Rochester, Minn.-based Mayo Clinic ended the first quarter of 2022 with an operating gain, unlike many health systems acrossthe U.S.
In the quarter ended March 31, Mayo Clinic recorded revenue of $3.9 billion, representing about a 7 percent increase compared to the same period one year prior. The health system saw a boost in medical service revenue and grant revenue, according to its financial report released May 19.
Mayo Clinic’s expenses also rose in the first quarter of 2022 to $3.8 billion. In the comparable quarter in 2021, Mayo Clinic’s expenses were $3.4 billion. The health system attributed the 10 percent expense increase to a boost in salaries and wages as well as supply costs.
Mayo Clinic ended the first quarter of this year with an operating gain of $142 million. In the same quarter last year, Mayo posted operating income of $243 million.
The health system also recorded nonoperating losses of $369 million in the first quarter of 2022.
Despite losses from nonoperating items, Mayo Clinic ended the quarter with $17.5 billion in net assets, up from $13.2 billion recorded in the same period one year prior.
“The year 2022 begins with new challenges that follow nearly two years of pandemic operations,” Mayo Clinic said in the financial report. “Workforce shortages and corresponding labor cost inflation, persistent supply chain disruptions and shortages, a higher interest rate environment, and capital market volatility have all taken center stage for management attention.”
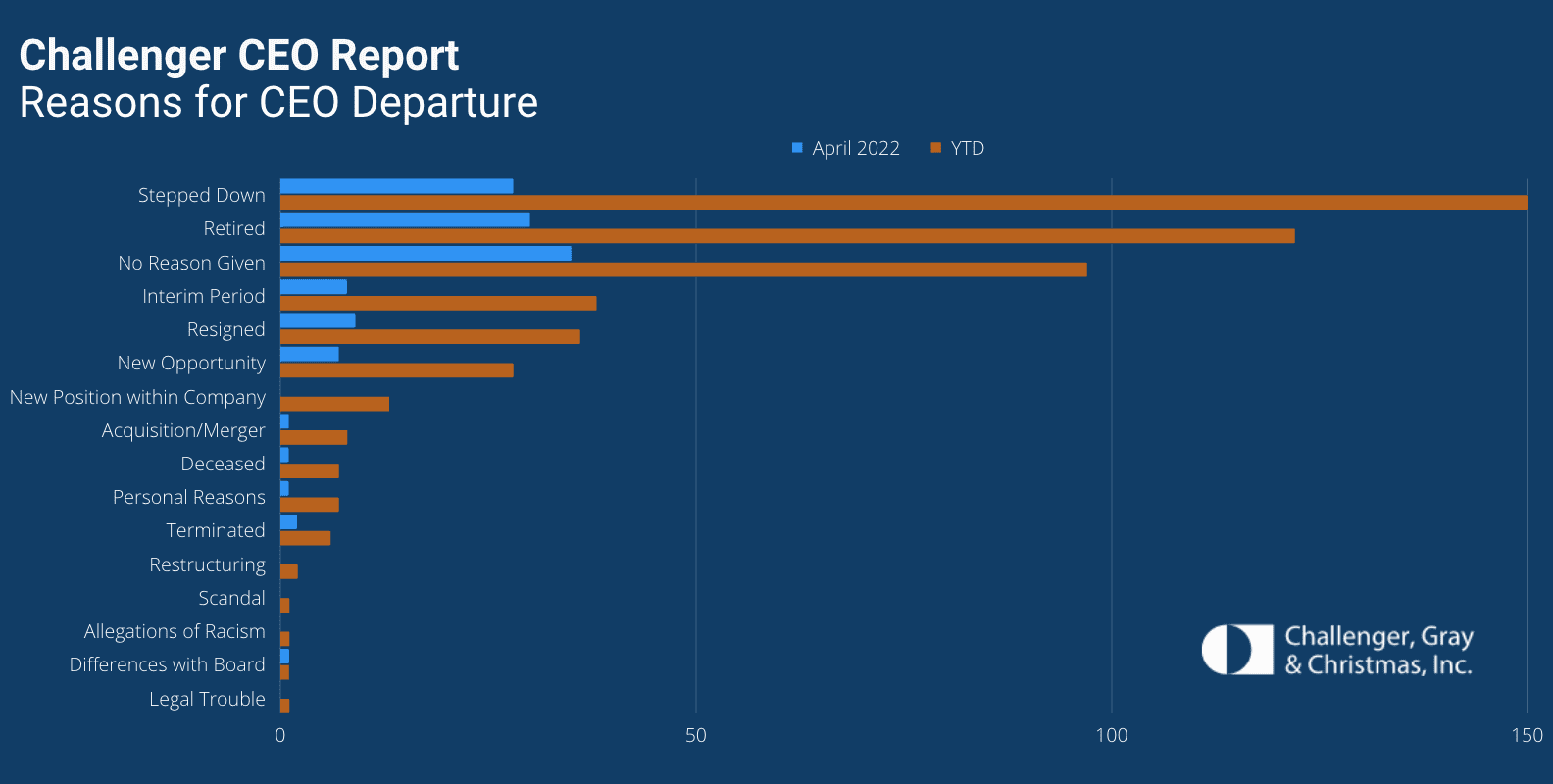
Dozens of hospital CEOs have resigned this year as a record number of chiefs across all industries have exited their roles, according to a May 18 Challenger, Gray & Christmas report.
Nearly 520 CEOs left their posts between Jan. 1 and the end of April, the highest total since the executive outplacement and coaching firm began tracking CEO changes in 2002. The total is up 18 percent from the 440 CEO exits announced in the same period of 2021.
Thirty-six hospital CEOs exited their roles in the first four months of this year. That’s up from the 20 hospital chiefs who resigned in the same period last year, according to the report.
CEOs are leaving their positions and businesses are making changes at the top for several reasons, Challenger, Gray & Christmas Senior Vice President Andrew Challenger said.
“Inflation, staffing shortages, and possible recession concerns are giving more cause for companies to reevaluate leadership,” Mr. Challenger said. “This, after years of companies trying to figure out the right formula to attract and retain talent and create a culture of inclusion, issues that often start at the top.”
Hospitals are feeling an enduring consequence of experienced employees’ early retirements and resignations: collective knowledge loss.
“Even when missing people can be replaced, missing knowledge cannot,” Ed Yong wrote for The AtlanticMay 18.
Beyond hospitals’ challenges in recruiting and retaining employees are the stubborn and sometimes subtle problems resulting from decreasing median tenure within their organizations. The ripple effects of losing older, seasoned employees to resignations or early retirements can be harder to quantify, but are nonetheless felt by colleagues who stay, newcomers to the organization, and patients and their families.
Team tenure is a significant determinant to the cost and quality of hospital care. For example, a one-year increase in the average tenure of registered nurses on a hospital unit was associated with a 1.3 percent decrease in length of stay, a 2014 study from researchers at Columbia University School of Nursing and Columbia Business School found.
“I don’t think the public really understands how great the loss of this generational knowledge is,” Kelley Cabrera, a nurse based in New York, told Mr. Yong. She described the six-week orientation for her current job, led by some people who had been in the ER for less than a year, as “shockingly short.”
“When inexperienced recruits are trained by inexperienced staff, the knowledge deficit deepens, and not just in terms of medical procedures,” Mr. Yong wrote. “The system has also lost indispensable social savvy — how to question an inappropriate decision, or recognize when you’re out of your depth — that acts as a safeguard against medical mistakes. And with established teams now ruptured by resignations, many healthcare workers no longer know — or trust — the people at their side.”
National data on average tenure in healthcare has not yet caught up to compare with pre-pandemic longevity numbers. The median years of tenure with current employers for healthcare practitioners and technical occupations was 4.7 years in 2020, according to the most recent data from the U.S. Bureau of Labor Statistics, ticking up to five years for workers in hospitals.
The benefits of lengthy tenures are felt at the front lines as well as hospitals’ most senior levels. Marc Boom, MD, CEO of Houston Methodist, told Becker’s this year the cumulative tenure of the health system’s executive team was a game changer throughout the pandemic. At the start of the pandemic, Dr. Boom had been CEO for more than eight years and at the institution for almost 22. The executive team of nine leaders, including him, collectively shared more than 150 years of tenure with Houston Methodist. The team had worked together without any changes for about seven years, when the most recent person joined.
This longevity lends itself to major systemwide decisions almost feeling instinctive due to their familiarity working together. “I had a team that was very tenured,” Dr. Boom said. “To work with people who you’ve known for a long period of time — you know the ins and outs, the strengths and weaknesses. You have almost an understood language. You can talk in five-word sentences, move on and everyone goes and does their thing. There are a lot of advantages to that.”
Higher labor costs put pressure on Trinity Health’s margins in the first nine months of fiscal year 2022, according to financial documents released May 20.
Livonia, Mich.-based Trinity Health posted revenue of $15.13 billion in the nine months ended March 31, up from $15.12 billion in the same period a year earlier. The health system said net patient service revenue was up 3.3 percent year over year, primarily because of increased volume and payment rates.
“Patient volumes continue to fluctuate with COVID-19 pandemic surge and recovery waves and patient volumes are returning but have yet to return to pre-pandemic levels,” the system said in an earnings release.
Trinity Health’s operating expenses for the first nine months of fiscal year 2022 increased by 4.8 percent year over year to $15.12 billion. The increase was attributed to a $679.8 million increase in labor costs. Contract labor expenses increased 154.2 percent during the nine-month period.
Trinity Health reported operating income of $139.7 million in the first nine months of fiscal year 2022, down 79 percent from operating income of $653.9 million in the same period a year earlier. Operating income in the first nine months of the current fiscal year included a $128.7 million gain on the sale of Gateway Health Plan.
After factoring in investments and nonoperating items, Trinity posted net income of $43 million for the first nine months of fiscal year 2022, down from $3.19 billion in the same period a year earlier.
Six health system and hospital deals have been canceled so far this year, whether it be a scrapped merger or acquisition or the unwinding of a partnership.
1. Proposed Dartmouth Health, GraniteOne Health merger canceled Lebanon, N.H.-based Dartmouth Health and Manchester, N.H.-based GraniteOne Health are canceling their proposed merger after the state Attorney General’s Office said the move would violate the New Hampshire constitution, according to VTDigger.
2. Hackensack Meridian, Englewood withdraw merger plans Edison, N.J.-based Hackensack Meridian Health and Englewood (N.J.) Health have dropped their merger plans, a spokesperson for Hackensack Meridian told Becker’s.
4. Lifespan, Care New England withdraw merger application The boards of Lifespan and Care New England — both based in Providence, R.I. — have decided to withdraw their merger application after the Federal Trade Commission made an announcement Feb. 17 it would file suit to block the deal.
5. Hoag, Providence to split: 5 things to know Hoag Memorial Hospital Presbyterian in Newport Beach, Calif., and Providence, a Catholic health system based in Renton, Wash., said they would end their affiliation in January.
6. Trinity Health won’t buy Tower Health hospital Trinity Health Mid-Atlantic has abandoned its plan to buy Tower Health’s Chestnut Hill Hospital in Philadelphia, according to the Philadelphia Inquirer.
Amid an international string of cases, a Massachusetts man has been infected with the first case of monkeypox in the United States this year. And while the virus isn’t likely to cause a pandemic like Covid-19, experts say the outbreak is still concerning.
What is monkeypox?
Monkeypox—so called because it was first identified in laboratory monkeys—is a rare viral infection that begins with flu-like symptoms and progresses to a distinctive rash on the face and body. Most infections resolve within weeks, but some cases can be fatal, according to the World Health Organization (WHO).
People can catch monkeypox through contact with infected animals or animal products. Human-to-human transmission, meanwhile, can occur via contact with bodily fluid, sores, or items contaminated by bodily fluid, but most often occurs via large respiratory droplets, which rarely travel more than a few feet.
According to WHO, “There is no evidence, to date, that person-to-person transmission alone can sustain monkeypox infections in the human population.”
Symptoms of monkeypox are typically mild, including headaches, muscle pain, chills, and swollen lymph nodes, The Hill reports. Patients can also develop rashes on their face and body that then turn into skin lesions that eventually fall off.
Although there are no specific treatments for monkeypox, at least one vaccine has been approved in the United States to protect against both monkeypox and smallpox.
Monkeypox cases pop up around the world
On Wednesday, the Massachusetts Department of Public Health (MDPH) reported the first confirmed case this year of monkeypox in the United States in a man who had recently traveled to Canada.
According to MDPH, “The case poses no risk to the public, and the individual is hospitalized and in good condition.”
MDPH said it’s “working closely with the CDC, relevant local boards of health, and the patient’s health care providers to identify individuals who may have been in contact with the patient while he was infectious. This contact tracing approach is the most appropriate given the nature and transmission of the virus.”
Generally, monkeypox cases are very rare in the United States, however two cases were reported in the United States last year—one in Texas and one in Maryland.
Monkeypox cases have also been popping up recently around the world. The United Kingdom has reported nine monkeypox cases, Spain has reported 23 suspected cases, Portugal has reported five and is investigating another 15, and Canadian health officials are investigating at least 15 potential cases in Montreal.
British officials noted that four of the nine cases it identified were among men who have sex with men, suggesting that the virus could be spreading through sexual contract.
What experts are saying
According to Jimmy Whitworth, a professor of international public health at the London School of Hygiene and Tropical Medicine, the monkeypox virus isn’t likely to follow a similar path to Covid-19.
“This isn’t going to cause a nationwide epidemic like COVID did, but it’s a serious outbreak of a serious disease—and we should take it seriously,” he said.
Still, experts said they are concerned by the monkeypox outbreaks. Typically, monkeypox doesn’t spread easily between humans, but the fact that multiple cases are emerging in different countries at the same time is concerning, said Aris Katzourakis, a professor of evolution and genomics at the University of Oxford.
“It’s either a lot of bad luck or something quite unusual happening here,” he said.
“The fact that it’s in the U.K. in multiple unrelated clusters, plus Spain, plus Portugal, is a surprise,” said Tom Inglesby, director of the Johns Hopkins Center for Health Security at the Bloomberg School of Public Health.
According to Mateo Prochazka, an epidemiologist at the U.K. Health Security Agency, the fact that the virus appears to be spreading through sexual contact is especially strange.
“What is even more bizarre is finding cases that appear to have acquired the infection via sexual contact,” he said. “This is a novel route of transmission that will have implications for outbreak response and control.”
While experts aren’t worried about the virus being a global threat as of now, Jay Hooper, a monkeypox expert from the U.S. Army Medical Research Institute of Infectious Diseases, noted that “[e]very time there’s an outbreak—and the more people get infected—the more chances monkeypox has to adapt to people.”
“With viruses that spill over from animals, you just never know what’s going to happen,” he added.
U.S. hospitals performed more than 100,000 surgeries on older patients during the first year of the pandemic, according to a new Lown Institute analysis.
The healthcare think tank relied on Medicare claims data and analyzed eight common low-value procedures. It called the 100,000 procedures unnecessary and potentially harmful in a press release. It found that between March and December 2020, among the most-performed surgeries were coronary stents and back surgeries.
The procedures either offered little to no clinical benefit, according to the institute, or were more likely to harm patients than help them.
“You couldn’t go into your local coffee shop, but hospitals brought people in for all kinds of unnecessary procedures,” Vikas Saini, M.D., president of the Lown Institute, said in a statement. “The fact that a pandemic barely slowed things down shows just how deeply entrenched overuse is in American healthcare.”
Here is the volume of each procedure analyzed, for a total of 106,474 procedures identified:
1. Stents for stable coronary disease: 45,176 2. Vertebroplasty for osteoporosis: 16,553 3. Hysterectomy for benign disease: 14,455 4. Spinal fusion for back pain: 13,541 5. Inferior vena cava filter: 9,595 6. Carotid endarterectomy: 3,667 7. Renal stent: 1,891 8. Knee arthroscopy: 1,596
Among the “U.S. News & World Report” 20 top-ranked hospitals, all had rates of coronary stent procedures above the national average in what the Lown Institute called “overuse.” Four had at least double the national average, including the Cleveland Clinic, Houston Methodist Hospital, Mt. Sinai and Barnes Jewish Hospital. The procedures and overuse criteria were based on previous Lown research.
“We’ve known for over a decade that we shouldn’t be putting so many stents into patients with stable coronary disease, but we do it anyway,” Saini said. “As a cardiologist, it’s frustrating to see this behavior continue at such high levels, especially during the pandemic.”
In response to the Lown analysis, the American Hospital Association said in a statement Tuesday that delays or cancelations in non-emergency care may have negative outcomes on patients. “Lown may define these services as ‘low value,‘ but they can be of tremendous value to the patients who receive them,” the statement read.
It also pointed to its response to last year’s Lown analysis, which it criticized as being based “on data that are not only incomplete, but also not current.” The organization argued the services surveyed only represent a portion of the care hospitals provide. It added that procedures are determined by physicians based on an evaluation of the patient’s medical needs.
Despite substantial operating margin declines during the first year of COVID-19, U.S. hospitals were able to keep their finances on track thanks to billions in government relief funds, Johns Hopkins researchers wrote in a new study published Friday in JAMA Health Forum.
Per their analysis of Centers for Medicare and Medicaid Services (CMS) Hospital Cost Reports data, researchers found that thousands of hospitals broadly maintained their overall profit margins thanks to a boost in “other nonoperating income,” the category under which hospitals recorded the collective $175 billion in subsidies Congress allocated to support healthcare facilities and clinicians.
This was particularly the case for government, rural and smaller hospitals that typically run on tighter margins, the researchers wrote. Because they, by design, received more targeted relief than other types of hospitals, these facilities were able to record higher overall profit margins in 2020 than in prior years.
“Hospital operations were really hit hard during the pandemic,” Ge Bai, professor in the Bloomberg School’s Department of Health Policy and Management, a professor of accounting at the Johns Hopkins Carey Business School and an author of the study, said in a statement.
“Our study shows that the relief funds provided an important lifeline to keep financially weak hospitals up and running.”
Among the study’s sample of 1,378 hospitals, mean operating margin declined from –1.0% in 2019 to –7.4% in 2020, representing the hit facilities took to their operations prior to the relief funding.
Those hospitals’ mean overall profit margin during the first year of the pandemic was 6.7%, which the researchers wrote was stable in light of the preceding four years and across all ownership types, geographic locations and hospital sizes.
The difference-maker, they wrote, was an increase in other nonoperating income as a share of a hospital’s total revenue. While that mean share was 4.4% in 2019, it jumped to 10.3% in 2020 thanks to the government relief funds.
Additionally, certain types of hospitals with traditionally lower overall profit margins saw significant improvements in 2020. These included government hospitals (3.7% to 7.2%), rural hospitals (1.9% to 7.5%) and hospitals with fewer admissions (3.5% to 6.7%).
“Hospitals that tend to serve socioeconomically disadvantaged patients and more who are uninsured are the most vulnerable to financial losses,” Yang Wang, a doctoral student in the Bloomberg School’s Department of Health Policy and Management and the study’s first author, said in a statement. “But the extra federal funding helped them stay operational.”
The researchers’ study included hospitals with fiscal years beginning in January whose financial data were compiled and processed as part of RAND Hospital Data, which in turn pulls its data from CMS’ Medicare Cost Reports. The findings persisted among a second sample of 785 hospitals from the database with fiscal years beginning in July.
The government’s distribution of COVID-19 relief funds to providers has faced some critique from healthcare policy researchers, some of whom suggested that the methodology led to funding skewed toward hospitals serving well-insured communities.
Much of the relief set aside for hospitals has since run dry or is on its last legs as of early 2022. With COVID hospitalizations again ticking upward and earlier surges still unaccounted for, industry groups and the Biden administration alike are pushing Congress for more relief support.
RWJBarnabas Health (RWJBH) and Saint Peter’s Healthcare System’s proposed integration has received the blessing of New Jersey regulators, a key step forward as the systems look to form what they describe as the state’s “first premier academic medical center,” according to a Monday announcement.
The organizations are now awaiting a final approval from the Federal Trade Commission (FTC) before moving ahead with the deal.
“State approval now puts us on the cusp of being able to create New Jersey’s first multi-campus premier academic medical center that will draw top talent, increased research funding and more opportunities for groundbreaking clinical trials, while also enhancing specialized services and improving overall patient care,” Saint Peter’s President and CEO Leslie Hirsch said in a statement.
“New Jersey deserves to have a premier academic medical center of national distinction like many other states that will serve as a destination for patients from all walks of life to get lifesaving treatment for complex illnesses and as an anchor for medical innovation, educational opportunity and economic development,” Hirsch said.
The organizations said that in addition to increasing services and strengthening patient access, the premier academic medical center’s location in New Brunswick, New Jersey, would play a role in attracting more academic talent and research to nearby Rutgers University.
The systems’ announcement also cited affirmation from Superior Court Judge Lisa Vignuolo, who said when authorizing the transaction that the deal “will serve in the public interest and the public good.”
RWJBH is the larger of the pair, providing care to more than 3 million patients annually across 11 hospitals, four children’s hospitals and dozens of other centers. It’s already the largest academic health system in New Jersey thanks to a collaboration with Rutgers Robert Wood Johnson Medical Schools to train over 1,000 medical residents and interns across RWJBH hospitals yearly.
Formed in 2007, Saint Peter’s Healthcare System is a Catholic organization headlined by the 478-bed Saint Peter’s University Hospital in New Brunswick. It also operates a children’s hospital, primary and specialty care networks and a surgical center.
Under the previously announced terms of the agreement, Saint Peter’s would remain a full-service acute healthcare provider in New Jersey and continue to adhere to its Catholic healthcare mission. RWJBH would make significant strategic capital investments in St. Peter’s facilities, technology and innovation.
“This is a tremendous milestone in a years-long journey towards fulfilling our shared vision to bring transformative care to New Jersey,” RWJBH CEO Barry Ostrowsky said in a statement.
Regulators’ green light for RWJBH’s moves contrasts with the recent opposition to Hackensack Meridian Health and Englewood Health’s now-nixed merger plans. The FTC and half of the country’s state attorneys general fought the proposal due to concerns that it would remove competition and harm residents in New Jersey’s Bergen County.