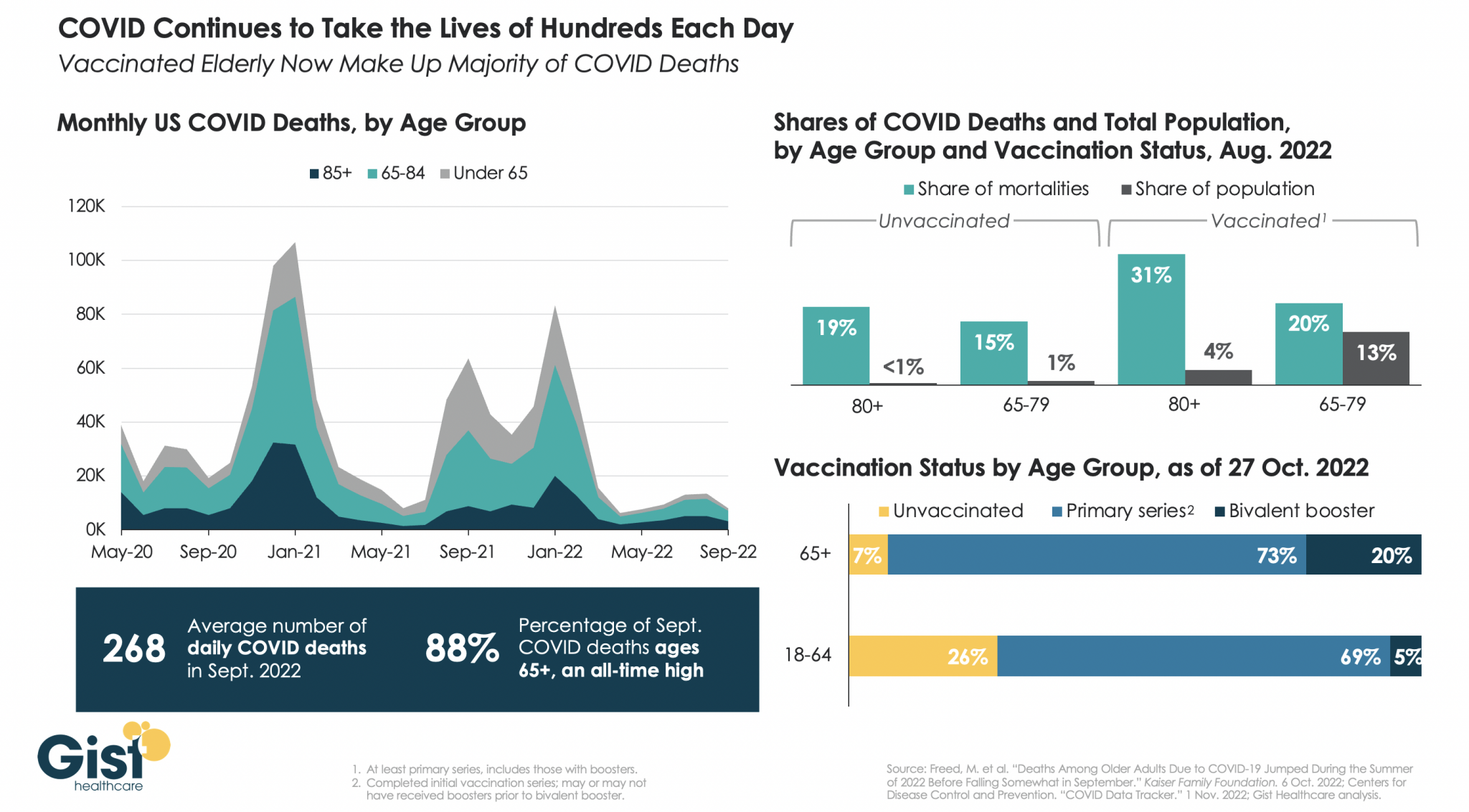
Most experts agree that updated bivalent Covid-19 boosters provide additional protection against serious illness and death among vulnerable populations—but evidence suggests that increased booster uptake may not prevent a “wave of Covid” infections this winter, Apoorva Mandavilli writes for the New York Times.
Can bivalent boosters prevent another surge of infections?
While the Biden administration’s plan to prevent another surge of Covid-19 infections relies on increasing Americans’ uptake of the updated booster doses of the Pfizer–BioNTech and Moderna vaccines, some experts doubt the strategy.
According to John Moore, a virologist at Weill Cornell Medicine, boosters provide additional protection to vulnerable populations—including older adults, immunocompromised individuals, and pregnant people—who should get boosted to prevent severe illness and death.
However, the benefit is not as clear for healthy, younger Americans who “are rarely at risk of severe illness or death from Covid, and at this point most have built immunity through multiple vaccine doses, infections or both,” Mandavilli writes.
“If you’re at medical risk, you should get boosted, or if you’re at psychological risk and worrying yourself to death, go and get boosted,” Moore said. “But don’t believe that will give you some kind of amazing protection against infection, and then go out and party like there’s no tomorrow.”
Separately, Peter Marks, FDA‘s top vaccine regulator, noted the limited data available data for the updated boosters.
“It’s true, we’re not sure how well these vaccines will do yet against preventing symptomatic disease,” he said, especially as the newer variants spread.
However, Marks added, “even modest improvements in vaccine response to the bivalent boosters could have important positive consequences on public health. Given the downside is pretty low here, I think the answer is we really advocate people going out and consider getting that booster.”
How much additional protection do updated shots provide?
While Pfizer-BioNTech and Moderna recently reported that their bivalent boosters produced antibody levels that were four to six times higher than the original vaccine, their results were based on BA.4 and BA.5 antibodies, instead of the more prevalent BQ.1 and BQ.1.1 variants.
According to Mandavilli, “[a] spate of preliminary research suggests that the updated boosters, introduced in September, are only marginally better than the original vaccines at protecting against the newer variants — if at all.”
These small studies have not been reviewed for publication in a journal—but they all came to similar conclusions.
“It’s not likely that any of the vaccines or boosters, no matter how many you get, will provide substantial and sustained protection against acquisition of infection,” said Dan Barouch, head of Beth Israel Deaconess‘ Center for Virology and Vaccine Research, who helped develop Johnson & Johnson‘s vaccine.
Notably, Barouch’s team recently discovered that BQ.1.1 is around seven times more resistant to the body’s immune defenses than BA.5, and 175 times more resistant than the original strain of the coronavirus. “It has the most striking immune escape, and it’s also growing the most rapidly,” he said. BQ.1 will likely follow a similar pattern.
“By now, most Americans have some degree of immunity to the coronavirus, and it does not surprise scientists that the variant that best evades the body’s immune response is likely to outrun its rivals,” Mandavilli writes.
The new vaccine increases antibodies, but the fact it is bivalent may not be significant. In August, a study by Australian immunologists suggested that any kind of booster would offer extra protection. In addition, the study noted that a variant-specific booster would likely not be more effective than the original vaccine.
“The bulk of the benefit is from the provision of a booster dose, irrespective of whether it is a monovalent or bivalent vaccine,” according to the World Health Organization.
Florian Krammer, an immunologist at the Icahn School of Medicine at Mount Sinai, noted that despite recent research, which evaluated immune response soon after vaccination, immune response may improve over time.
“We will see with larger studies and studies at a later time point if there is a good or a significant benefit, but I think it’s certainly not worse,” he added. “I don’t see much risk when you get the vaccine, so you might as well get the benefit.”
“What we need to do right now to get us through the next few months when I think we are in yet another wave of incipient wave of Covid,” Marks added. “And then we need to look forward, and lean into how we’re going to do things differently moving forward.”
Will we see an increase in vaccine uptake?
Currently, FDA allows the booster dose at least two months after a Covid-19 infection or previous does. However, some studies suggest boosting too early could have negative consequences. “Lengthening the interval between boosts to five or six months may be more effective, giving the immune system more time to refine its response,” Mandavilli writes.
Still, “adding yet another shot to the regimen seems unlikely to motivate Americans to opt for the immunization,” no matter the schedule, she adds.
“Each new booster we roll out is going to have a lower and lower uptake, and we’re already pretty close to the floor,” said Gretchen Chapman, an expert in health behavior at Carnegie Mellon University.
Ultimately, “[w]e should not spend a lot of political capital trying to get people to get this bivalent booster, because the benefits are limited,” Chapman added. “It’s more important to get folks who never got the initial vaccine series vaccinated than to get people like me to get their fifth shot.”