance on how to do this safely, university administrators were left to cobble together their own plans for preventing coronavirus from spreading into the community.
“I don’t think there are two universities that have the same protocol,” Irwin Redlener, director of the Pandemic Resource and Response Initiative at Columbia University, told Politico. “It’s national chaos.”
Universities have a strong financial incentive to reopen in person. Many are hoping to recover revenue from housing fees and out-of-state tuition payments that were lost when the pandemic forced them to suspend in-person classes in March. But as many universities have learned in recent weeks, reopening in person comes at a cost to the health of students, faculty members, and the surrounding community.
While California is not represented on USA Today’s list of big outbreaks, it is dealing with surges on some campuses. According to the New York Times campus tracker, there are nearly 2,600 coronavirus cases at 57 schools in California. (Because there is no national tracking system for coronavirus cases on college campuses, the New York Times is believed to have the most comprehensive count available.)
I expect this will blow up outbreaks in places that never had outbreaks, or in places that had outbreaks under control.
—Boston University epidemiologist Eleanor Murray
With 444 confirmed cases, San Diego State University tops the list among California schools, followed by the University of Southern California with 358 cases and UC San Diego with 237. By comparison, North Carolina has nearly 5,200 coronavirus cases at 42 schools, including 1,150 cases at UNC.
California’s relative success at mitigating the spread of COVID-19 on campus can be attributed in part to the conservative reopening plans of many schools. The California State University (CSU) system, California Community Colleges, and University of California (UC) schools moved nearly all fall classes online. UC Berkeley is fully remote for the fall semester. Stanford University planned to have half of its undergraduate students on campus during different quarters, but it switched to mostly remote learning as coronavirus cases continued to rise in the Bay Area over the summer.
Even a hybrid learning model, however, has failed to stave off new coronavirus cases on campuses. Chico State University and San Diego State University, both part of the CSU system, became the first and second California campuses to pause in-person classes after COVID-19 cases spiked, Ashley Smith reported for EdSource.
Resources are a factor in prevention efforts. Chico State’s health center doesn’t have coronavirus tests for students. San Diego State, which has more resources, has two coronavirus testing sites on campus. Across the CSU system, only 2 out of 23 campuses (CSU Maritime Academy and Humboldt State University) have tested all students living in dorms, according to CalMatters. The UC system, which has a budget roughly four times that of the CSU system, is testing all students living in dorms across all 10 campuses. (The UC system has restricted on-campus housing to students who have no alternative housing options.)
An Avoidable Situation
With the academic year off to a rocky start and students being sent home amid coronavirus outbreaks on campuses, experts across the country are nervously tracking the spread of the virus. “I expect this will blow up outbreaks in places that never had outbreaks, or in places that had outbreaks under control,” Eleanor Murray, ScD, MPH, an epidemiologist at Boston University, told Ed Yong in the Atlantic.
COVID-19 surges on college campuses were preventable. “If you put 10,000 [students] in a small space, eating, sleeping, and socializing together, there’ll be an explosion of cases,” Whitney Robinson, PhD, an epidemiologist at UNC, told Yong. “I don’t know what colleges were expecting.”