The Biden administration has declared the monkeypox outbreak a public health emergency — a move that gives officials more flexibility to tackle the virus’ spread.
Details: Department of Health and Human Services secretary Xavier Becerra made the announcement Thursday in a briefing on monkeypox.
Federal health officials can now expedite preventative measures to treat monkeypox without going through a full federal review, the Washington Post reports.
What they’re saying: “We’re prepared to take our response to the next level in addressing this virus,” Becerra said Thursday. “We urge every American to take monkeypox seriously and to take responsibility to help us tackle this virus.”
Dr. Rochelle Walensky, the director of the Centers for Disease Control and Prevention, said the declaration will help “exploit the outbreak” and potentially increase access to care for those at risk.
Dr. Demetre Daskalakis, the White House national monkeypox response deputy coordinator, said “today’s actions will allow us to meet the needs of communities impacted by the virus … and aggressively work to stop this outbreak.”
State of play: Dr. Robert Califf, the commissioner of the Food and Drug Administration, said the U.S. is “at a critical inflection point” in the monkeypox outbreak, requiring “additional solutions to address the rise in infection rates.”
There are 6,600 cases of monkeypox in the U.S. as of Thursday, Becerra said.
There were less than 5,000 cases of monkeypox last week, he added.
The big picture: Biden’s decision to declare monkeypox a public emergency allows him to raise awareness of the virus and unlock more flexibility for spending on ways to treat and tackle the virus.
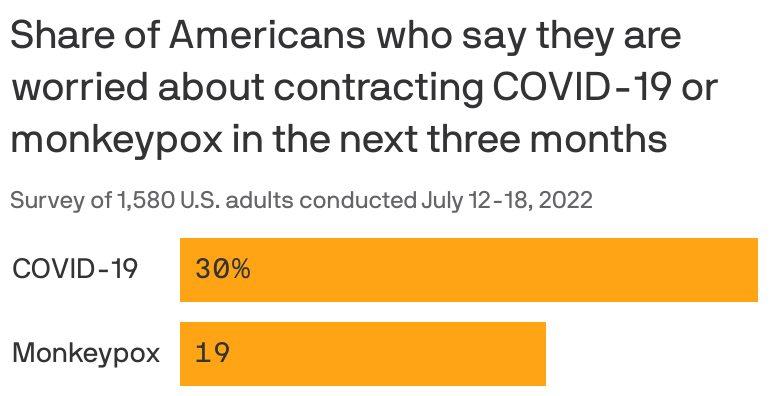
About 20% of Americans are worried they’ll contract monkeypox, Axios previously reported. But there are still some gaps in Americans’ knowledge of the virus and how it impacts our population.
What’s next: U.S. health officials said that 800,000 monkeypox vaccine doses will be made available for distribution. But in hotspot states for the monkeypox outbreak, there’s a drastic disconnect between the number of doses that local health officials say they need versus what they have been allotted.
The U.S. will receive another 150,000 monkeypox vaccine doses in the strategic national stockpile in September, Dawn O’Connell, administrator at HHS’ Administration for Strategic Preparedness & Response, told reporters Thursday. These were previously scheduled to arrive in October.
About 20% of Americans are afraid they’ll soon contract monkeypox, but there are still some significant holes in the public’s understanding of the virus, according to a new survey from the Annenberg Public Policy Center.
The big picture: These early stages of monkeypox outbreaks aren’t nearly as dangerous as early COVID outbreaks were, but some of the challenges for public health officials — like educating people about a virus they’re not familiar with, and mobilizing vaccination efforts — are similar.
By the numbers: One in five Americans are worried about getting monkeypox in the next three months, the Annenberg survey found.
Nearly half are unsure whether monkeypox is less contagious than COVID, although 69% correctly identified the way it usually spreads (through close contact with an infected person).
Two-thirds said they either don’t think there’s a vaccine for monkeypox, or aren’t sure. (There is a vaccine. The Biden administration said Thursday that it’s allocating another 786,000 doses, on top of the more than 340,000 it distributed this month.)
Women were more worried about contracting monkeypox than men, even though the overwhelming majority of cases in the U.S. have been among men.
Between the lines: Memories of false assurances and mixed messaging about the coronavirus in the early days of the pandemic are factoring into public sentiment on monkeypox, said Kathleen Hall Jamieson, director of the Annenberg center.
“There is some suspicion scientists don’t know what they know, so that translates to higher worry,” Jamieson told Axios.
Misinformation and conspiracy theories are also a problem.
12% of respondents in the Annenberg survey said they believe the monkeypox virus was probably or definitely created in a lab; 21% said they were not sure whether it was caused by exposure to a 5G signal.
The fact that the virus has so far spread primarily among men who have sex with men has also fueled widespread perceptions that it’s a sexually transmitted infection, which it is not.
What we’re watching: Perceptions of risk remain fluid and could shift if monkeypox finds new modes of transmission, or if it continues to affect children.
“If kids get it and there’s been no contact with individuals at risk, then you have a completely different situation than you have now,” Jamieson said.
New York state declared an imminent threat and San Francisco issued a state of emergency over monkeypox July 28 as the virus continues to spread in the U.S., NBC News reported.
The news comes after the World Health Organization declared monkeypox a global emergency July 23 and as the CDC reported 4,907 confirmed cases nationwide as of July 28. California and New York account for more than 40 percent of the reported cases in the U.S., according to The Washington Post.
In a statement, New York State Commissioner of Health Mary Bassett, MD, said the declaration allows local health departments “to access additional state reimbursement, after other federal and state funding sources are maximized, to protect all New Yorkers and ultimately limit the spread of monkeypox in our communities.” It covers monkeypox prevention response and activities from June 1 through the end of the year.
In San Francisco, the monkeypox public health emergency takes effect Aug. 1, city officials said in a news release. The release, from Mayor London Breed and the San Francisco Department of Public Health, said the declaration “will mobilize city resources, accelerate emergency planning, streamline staffing, coordinate agencies across the city, allow for future reimbursement by the state and federal governments and raise awareness throughout San Francisco about [monkeypox].”
Four other updates:
1. HHS announced July 28 that nearly 800,000 additional monkeypox vaccine doses will be available for distribution to states and jurisdictions. The 786,000 additional doses are on top of the more than 300,000 doses already distributed. This means the U.S. has secured a total of about 1.1 million doses “that will be in the hands of those who need them in the next several weeks,” HHS Secretary Xavier Becerra said during a July 28 news conference. The additional doses will be allocated based on the total population of at-risk people and the number of new cases in each jurisdiction. “This strategy ensures that jurisdictions have the doses needed to complete the second dose of this two-dose vaccine regimen for those who have been vaccinated over the past month,” HHS said in a news release.
2. As of the morning of July 29, the U.S. has held off on declaring a national monkeypox emergency. Mr. Becerra said July 28 that HHS “continue[s] to monitor the response throughout the country on monkeypox” and will weigh any decision regarding a public health emergency declaration based on the response.
3. The monkeypox response is straining public health workers. Health experts are concerned over how the monkeypox response will further deplete the nation’s public health workforce, still strained and burnt out from the ongoing COVID-19 pandemic. Barriers to testing, treatment and vaccine access largely mirror the missteps in the early coronavirus response, Megan Ranney, MD, emergency physician and academic dean of Brown University School of Public Health in Providence, R.I, told The Washington Post. “I can’t help but wonder if part of the delay is that our public health workforce is so burned out,” she said. “Everyone who’s available to work on epidemiology or contract tracing is already doing it for COVID-19.”
4. Monkeypox testing demand is low, commercial laboratories told CNN. In recent weeks, five major commercial laboratories have begun monkeypox testing, giving the nation capacity to conduct 80,000 tests per week. While Mayo Clinic Laboratories can process 1,000 samples a week, it’s received just 45 specimens from physicians since it began monkeypox testing July 11, according to the July 28 CNNreport. “Without testing, you’re flying blind,” William Morice, MD, PhD, president of Mayo’s lab and chair of the board of directors at the American Clinical Laboratory Association, told the news outlet. “The biggest concern is that you’re not going to identify cases and [monkeypox] could become an endemic illness in this country. That’s something we really have to worry about.”
The World Health Organization (WHO) has declared the monkeypox outbreak a global health emergency after the virus reached more than 70 countries around the world.
WHO Director General Tedros Adhanom Ghebreyesus said at a press conference on Saturday that he decided the outbreak represents a “public health emergency of international concern.”
“WHO’s assessment is that the risk of monkeypox is moderate globally and in all regions, except in the European region where we assess the risk as high,” he said.
Tedros said the WHO’s International Health Regulations Emergency Committee came to a consensus at a meeting a month ago that monkeypox did not represent an international public health emergency, but the situation has changed.
He said the WHO had received reports of just more than 3,000 cases from 47 countries at the time, but more than 16,000 cases have now been reported from 75 countries and territories. He said there have been five deaths.
Tedros said the committee was unable to reach a consensus on whether the outbreak should be considered a public health emergency of international concern, but he considered five factors in declaring it an emergency.
He said the first factor is information countries have shared with the WHO, and that data from countries around the world shows that the virus has spread rapidly to many countries that have not seen it before.
He added that the second factor is the definition of a public health emergency and that the three criteria for declaring such an emergency have been met.
A public health emergency of international concern is considered a situation that is serious, sudden, unusual or unexpected, carries implications for public health beyond a country’s borders and may require immediate international action, according to the WHO.
Tedros said the third factor is the advice of the committee, which was divided, and the fourth factor is scientific principles and evidence, which is currently “insufficient” and leaves “many unknowns.”
He said the fifth factor is the risk to human health, international spread and the potential for interfering with international traffic.
He said there is a “clear risk” for international spread, but the risk of interfering with international traffic is currently low.
“So in short, we have an outbreak that has spread around the world rapidly, through new modes of transmission, about which we understand too little and which meets the criteria in the International Health Regulations,” Tedros said.
The Hill has reached out to the WHO for comment.
Monkeypox has spread quickly in the United States since cases were first detected in the country in May. The virus appears to be spreading primarily among men who have sex with men and spreads through extended physical contact.
The virus can cause symptoms like lesions, a rash and swelling of lymph nodes.
Ghebreyesus said he is making recommendations for four categories of countries in managing monkeypox.
For countries that have not seen any cases or not reported a case in 21 days, they should take measures like activating health mechanisms to prepare to respond to monkeypox and raise awareness about transmission, according to a WHO statement.
Countries with recently imported cases of monkeypox and that are experiencing human-to-human transmission — which includes the United States — should implement a coordinated response, work to engage and protect their communities and implement public health measures like isolating cases and using vaccines.
The Biden administration announced earlier this month that it would distribute an additional 144,000 doses of the Jynneos vaccine to address monkeypox after having distributed about 40,000 doses previously.
The third group of countries are those with the “known or suspected” transmission of the virus from animals to humans. They should establish or activate mechanisms for understanding and monitoring the animal-to-human and human-to-animal transmission risk and study transmission patterns.
The fourth group are countries with the manufacturing capacity to create vaccines and other medical countermeasures. The WHO statement calls on these countries to increase production and availability of these measures and work with WHO to ensure necessary supplies are made available based on public health needs at “reasonable cost” to countries that need support the most.
Ghebreyesus said the outbreak is concentrated among men who have sex with men and especially those with multiple sexual partners.
“That means that this is an outbreak that can be stopped with the right strategies in the right groups,” he said.
He added that countries should work with communities of men with male sexual partners to inform them and offer support and to adopt measures that protect the “health, human rights and dignity of affected communities.”
Ghebreyesus said civil society organizations, especially those with experience working with people who are HIV-positive, should work with WHO to fight stigma and discrimination.
The spread of HIV and AIDS in the 1980s led to increased stigma for those who identify as gay as the virus was initially reported to be spreading among gay men.
The rise of the BA.5 variant is spurring new calls for funding for an Operation Warp Speed 2.0 to accelerate development of next-generation COVID-19 vaccines that can better target new variants.
The BA.5 subvariant of omicron that now makes up the majority of U.S. COVID-19 cases is sparking concern because it has a greater ability to evade the protection of current vaccines than past strains of the virus did.
Pfizer and Moderna are working on updated vaccines that target BA.5 that could be ready this fall, but experts say that by the time they are ready, a new variant very well could have taken hold.
As alternatives to vaccine makers chasing each variant, experts point to research on “pan-coronavirus” vaccines that are “variant-proof,” targeting multiple variants, as well as nasal vaccines that could drastically cut down on transmission of the virus.
There is ongoing research on these next-generation vaccines, but unlike in 2020, when the federal government’s Operation Warp Speed helped speed the development of the original vaccine, there is less funding and assistance this time around.
COVID-19 funding that could help develop and manufacture new vaccines more quickly has been stalled in Congress for months.
“There’s no Operation Warp Speed,” said Eric Topol, professor of molecular medicine at Scripps Research. “So it’s moving very slowly. But at least it’s moving.”
Leana Wen, a public health professor at George Washington University, wrote in a Washington Post op-ed this week that the U.S. needs “urgent investment” in next-generation vaccines and “we need an ‘Operation Warp Speed Part 2.’”
Pfizer and Moderna are working on updated vaccines that target BA.5 that could be ready this fall, but experts say that by the time they are ready, a new variant very well could have taken hold.
As alternatives to vaccine makers chasing each variant, experts point to research on “pan-coronavirus” vaccines that are “variant-proof,” targeting multiple variants, as well as nasal vaccines that could drastically cut down on transmission of the virus.
There is ongoing research on these next-generation vaccines, but unlike in 2020, when the federal government’s Operation Warp Speed helped speed the development of the original vaccine, there is less funding and assistance this time around.
COVID-19 funding that could help develop and manufacture new vaccines more quickly has been stalled in Congress for months.
“There’s no Operation Warp Speed,” said Eric Topol, professor of molecular medicine at Scripps Research. “So it’s moving very slowly. But at least it’s moving.”
Leana Wen, a public health professor at George Washington University, wrote in a Washington Post op-ed this week that the U.S. needs “urgent investment” in next-generation vaccines and “we need an ‘Operation Warp Speed Part 2.’”
Administration health officials pointed to funding when asked about next-generation vaccines at a press briefing on Tuesday.
“We need resources to continue that effort and to accelerate that effort,” said Anthony Fauci, the government’s top infectious disease expert. “So although we’re doing a lot and the field looks promising, in order to continue it, we really do need to have a continual flow of resources to do that.”
But COVID-19 funding has been stuck in Congress for months. Republicans have long said they do not see any urgency in approving the money. Democrats, while generally calling for the funding, have been caught up in their own internal divisions, like when a group of House Democrats objected to a way to pay for the new funding in March.
“Of course more funding would accelerate some parts of the development,” Karin Bok, acting deputy director of the National Institutes of Health’s (NIH) Vaccine Research Center, said in an interview.
She also cautioned that development of next-generation vaccines like nasal vaccines would take longer than the original vaccines, because less groundwork has been laid over the preceding years.
Experts stress that even for BA.5, the current vaccines still provide important protection against severe disease and hospitalization, and are urging people to get their booster shots now. But there is potential for further improvement in the vaccines as well.
Aside from funding, another obstacle is obtaining copies of the existing COVID-19 vaccines for use in research, said Pamela Bjorkman, a California Institute of Technology professor working on a next-generation vaccine.
“I would say we’ve wasted at least six months,” with various procedural hurdles on that front, she said. “It’s just ridiculous.”
For example, she said at one point when her team was able to get access to the AstraZeneca COVID-19 vaccine, it then took two or three months to get an import permit to send it from the United Kingdom.
“This is a hot topic,” Bok, of the NIH, said of access to existing vaccine doses for researchers. “The government is working very hard on an agreement with the companies to provide it to us and to all the investigators…that are funded by NIH.”
Asked about providing vaccine doses for researchers and any talks with the administration on that front, a Moderna spokesperson said: “We do provide vaccine in certain investigator-initiated studies where physicians and scientists propose research they have designed and want to conduct with our support,” pointing to a South African study as an example.
More broadly, the White House says it is working on accelerating next-generation vaccine research and will have more announcements soon.
“Let me be very clear: We clearly need a true next-generation vaccine,” White House COVID-19 response coordinator Ashish Jha told reporters on Tuesday.
“You’ll hear more from us in the days and weeks ahead,” he added. “This is something that we have been working quite assiduously on.”
The rise of ubiquitous self-testing and the paucity of accurate, timely data from the CDC on COVID numbers has left us feeling our way in the dark in terms of the current state of the pandemic. Clearly there’s a new surge underway, driven by the BA.5 variant. What we can report from our experiences on the road over the past few weeks is that the wave is significant.
We’re hearing from our health system members that inpatient COVID volumes and COVID-related ED visits are significantly up again—often double or more what they were just two months ago, although still well below levels of past surges. Length of stay for COVID inpatients is shorter, with fewer ICU visits than during the Delta surge—about the same intensity, proportionally, as during Omicron.
But COVID-related staffing shortages are once again having a real impact on hospitals’ ability to deliver care—clinical and non-clinical staff callouts are at high levels again, as during Omicron.
One piece of good news: masking is back in vogue among many health system executive teams, likely in response to a number of “superspreader” events: gatherings of hospital staff over the past few weeks that resulted in clusters of cases. One system described an all-hands session for anesthesiologists that resulted in more than a dozen cases across the next week—forcing the hospital to cancel procedures.
We’re worried that this BA.5 surge is just getting started, and with booster uptake stagnating and masking all but nonexistent in the general population, the late summer and early autumn situation could be significantly worse.
Figure. Excess deaths in the U.S. relative to other wealthy nations, 1933-2021. Source: Human Mortality Database. Note: Figure shows the difference between the number of deaths that occurred in the U.S. each year and the number of deaths that would have occurred if the U.S. had age-specific mortality rates equal to the average of other wealthy nations. The comparison set includes Austria, Belgium, Canada, Denmark, Finland, France, Germany, Iceland, Italy, Japan, Luxembourg, Netherlands, Norway, Portugal, Spain, Sweden, Switzerland, and the United Kingdom. The average of other wealthy nations excludes Portugal prior to 1940, Austria and Japan prior to 1947, Germany prior to 1956, and Luxembourg prior to 1960. From 1960, all countries are represented (solid dots).
COVID-19 led to a large increase in U.S. deaths. However, even before the pandemic, the U.S. had higher death rates than other wealthy nations. How many deaths could be avoided if the U.S. had the same mortality rates as its peers?
In a new study, we quantify the annual number of U.S. deaths that would have been averted over nearly a century if the U.S. had age-specific mortality rates equal to the average of 18 similarly wealthy nations. We refer to these excess U.S. deaths as “missing Americans.”
The annual number of “missing Americans” increased steadily beginning in the late 1970s, reaching 626,353 in 2019 (Figure). Excess U.S. deaths jumped sharply to 991,868 in 2020 and 1,092,293 in 2021 during the COVID-19 pandemic.
In 2021, nearly 1 out of every 3 U.S. deaths would have been averted if U.S. mortality rates had equaled those of its peer nations. Half of these excess deaths were among U.S. residents under 65 years. We estimate that the 1.1M excess deaths in 2021 were associated with 25M years of life lost, accounting for the number of years the deceased would otherwise be expected to live.
We also compared mortality rates of U.S. racial and ethnic groups with the international benchmark. Black and Native Americans accounted for a disproportionate share of the “missing Americans.” However, the majority of “missing Americans” were White non-Hispanic persons.
Our findings are consistent with recent reports that the life expectancy gap between the U.S. and peer nations widened during the pandemic, with U.S. life expectancy falling from 78.9 to 76.6 years. Life expectancy is widely reported, but it is a complex measure and may be misinterpreted as reflecting small differences in mortality at advanced ages.
In fact, the greatest relative differences in mortality between the U.S. and peer countries occur before age 65. In 2021, half of all deaths to U.S. residents under 65 years – and 90% of the increase in under-65 mortality since 2019 – would have been avoided if the U.S. had the mortality rates of other wealthy nations. In addition to the loss of life, these early deaths often leave behind child (and elder) dependents without key social and economic support.
Our calculations were based on recently released mortality data, obtained from the U.S. Centers for Disease Control and Prevention WONDER Database and the Human Mortality Database. The international comparison group included all available countries with relatively complete mortality data starting in 1960 or earlier, after excluding former communist countries. Our paper builds on prior analyses of excess deaths by our study team and byothers.
We find a very large increase in excess U.S. deaths during the COVID-19 pandemic. However, this spike occurred on top of a growing trend that reached 600,000 excess deaths in 2019. Future COVID-19 deaths could be reduced with broader vaccine uptake, worker protections, and masking during surges. Even if COVID-19 mortality were eliminated, however, the U.S. would likely suffer hundreds of thousands of excess deaths each year, with many linked to firearms, opioids, and obesity.
Addressing excess deaths in the U.S. will require public health and social policies that target the root causes of U.S. health malaise, including fading economic opportunities and rising financial insecurity, structural racism, and failures of institutions at all levels of government to invest adequately in population health.
As this summer heats up, so has the spread of the hot new version of COVID-19.
Why it matters: This subvariant of Omicron called BA.5 — the most transmissible subvariant yet — quickly overtook previous strains to become the dominant version circulating the U.S. and much of the world.
BA.5 is so transmissible — and different enough from previous versions — that even those with immunity from prior Omicron infections may not have to wait long before falling ill again.
What they’re saying: “I had plenty of friends and family who said: ‘I didn’t want to get it but I’m sort of glad I got it because it’s out of the way and I won’t get it again’,” Bob Wachter, chairman of the University of California, San Francisco Department of Medicine told Axios. “Unfortunately that doesn’t hold the way it once did.”
“Even this one bit of good news people found in the gloom, it’s like, ‘Sorry’,” Wachter said.
State of play: This week, the CDC reported BA.5 became the dominant variant in the U.S., accounting for nearly 54% of total COVID cases. Studies show extra mutations in the spike protein make the strain three or four times more resistant to antibodies, though it doesn’t appear to cause more serious illness.
Hospital admissions are starting to trend upward again, CDC data shows, though they’re still well below what was seen during the initial spread of Omicron.
It’s unclear whether that could be indicating an increase in patients in for COVID, or patients who happen to have COVID, Wachter said. “We’re up in hospitalizations around 20% but with a relatively small number of ICU patients,” Wachter said about COVID cases at UCSF.
In South Africa, the variant had no impact on hospitalizations while Portugal saw hospitalizations rise dramatically, Megan Ranney, academic dean at the Brown University School of Public Health told Axios.
“So the big unknown is what effect it’s going to have on the health care system and the numbers of folks living with long COVID,” she said.
Yes, but: “I’m certainly hearing about more reinfections and more fairly quick reinfections than at any other time in the last two and a half years,” Wachter said.
Zoom in: That is also largely the experience of the surge seen firsthand in New York City by Henry Chen, president of SOMOS Community Care, who serves as a primary care physician across three boroughs of the city.
With this particular variant, he said: “The symptoms are pretty much the same but a little bit more severe than the last wave. It’s more high fever, body ache, sore throat and coughing,” Chen said, adding his patient roster is mostly vaccinated.
But it is occurring among patients who’d gotten the virus only three or four months ago, he said.
The big picture: Another summertime wave of cases could prolong the pandemic, coming after many public health precautions were lifted and with available vaccines losing their efficacy against the ever-evolving virus.
The bottom line: The messaging isn’t to panic, but to understand the virus is likely spreading in local communities much more than individuals realize due to shrinking testing programs — and without the level of protection they might assume they have.
“If you don’t want to get sick, you still need to be taking at least some precautions,” Ranney said. “[COVID] is still very much among us.”
Gun violence is a public health problem, but we don’t approach it like one. The debate often gets framed as “guns or no guns” when it isn’t that black and white. In this episode we break down how and why to approach gun violence as a public health problem, what the current research has to say, and what we need to move forward.
What role should the federal government play in addressing major healthcare issues? And does the way you vote affect your prospects for a long and healthy life? We talked about it on today’s episode of the 4sight Friday Roundup podcast.
David Johnson is CEO of 4sight Health.
Julie Vaughan Murchinson is Partner of Transformation Capital and former CEO of Health Evolution.
David Burda is News Editor and Columnist of 4sight Health.