Last week, President-elect Donald Trump announced that Robert F. Kennedy, Jr. would be his nominee for Secretary of Health and Human Services (HHS). He followed this up on Tuesday with his selection of Dr. Mehmet Oz as his nominee for the Centers for Medicare and Medicaid Services (CMS) Administrator. If confirmed, the two men would replace Xavier Becerra and Chiquita Brooks-LaSure, respectively.
Kennedy, who ended his independent presidential campaign and endorsed Trump in August, has become known for his heterodox views on public health, including vaccine skepticism and opposition to water fluoridization.
Dr. Oz, first famous as a TV personality and more recently a Republican candidate for Pennsylvania Senator, is a strong proponent of Medicare Advantage, having co-authored an op-ed advocating for “Medicare Advantage for All” in 2020.
The Gist:
These nominees, especially Kennedy, hold a number of personal beliefs at odds with the public health consensus.
They are both likely to be confirmed, however, as the last cabinet nominee to be rejected by the Senate was John Tower in 1989. (This does not include nominees who have chosen to withdraw themselves from consideration, as former Representative Matt Gaetz has just done.)
Should they be confirmed, they will be responsible for implementing not their own but President Trump’s agenda, the specific priorities of which also remain relatively undefined.
However, possible consensus points between Trump and his nominees include public health cuts and deregulation, greater scrutiny of pharmaceutical companies, and a favoring of Medicare Advantage over traditional Medicare.
Artificial intelligence has long been heralded as a transformative force in medicine. Yet, until recently, its potential has remained largely unfulfilled.
Consider the story of MYCIN, a “rule-based” AI system developed in the 1970s at Stanford University to help diagnose infections and recommend antibiotics. Though MYCIN showed early promise, it relied on rigid, predetermined rules and lacked the flexibility to handle unexpected or complex cases that arise in real-world medicine. Ultimately, the technology of the time couldn’t match the nuanced judgment of skilled clinicians, and MYCIN never achieved widespread clinical use.
Fast forward to 2011, when IBM’s Watson gained global notoriety by besting renowned Jeopardy! champions Ken Jennings and Brad Rutter. Soon after, IBM applied Watson’s vast computing power to healthcare, envisioning it as a gamechanger in oncology. Tasked with synthesizing data from medical literature and patient records at Memorial Sloan Kettering, Watson aimed to recommend tailored cancer treatments.
However, the AI struggled to provide reliable, relevant recommendations—not because of any computational shortcoming but due to inconsistent, often incomplete, data sources. These included imprecise electronic health record entries and research articles that leaned too heavily toward favorable conclusions, failing to hold up in real-world clinical settings. IBM shut down the project in 2020.
Today, healthcare and tech leaders question whether the latest wave of AI tools—including much-heralded generative artificial intelligence models—will deliver on their promise in medicine or become footnotes in history like MYCIN and Watson.
Anthropic CEO Dario Amodei is among the AI optimists. Last month, in a sprawling 15,000-word essay, he predicted that AI would soon reshape humanity’s future. He claimed that by 2026, AI tools (presumably including Anthropic’s Claude) will become “smarter than a Nobel Prize winner.”
Specific to human health, Amodei touted AI’s ability to eliminate infectious diseases, prevent genetic disorders and double life expectancy to 150 years—all within the next decade.
When people ask me how to separate AI hype from reality in medicine, I suggest starting with three critical questions:
Question 1: Will the AI solution speed up a process or task that humans could eventually complete on their own?
Sometimes, scientists have the knowledge and expertise to solve complex medical problems but are limited by time and cost. In these situations, AI tools can deliver remarkable breakthroughs.
Consider AlphaFold2, a system developed by Google DeepMind to predict how proteins fold into their three-dimensional structures. For decades, researchers struggled to map these large, intricate molecules—the exact shape of each protein requiring years and millions of dollars to decipher. Yet, understanding these structures is invaluable, as they reveal how proteins function, interact and contribute to diseases.
With deep learning and massive datasets, AlphaFold2 accomplished in days what would have taken labs decades, predicting hundreds of proteins’ structures. Within four years, it mapped all known proteins—a feat that won DeepMind researchers a Nobel Prize in Chemistry and is now accelerating drug discovery and medical research.
Another example is a collaborative project between the University of Pittsburgh and Carnegie Mellon, where AI analyzed electronic health records to identify adverse drug interactions. Traditionally, this process took months of manual review to uncover just a few risks. With AI, researchers were able to examine thousands of medications in days, drastically improving speed and accuracy.
These achievements show that when science has a clear path but lacks the speed, tools and scale for execution, AI can bridge the gap. In fact, if today’s generative AI technology existed in the 1990s, ChatGPT estimates it could have sequenced the entire human genome in less than a year—a project that originally took 13 years and $2.7 billion.
Applying this criterion to Amodei’s assertion that AI will soon eliminate most infectious diseases, I believe this goal is realistic. Today’s AI technology already analyzes vast amounts of data on drug efficacy and side effects, discovering new uses for existing medications. AI is also proving effective in guiding the development of new drugs and may help address the growing issue of antibiotic resistance. I agree with Amodei that AI will be able to accomplish in a few years what otherwise would have taken scientists decades, offering fresh hope in the fight against human pathogens.
Question 2: Does the complexity of human genetics make the problem unsolvable, no matter how smart the technology?
Imagine searching for a needle in a giant haystack. When a single answer is hidden within mountains of data, AI can find it much faster than humans alone. But if that “needle” is metallic dust, scattered across multiple haystacks, the challenge becomes insurmountable, even for AI.
This analogy captures why certain medical problems remain beyond AI’s reach. In his essay, Amodei predicts that generative AI will eliminate most genetic disorders, cure cancer and prevent Alzheimer’s within a decade.
While AI will undoubtedly deepen our understanding of the human genome, many of the diseases Amodei highlights as curable are “multifactorial,” meaning they result from the combined impact of dozens of genes, plus environmental and lifestyle factors. To better understand why this complexity limits AI’s reach, let’s first examine simpler, single-gene disorders, where the potential for AI-driven treatment is more promising.
For certain genetic disorders, like BRCA-linked cancers or sickle cell disease that result from a single-gene abnormality, AI can play a valuable role by helping researchers identify and potentially use CRISPR, an advanced gene-editing tool, to directly edit these mutations to reduce disease risk.
Yet even with single-gene conditions, treatment is complex.CRISPR-based therapies for sickle cell, for example, require harvesting stem cells, editing them in a lab and reinfusing them after risky conditioning treatments that pose significant health threats to patients.
Knowing this, it’s evident that the complications would only multiply when editing multifactorial congenital diseases like cleft lip and palate—or complex diseases that manifest later in life, including cardiovascular disease and cancer.
Put simply, editing dozens of genes simultaneously would introduce severe threats to health, most likely exceeding the benefits. Whereas generative AI’s capabilities are accelerating at an exponential rate, gene-editing technologies like CRISPR face strict limitations in human biology. Our bodies have intricate, interdependent functions. This means correcting multiple genetic issues in tandem would disrupt essential biological functions in unpredictable, probably fatal ways.
No matter how advanced an AI tool may become in identifying genetic patterns, inherent biological constraints mean that multifactorial diseases will remain unsolvable. In this respect, Amodei’s prediction about curing genetic diseases will prove only partially correct.
Question 3: Will the AI’s success depend on people changing their behaviors?
One of the greatest challenges for AI applications in medicine isn’t technological but psychological: it’s about navigating human behavior and our tendency toward illogical or biased decisions. While we might assume that people will do everything they can to prolong their lives, human emotions and habits tell a different story.
Consider the management of chronic diseases like hypertension and diabetes. In this battle, technology can be a strong ally. Advanced home monitoring and wearable devices currently track blood pressure, glucose and oxygen levels with impressive accuracy. Soon, AI systems will analyze these readings, recommend diet and exercise adjustments and alert patients and clinicians when medication changes are needed.
But even the most sophisticated AI tools can’t force patients to reliably follow medical advice—or ensure that doctors will respond to every alert.
Humans are flawed, forgetful and fallible. Patients skip doses, ignore dietary recommendations and abandon exercise goals. On the clinician side, busy schedules, burnout and competing priorities often lead to missed opportunities for timely interventions. These behavioral factors add layers of unpredictability and unresponsiveness that even the most accurate AI systems cannot overcome.
And in addition to behavioral challenges, there are biological issues that limit the human lifespan. As we grow older, the protective caps on our chromosomes wear down, causing cells to stop functioning. Our cells’ energy sources, called mitochondria, gradually fail, weakening our bodies until vital organs cease to function. Short of replacing every cell and tissue in our bodies, our organs will eventually give out. And even if generative AI could tell us exactly what we needed to do to prevent these failings, it is unlikely people would consistently follow the recommendations.
For these reasons, Amodei’s boldest prediction—that longevity will double to 150 years within a decade—won’t happen. AI offers remarkable tools and intelligence. It will expand our knowledge far beyond anything we can imagine today. But ultimately, it cannot override the natural and complex limitations of human life: aging parts and illogical behaviors.
In the end, you should embrace AI promises when they build on scientific research. But when they violate biological or psychological principles, don’t believe the hype.
Last week, the Senate Permanent Subcommittee on Investigations, led by Sen. Richard Blumenthal (D-Connecticut), released a Majority Staff Report on rampant prior authorization (PA) abuses in Medicare Advantage (MA).
The report offers unique insight into recent trends in the use of prior authorization by Medicare Advantage plans and the strategy and motives behind insurance corporations’ use of it.
While the findings won’t surprise those who’ve been following health policy trends, it is immensely concerning that between 2019 and 2022, the prior authorization denial rate for post-acute care in UnitedHealth’s Medicare Advantage plans doubled.
The denial rate for long-term acute care hospitals in Humana’s Medicare Advantage plans increased by 54% from 2020 to 2022. During this time, UnitedHealth, CVS/Aetna, and Humana increased their use of artificial intelligence (AI) for prior authorization reviews, often resulting in increasing denial numbers and decreasing (or absent) review time by human beings.
The report recommends that the Centers for Medicare and Medicaid Services (CMS) collect additional data, conduct audits of prior authorization processes, and expand regulations on the use of technology in PA reviews. While these recommendations would be positive steps, the report’s findings call into question whether Big Insurance can ever be trusted or regulated enough to prevent abuse of patients through prior authorization and other mechanisms.
This report provides an in-depth look at insurers’ motivations. Sadly, those motivations are not to “make sure a service or prescription is a clinically appropriate option,” as UnitedHealth claims, but to decrease the amount spent on medical care to increase the corporations’ profits.
The report noted that CVS, which owns Aetna, saved $660 million in 2018 by denying Medicare Advantage patients’ claims for treatment at inpatient facilities. Around the same time, CVS found in its testing of a model to “maximize approvals,” which would be a good thing for patients, that the model jeopardized profits because it would lead to more care being covered. In 2022, CVS “deprioritized” a plan to increase auto-approvals because of the lost “savings” from denying patient care.
The report found that the motivation to increase profits, without regard for patient care, was not unique to CVS/Aetna.
UnitedHealth’s naviHealth subsidiary provided this directive to its employees: “IMPORTANT: Do NOT guide providers or give providers answers to the questions” when speaking to a patient’s doctor about a prior authorization request. Instead of working collaboratively with doctors to get patients the care they need, UnitedHealth told its workers not to bother. In a training session offered to Humana employees involved in prior authorization reviews, the company explained that reviewers should deny a request for post-acute care even if a patient needed more intensive treatment. Humana told reviewers that the lack of an in-network lower-level care facility for patients to go to was not a reason to approve post-acute care and that usually the situations can be “sorted out,” presumably by the patient with no help from the insurer.
All three companies (UnitedHealth, Humana and CVS/Aetna), which dominate the Medicare Advantage program, demonstrated a striking lack of motivation to protect and enhance patient care, instead showing a primary motivation to increase profits and margins.
The subcommittee’s report also noted that UnitedHealth, CVS/Aerna, and Humana are increasingly using AI to make care decisions and cutting humans, especially doctors, out of the process. The researchers found that in 2022, UnitedHealth looked into how using AI and machine learning could aid in predicting which denials of post-acute care requests were most likely to be overturned. One would hope this effort would be to decrease the number of wrongfully denied prior authorization requests and increase patient access to care.
However, the report includes a quote from a recap of a meeting on the project asking “what we could do in the clinical review process to change the outcome of the appeal,” meaning that UnitedHealth was interested in preventing the overturning of denials, not getting the decision right in the first place. The report also found evidence that naviHealth used artificial intelligence to help determine the coverage decisions for a patient’s post-acute care claim before any human post-acute care providers evaluated a case. The report’s authors found that denials for post-acute care facilities rose rapidly once naviHealth began managing these requests for UnitedHealth’s MA plans.
These are just some of the findings in the 54-page report on Big Insurance’s use of prior authorization to deny Medicare Advantage patient requests for post-acute care.
The report’s findings demonstrate the abuse of prior authorization by the insurers, the motivation to increase profit and decrease patient care, and the use of AI to increase denials. Further, the findings underscore that prior authorization is a tool used by Big Insurance primarily to maximize profits. The report puts forward recommendations to cut down on abusive denials, which would have some positive impact.
More importantly, I believe the report provides more evidence that it is becoming exceedingly less likely that private and for-profit insurance companies can be regulated and act in a way that promotes patient health over profits.
With the election looming and the beginning of annual open enrollment periods for health insurance plans, it is vital to pull back the curtain on the influx of money from Big Insurance corporations to political campaigns and lobbying.
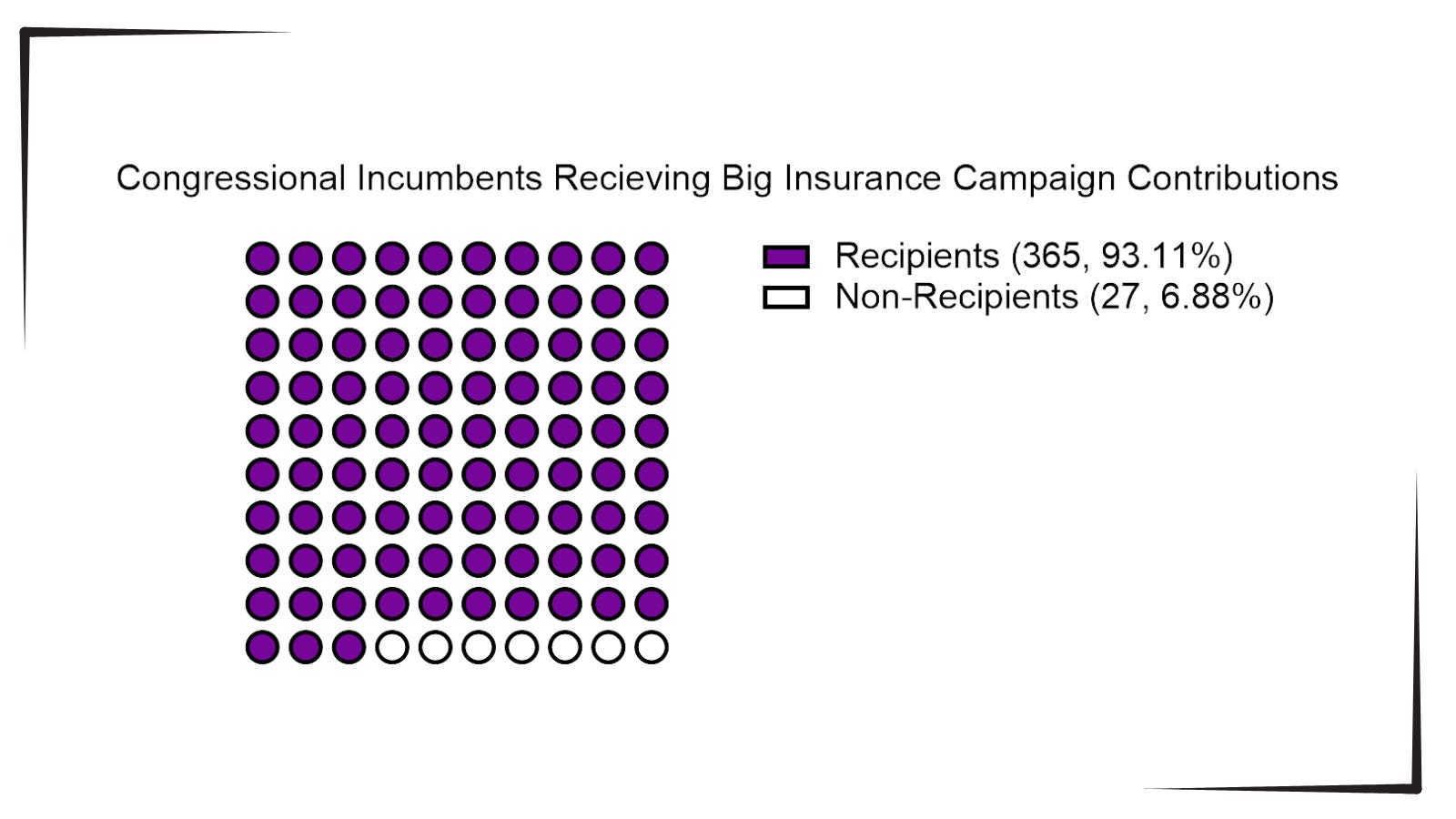
Data available from OpenSecrets.com thus far in 2024 shows that 93% of Congressional incumbents running in 2024 received contributions from Big Insurance, including 100% of Senate incumbents. These insurance corporations run the ten largest Medicare Advantage plans in the country and are known to deny needed health care and defraud the government, but face little to no consequences.
Insurance corporations included in this analysis are UnitedHealth Group, Humana, CVS/Aetna, Kaiser Permanente, Elevance Health, Centene Corp, Cigna, Blue Cross Blue Shield Association (which represents many MA plans, including two of the largest: BCBSMichigan and Highmark), and SCAN.
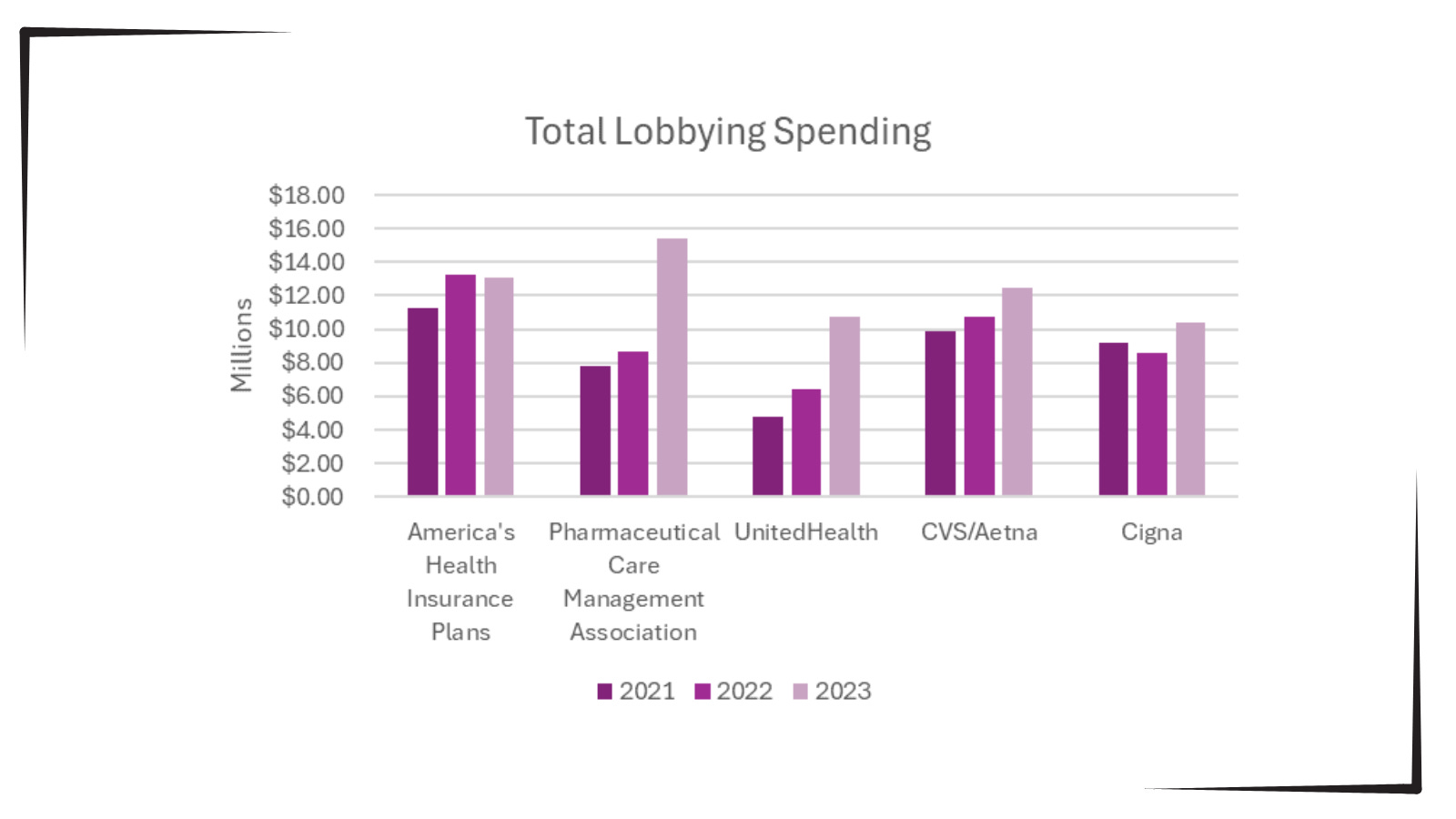
Additionally, as bipartisan scrutiny of pharmacy benefit managers (PBMs) and Medicare Advantage plans has intensified, spending by Big Insurance on lobbying has increased.
Total lobbying spending by America’s Health Insurance Plans; Pharmaceutical Care Management Association; UnitedHealth; CVS/Aetna; and Cigna for the years 2021, 2022 and 2023.
This open enrollment season, people struggling to choose a health insurance plan that they can afford and that provides the care they need may ask themselves, “Why is our health care system like this?” The immense amounts of money Big Insurance spends to blanket members of Congress with contributions and lobbying hold the answer.
Additional analysis following the election will allow evaluation of just how much Big Insurance spends on politics to help protect industry profits and will give health reform advocates an idea of how to overcome this influence to pass policies for patients, not profits.
Innovation in the American economy over the past 30 years has been nothing short of stunning—one remarkable technological advance after another. Industry by industry and product by product, corporate innovation has profoundly changed the way we navigate our economic and consumer lives. From this context of technological and innovative change came the corporate belief that healthcare could be “significantly improved” through the same application of aggressive corporate strategy and innovation.
So along came Walmart, Walgreens, CVS, and Amazon with all the resources in the world and with the best intentions to contemporize primary care.
The goals of all this were front and center: change the definition of the healthcare gatekeeper, lower costs, improve quality, and create a much more consumer-friendly care experience. Yet here we see that American business has proven—once again—that the best intentions, the smartest ideas, and a lot of money are still no guarantee of commercial success. How quickly the corporate retail re-invention of primary care all came apart.
Between 2017 and 2022, retail clinic claims grew 200%, spiking particularly during the pandemic, according to Healthcare Finance. And yet now, Walmart has abandoned its primary care strategy, Walgreens is pulling back significantly—even after announcing significant expansion plans as little as a year ago—and CVS is facing uncertainty after a leadership shakeup.
Under corporate leadership and strategy, primary care has become a catalog of woes. Let’s unpack that catalog.
Walmart opened its first health center in 2019, offering a range of basic services with prices posted. At first, it focused on patients who could pay cash, but eventually evolved to accept a range of insurance plans. Walmart brought a level of strategic aggression to its primary care initiative by announcing in 2023 it would nearly double the number of clinics it operated. But in an abrupt about face, the megaretailer shuttered all 51 primary care locations in April, citing an unsustainable business model with an inability to maximize revenue and adequately control expenses.
Walgreens, on the other hand, opted to invest in existing providers. In 2020 and 2021, Walgreens spent $6.2 billion on the primary care clinic chain VillageMD, establishing it as the majority owner. In 2022, Walgreens sunk another $3.5 billion, through a mix of debt and equity, into VillageMD’s $8.9 billion acquisition of Summit Health. Walgreens, like Walmart, suffered for its primary care investments. The company was forced to take a $5.8 billion write-down on Village MD in the second quarter of this year.
During an October 15 earnings call, Walgreens CEO Tim Wentworth said the company “is reorienting to its legacy strength as a retail pharmacy-led company,” according to the Wall Street Journal. “We are in the early stages of a turnaround that will take time.” And that comment came with the potential closure of 1,200 Walgreens retail locations, following on the heels of 160 primary care clinic closures earlier this year.
CVS, too, has not been immune to primary care turbulence, as CVS Health CEO Karen Lynch was forced to step down last month after presiding over an expansion of healthcare clinics but then closing dozens of them in California and New England. CVS’s strategic approach revolved around its $10.6 billion acquisition of Oak Street Health in 2023 and its intention to expand primary care in 1,100 MinuteClinics. That strategy now seems to be up in the air with the departure of Ms. Lynch. The CVS board is now suggesting an approach that may involve a spinoff of its insurance and pharmacy benefits manager units, Aetna and Caremark.
Amazon, however, at the moment shows no signs of abandoning its foray into primary care. Rather than focusing its efforts on solely brick-and-mortar locations, Amazon organized its primary care strategy around the 2023 $3.9 billion acquisition of One Medical, a concierge-style service designed to facilitate both in-person and virtual visits. While Amazon’s primary care strategy remains somewhat opaque, it seems to revolve around partnering with employers and health systems to cultivate primary care patient loyalty through a membership program that builds on the Amazon Prime brand.
Each company took a slightly different approach to primary care, but all four planned to leverage their exceptional size to achieve profitability.
Interestingly, scale has not been sufficient to solve the challenges of primary care. American Medical Association President Bruce A. Scott wrote recently: “If retail giants can’t make today’s care delivery model work financially, how on earth can physicians in private practice?” It’s no wonder the ongoing shortage of about 20,000 primary care physicians is expected to persist. A recent AAMC report found that by 2036, that number could double.
Primary care has been unsuccessful as a transactional business; retailers sell goods at a set price and send customers on their way. In healthcare, payment models are nowhere near as straightforward. Patients, particularly in areas where access to care is limited, may have continuous, rather than episodic, needs. All of this complexity has seemed to add up to higher costs and lower margins. Primary care seems to require a much more complex business model, one robust enough to remain patient as that business model experiments with various approaches or is vast enough to offset losses with other lines of revenue.
So where does all of the above lead us? Are there any useful conclusions or lessons to be learned? Maybe so.
Primary care is an essential component of any hospital system of care. Done right, it acts as both an important gatekeeper and as a trusting component of the continuity of healthcare service.
At the moment, there is not enough primary care to meet the demand. Stories abound of patients whose longtime primary care physicians retire and said physicians cannot be replaced without a great effort—or often not at all.
Right now, the economics of primary care don’t work as a standalone service. Many have tried and—regardless of whether they were big or small, for profit or not-for-profit—this essential patient-centered service can only operate when subsidized by a larger enterprise. Walmart, Walgreens, and CVS have all tired of those subsidies.
The overall healthcare system and its quality of care and delivery is significantly damaged by the current state of primary care. Too many patients receive delayed diagnosis and treatment and slow or little necessary follow-up. Patients that should be seen in the office are instead funneled to the emergency room. Care, of course, remains well-intentioned but often is instead inconsistent and chaotic. Conditions that might have been deftly managed instead become chronic.
All this leads to the importance of not giving up on primary care. Patients prefer to be seen in the primary care ecosystem. They tend to trust that level of care and attention. Patients also prefer to be seen in-person when they are feeling particularly poorly, and they appreciate prompt answers about concerning health issues. What this all suggests is that we are at a moment when hospitals need to double down on the primary care dilemma. Primary care needs to be examined as an essential component of the overall enterprise-wide strategic plan both clinically and—especially—financially.
Corporate America, with all of its economic power and resources and scale, has found primary care to be a confounding and, so far, unsuccessful business model. So, after all of the recent noise and promises and slide decks, the problem and promise of primary care is back in the mission-driven hands of America’s not-for-profit hospitals—exactly where it should have been all along.
While speculation swirls around key cabinet appointments in the incoming Trump administration, much is being written about how things might change for industries and the companies that compose them. Healthcare is no exception.
Speculation about possible changes originates from media coverage, healthcare trade associations, law firms, consultancies, think tanks and academics. Their views are primarily based on Trump Healthcare 1.0 initiatives (2017-2021), presumed Trump 2.0 leverage in the U.S. Senate, House and conservative Supreme Court and a belief by the Trump-team leaders that their mandate is to lower costs for “everyday Americans” and tighten border security.
Thus, Trump Healthcare 2.0 policy changes will be extensive, leveraging legislation, executive orders, agency administrative actions, court decisions and appropriations processes to reset the U.S. health system.
Context:
The red shift that enabled the 45th President to regain the White House was fueled by discontent and fear: discontent with prices paid by ordinary consumers and fear that illegal immigration was an existential threat. Abortion was an important concern to women but inflation and prices for gas, groceries, housing and healthcare mattered more. Exit polls indicate voter concern about how Trump 2.0 economic policies (tariffs et al) might inflate consumer prices or add up to $7 trillion to the national debt was low. And the fate of the Affordable Care Act was a non-issue: assurance about protection for pre-existing condition coverage neutered attention to other elements of the ACA that will get attention in Trump Healthcare 2.0 (i.e. subsidies, short-term plans, et al).
The Four Pillars of Trump Healthcare 2.0 Policy Changes
The new administration is inclined toward a transactional view of the U.S. health system. It does not envision transformational change; instead, it sees opportunity for the system to perform significantly better. Its policies, leadership appointments and actions will be predicated on these four pillars:
Access to the U.S. healthcare system is a right to be earned. Fundamentally, Trump Healthcare 2.0 builds on its moral conviction that there should be NO FREE LUNCHES whether it’s illegal immigrants or patients who use the health system without doing their part. Trump Healthcare 2.0 will advance mechanisms to enable self-care, increase personal responsibility, promote cheaper/better alternatives to traditional insurance and health delivery and challenge lawmakers to limit financial support to free-loaders. The fundamental notions of public health and community benefit will be revisited and restrictions enacted.
The status quo is not working. Change is needed. Polls show the majority of Americans are dissatisfied with the health system. Affordability is their major concern: escalating, inexplicable costs are forcing their employers to share more responsibility. Trump Healthcare 2.0 will implement changes that lower spending and costs for consumers and employers. They’ll leverage coalitions of working-class voters and businesses to enact policies that expose waste, fraud and abuse in the system and direct the U.S. Department of Health & Human Services to streamline its structure and prioritize cost-effectiveness (the HHS Strategic Plan for 2022-2026 is up for review).
Private solutions solve public problems better than government. Trump Healthcare 2.0 posits that government is broken including the federal and state agencies that control healthcare oversight and funding. Reducing regulatory barriers to consolidation and innovation and lessening risks for private investors whose ventures align with Trump Healthcare 2.0 priorities will be foci. Fundamentally, Trump Healthcare 2.0 believes the private sector is better able to address problems than government bureaucrats: key Trump Healthcare 2.0 leadership positions will be filled by successful private sector operators instead of re-cycled DC luminaries desiring attention.
Price transparency fuels competition and value. Trump Healthcare 1.0 mandated hospital price transparency via its 2019 Executive Order: Trump Healthcare 2.0 will expand the scope and usefulness of price transparency mandates in hospital, ancillary and outpatient services, physician services, insurance and others. It will facilitate accelerated use of Artificial Intelligence in decision-making by consumers, providers and payers. It will expand timely access to data on prices, direct costs, overhead, executive compensation, outcomes, user experiences and other elements of care management provided by hospitals, physicians and other providers. And it will move quickly to implement site neutral payments in the 119th Trump Healthcare 2.0 holds that providers, insurers and drug companies are not inclined to transparency despite strong support from elected officials and voters. They’ll advance these policy changes anticipating pushback from industry insiders. Trump Healthcare 2.0 believes price transparency in healthcare will produce transformational changes that enable more competition and lower costs.
Looking ahead:
The Trump 2.0 team’s immediate task is to assemble its Cabinet: that’s taken prior administrations 38 days on average to complete. In tandem, temporary fixes for CMS’ pending Physician Pay Cut and telehealth expansion will pass as Congress’ lame duck session begins this week.
Looking to 2025, the Trump Healthcare 2.0 team will focus initially on issues in Congress where Bipartisan support appears strong i.e. regulation of PBMs, implementation of site neutral payment policies, expansion of drugs subject to Inflation Reduction Act’s pricing limits and perhaps others. It will plan its legislative agenda coordinating with key committees (i.e. Senate HELP, House Ways and Means et al) and outside groups that share its predisposition. And it will use its political clout to build popular support for healthcare reforms that respond directly to consumer (voter) concern about affordability.
Trump Healthcare 2.0 will bring heightened transparency to the health system and be premised on pillars that are popular with working class voters. It will not be a duplicate of Trump Healthcare 1.0: it will be much more.
Congressional Republicans are beginning to discuss overhauling Medicaid using a process that would allow the Senate to bypass the required 60-vote threshold to pass certain priorities, according to GOP lawmakers.
Why it matters:
The changes could significantly reshape a safety net program that covers more than 70 million people, reducing federal spending and potentially leading to significant coverage losses.
Driving the news:
Perhaps the most likely Medicaid change would be imposing work requirements for recipients, according to GOP sources.
That idea was discussed as part of last year’s debt ceiling talks and is familiar to GOP lawmakers.
House Majority Leader Steve Scalise (R-La.) told Axios that Medicaid work requirements “potentially” could be included in a legislative package brought up under the fast-track budget procedure known as reconciliation.
Asked about other Medicaid spending changes, Scalise said members “have a lot of internal conversations to have about all the things that will be included.”
Yes, but:
It’s not clear how much, if any, health policy will be packed into a reconciliation bill, since the overriding focus of the package would be on extending major provisions of the Trump 2017 tax law.
There has been less recent enthusiasm for controversial health policy changes among Republicans, who’d prefer to focus on taxes, energy and immigration.
However, a health package could generate valuable savings to help pay for some of the tax cuts, and Medicaid is a large pot of money, costing over $800 billion per year.
Congressional scorekeepers previously estimated work requirements would save over $100 billion over 10 years — and 600,000 people would become uninsured.
What they’re saying:
Rep. Brett Guthrie (R-Ky.), one of two leading contenders to be chair of the House Energy and Commerce Committee in the next Congress, told Axios he is interested in capping Medicaid spending on each enrollee, known as a “per capita cap” or allotment.
This would be a revival of a proposal from the 2017 Affordable Care Act repeal-replace plan.
“We offered Medicaid reform in reconciliation in the repeal-and-replace package, and it was per capita allotments, which didn’t cut Medicaid but it does limit the growth,” Guthrie said.
“I do think it has to be discussed as part of the package” next year, he said, adding he hadn’t discussed the idea with leadership yet.
Between the lines:
Another potential change is reducing the federal share of spending on the Medicaid expansion population, currently at 90%, so that it matches the lower federal share for the traditional Medicaid population.
“It makes no sense for federal policy to pay states more for able-bodied enrollees than for disabled people, children and pregnant women on the program,” said Brian Blase, president of the Paragon Health Institute and a former Trump administration health official.
The flip side is that a cash crunch in the states could lead some to drop the Medicaid expansion altogether. Forty states have expanded their programs.
The big picture:
The first Trump administration approved Medicaid waivers for conservative-led states that imposed work and reporting requirements. But courts struck down many of the approvals.
Republicans could be wary of political blowback from efforts to reshape the entitlement program this time around.
Protests against Medicaid cuts, as well as possible resistance from some Republican governors, helped doom the repeal-replace effort in 2017.
Democrats also are sure to portray any Medicaid cuts as penalizing the poor to help lower taxes on the wealthy.
Rep. Morgan Griffith (R-Va.), an Energy and Commerce Committee member, acknowledged “people get scared” when Medicaid work requirements are discussed, but he noted the possibility of exemptions for people with disabilities or those in school.
There have been “some private conversations” though “nothing formal” in the committee about Medicaid changes, he said.
The bottom line:
“It’s hard to make adjustments to reduce federal spending without touching people who rely on the program,” said Robin Rudowitz, director of the Program on Medicaid and the Uninsured at KFF.
Back in February, Dr. Philip Verhoef and I wrote an op-ed for STAT News warning both patients and investors to steer clear of the health insurance industry’s private version of Medicare, which the government continues to allow insurers to market as Medicare Advantage.
As we enter the open enrollment period in which America’s seniors and disabled people are able to choose between the traditional Medicare program and a bewildering array of private plans, it’s a good time to remind you why you need to steer clear of Medicare Advantage.
Millions of people enrolled in those private plans are now getting notices from their insurers that their plans will not be available in 2025 because
three of the biggest insurance corporations (Humana, CVS/Aetna and Cigna) – and probably several smaller insurers – have decided to stop selling MA plans in hundreds of communities across the country, which means that MA enrollees in all those places are going to have to go through the agonizing chore of finding a replacement.
Why? Because Wall Street, which until this year was head-over-heels in love with Medicare Advantage, is now filing for divorce.
Investors have been running for the exits since they began seeing danger signs in for-profit insurers’ earnings reports in the last quarter of 2023. For at least two of the biggest players in MA – Humana and CVS – that exodus has in recent weeks turned into a stampede. The stock prices of those two companies have been in steep decline all year, and you can be certain the top executives of those companies are now in panic mode.
People who’ve been following my work since I blew the whistle on the health insurance racket know I’ve been trying to educate seniors – and policymakers – for at least a dozen years, going back to my time at the Center for Public Integrity, about the many shortcomings of what I’ve often called Medicare Disadvantage. I’ve also called Medicare Advantage the biggest heist of taxpayers’ dollars in American history. It’s truly epic.
The truth is that MA has been a broken system since the beginning, especially for patients. The business worked only as long as insurers were able to extract inappropriately large payments from the Medicare fund through methods like upcoding, where plans list false or exaggerated diagnoses on patient charts to get more money while providing no additional care.
In fact, the MA model relies on providing as little care as possible in general, with insurers putting care approval behind a wall of delays and denials to save money and leaving patients suffering without necessary treatment.
We wrote that op-ed just as the government began taking long-overdue steps to rein in some of those abuses and, to Wall Street’s shock, announced at the end of February that it would not be giving MA plans as much money going forward as the industry had expected. That announcement, coupled with the reins-tightening, really spooked investors.
But that wasn’t all that soured them on Medicare Advantage. The big MA insurers had to admit to Wall Street when they released quarterly earnings that despite their best efforts to delay and deny as much care as possible, seniors nevertheless were using more health care than before.
The insurers’ medical loss ratios were ticking up, meaning they were having to use more of their customers’ premiums (and Medicare fund money) paying claims than they had anticipated. And folks, Wall Street HATES it when insurers do that.
Phil and I wrote that:
Before, investors had assumed MA plans could keep the business humming along, that private insurers would always be able to keep their enrollees’ use of medical goods and services in check, and that policymakers would always look the other way as the government doled out billions in overpayments annually. They now see that these assumptions are failing, and many have sold their holdings in these companies as a result.
The selling has continued apace throughout 2024, and the biggest loser on Wall Street has been Humana, which currently has an 18% share of the MA market, second behind UnitedHealth’s 29%. CVS/Aetna’s shares have also been dropping like a rock.
Humana got another kick to the stomach from investors this week when it admitted that it likely will lose billions of dollars in payments in the future because far fewer of its MA enrollees will be in so-called four-star rated MA plans – 25% in 2025 compared to 94% in 2024. The feds give four-star rated MA plans a lot more money than lower-rated plans.
When the New York Stock Exchange closed yesterday, Humana’s share price had fallen to $241.37. That’s down more than 54% since the 52-week high of $530.54 it reached in October 2023. But get this: on Wednesday the share price reached a 52-week low of $213.31 before inching back up later in the day as some investors apparently saw a way to make money at some point down the road by buying at that low price.
And folks, that was not just a 52-week low. The last time Humana’s share price was in that territory was on April 25, 2017, when the low for the day was $214.51.
All this turmoil has led Bank of America Securities to downgrade the stock to “underperform,” another word for sell. Piper Sandler also downgraded the company yesterday. Those downgrades – and possibly more to come – could cause the stock price to sink even further.
Having worked closely with Humana’s C-suite and investor relations people when I headed corporation communications there before going to Cigna, I can assure you the company’s top brass are grasping at any levers they can get their hands on to stop the freefall. I would not want to be one of them, and I certainly would not want to be one of their customers or investors.
As I mentioned, Humana, UnitedHealth and CVS/Aetna are by far the biggest players in the MA game. Earlier this year, those three companies captured 86% of the 1.7 million new MA enrollees, thanks to spending untold millions of federal dollars on deceptive TV ads and other marketing schemes.
Humana is now dumping hundreds of thousands of its MA enrollees because they somehow managed to get the care they needed. The company is doing that for one single reason: to try to get back into Wall Street’s good graces.
Next week we’ll look at how the other two big players in Medicare Advantage, UnitedHealthcare and CVS/Aetna, are faring on Wall Street. It is a tale of two cities, as you’ll see.
In a surprising turn of events, sources say that CVS Health is exploring the possibility of breaking up its business empire — a move that could unravel years of aggressive vertical integration, including its $70 billion acquisition of health insurer Aetna back in 2017.
While details are still slim, such a move signals just how dire the situation has become for CVSHealth as it navigates mounting financial and regulatory pressures on multiple fronts.
It’s yet another chapter in a story that has seen CVSHealth evolve from a retail pharmacy chain into a health care behemoth — but perhaps one that grew too big, too fast. And to be honest, I’m not surprised. I’ve seen this movie before. In fact, I saw it many times – although each time with different stars – during my 20 years in the health insurance business. One of the most memorable featured Aetna, which in the late 1990s and early 2000s had to retrench, at Wall Street’s insistence, after a buying spree of smaller health insurers that brought the company a ton of unprofitable accounts and disappointing bottom lines. Aetna followed its buying spree with a purging spree, dumping as many as eight million health plan enrollees in short order to get back into Wall Street’s good graces.
It seems that CVSHealth also bought too much too fast. The results? Rising expenses, frustrated patients, and now potential cracks in the corporate structure itself.
CVS: A Cautionary Tale of Vertical Integration
Large corporations like CVS and its peers have used their size to dominate various aspects of health care—whether it’s insurance, retail pharmacy, physician practices and clinics, and controlling the drug supply chain. But as these mega-corporations continue to grow, they also become harder to manage, and their inefficiencies start to become evident.
CVS’s acquisition of Aetna was hailed at the time as a strategic masterstroke — a way to streamline health care by bringing together the different parts of the system under one corporate umbrella. It was supposed to deliver “efficiencies” that would benefit both the company and patients.
But it’s not just the purchase of Aetna. From pharmacy benefit manager Caremark to Aetna to health care providers Signify Health and Oak Street Health — CVS’s business model has become increasingly complex, making it difficult to navigate regulatory scrutiny, rising costs and fierce competition in the retail pharmacy space.
The latest reports suggest that CVS’s board is trying to figure out where Caremark would land in the event of a breakup. Would it stay with the retail side or with the insurance arm?
This isn’t just an internal debate; it’s emblematic of the broader issue—CVS has built a vertically integrated structure that was supposed to work together to improve care, but investors are now questioning how and even if these pieces should fit together.
It’s Been a Hard Few Years for CVS
Federal Trade Commission’s Legal Action Against CVS’s Caremark and Other PBMs
Instead, those supposed efficiencies have largely translated into higher costs for consumers and increased scrutiny from regulators, especially with CVS’s Caremark at the center of anti-competitive practices allegations by the Federal Trade Commission (FTC). PBMs like Caremark control the drug pricing landscape in ways that lack transparency and disproportionately affect patients and independent pharmacies.
Now, as CVS grapples with rising medical costs within its Aetna business — just like its biggest competitors, UnitedHealth and Humana —the company’s management appears to be in damage control mode. While nothing is certain, discussions about splitting the business have reached the boardroom level, according to sources familiar with the matter. This comes as activist investors, like Glenview Capital, push for structural changes to improve CVS’s declining financial performance.
CVS’s Aetna Medicare Advantage Loss in New York City
New York City Mayor Eric Adams had a plan to force city municipal retirees out of traditional Medicare and into a corporate Aetna Medicare Advantage plan. The NYC Organization of Public Service Retirees vehemently opposed the move and spent months fighting it.
In August, a Manhattan Supreme Court judge permanently halted the mayor and Aetna’s attempts.
Wall Street Woes
For CVS Health, 2024 started off bad. CVS missed Wall Street financial analyst’s earnings-per-share expectations for the first quarter of 2024 by several cents. Shareholders’ furor sent CVS’ stock price tumbling from $67.71 to a 15-year low of $54 at one point.
Also in August, CVS Health cut its 2024 forecast for a third time, citing troubles covering seniors via the company’s private Medicare Advantage business. Operating income for CVS Health’s insurance arm, Aetna, dropped a whopping 39% in Q3, which forced the company to shake up its leadership – moving CEO Karen Lynch into the role of managing insurance and publicly firing one of her lieutenants, Executive Vice President Brian Kane.
What’s Next?
The notion that CVS could split its operations would effectively unwind one of the most high-profile health care mergers in recent memory. A split up of the company would mark the end of an era in which health care conglomerates could grow unchecked. CVS’s struggle isn’t happening in isolation—other companies, like Walgreens and Rite Aid, are facing similar financial difficulties and structural questions.
CVS’s potential breakup could signal a broader industry trend toward unwinding massive, vertically integrated health care corporations.
Whether CVS breaks up or not, it’s clear that the model of health care mega-mergers, designed to consolidate power and increase corporate profits, is facing serious headwinds. Cigna recently announced that it is getting out of the Medicare Advantage business and Humana is getting out of the commercial insurance market. UnitedHealth, meanwhile, so far seems to be weathering those headwinds, but it, too, will be facing even more scrutiny by lawmakers and regulators in the months and years ahead.
UnitedHealth Group has taken a beating on Wall Street this week after admitting that its Medicare Advantage plans had to pay out more in medical claims in the third quarter of this year than investors had expected. As I’ve noted many times, Wall Street can’t stand it and gets very spiteful when Big Insurance uses more of our premium dollars paying for patients’ care because that means there’s less money left over to enrich shareholders.
At the end of trading at the New York Stock Exchange Tuesday, UnitedHealth’s share price was down 8.11% — almost $50 a share — falling like a rock from $605.40 to $556.29 as soon as the market opened. It had reached a 52-week high just the day before but fell off a cliff Tuesday morning. This despite the fact that the company still made $8.7 billion in operating profits during the third quarter.
What investors didn’t like at all was the fact that UnitedHealthcare’s medical loss ratio (MLR) climbed to 85.2% from 82.3% for the same period last year.
By other measures, the company did just fine, especially when you look at how much money it made during the first nine months of this year: a whopping $24.5 billion in profits.
Enrollment in both the company’s commercial and Medicare Advantage plans increased, but it posted a significant decline in the number of people enrolled in the Medicaid plans its administers for several states. That’s because of the Medicaid “unwinding” that has been going on since the official end of the pandemic.
And here is another couple of numbers of note from the third quarter:
UnitedHealth’s Optum division, which encompasses its massive pharmacy benefit manager, Optum Rx, made more money for the parent company than the health plan division: $4.5 billion in profits vs. $4.2 billion for UnitedHealthcare.
PBMs have become even more of a cash cow for Big Insurance than Medicare Advantage, which despite the higher MLRs of late is still a reliable money-gushing ATM for the industry.