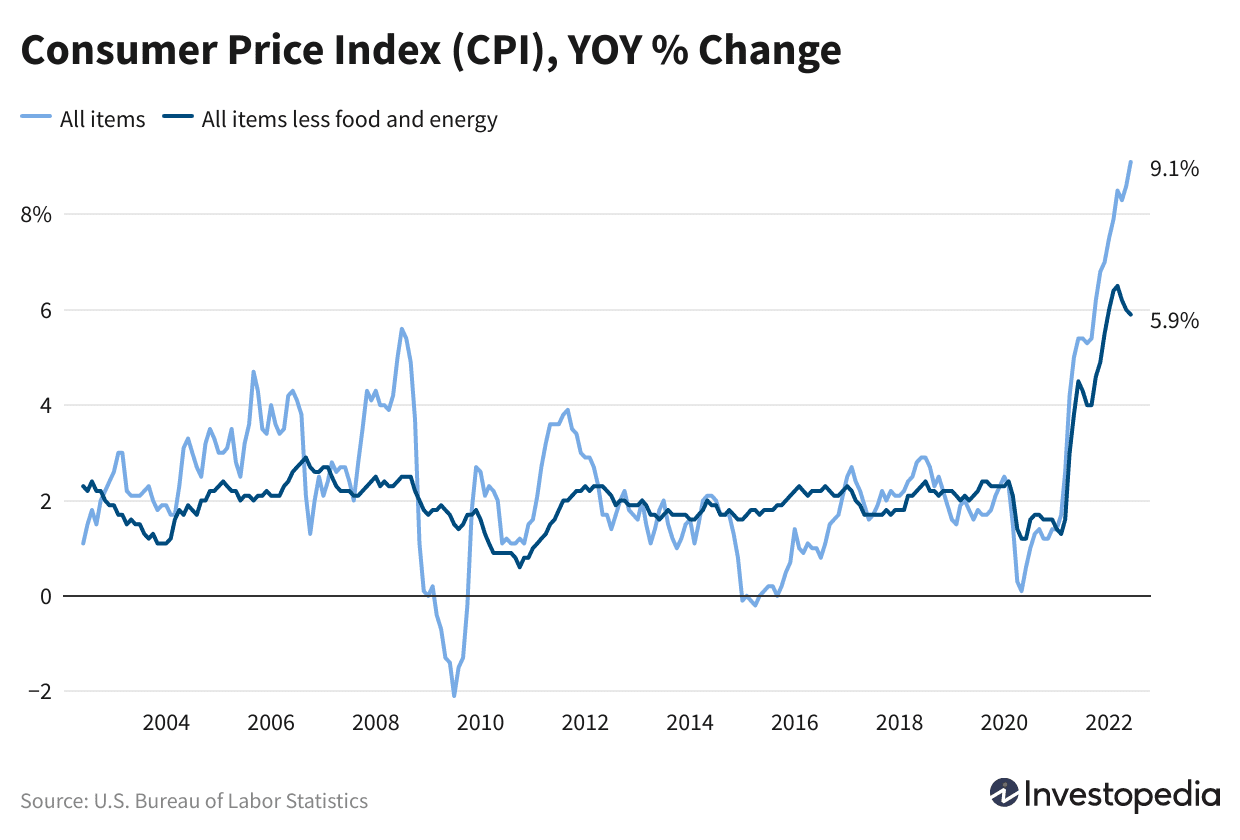
Consumer prices were unchanged in July, as plunging prices for gasoline dragged the Consumer Price Index down to zero. Core inflation, which excludes energy and food, rose only 0.3%, below what analysts expected.
Driving the news: The Labor Department reported that overall consumer prices rose 0% last month, and are up 8.5% over the past year. That compares to a 9.1% year-over-year reported in June.
Why it matters: Falling gasoline prices are clearly giving American consumers some inflation relief, and the broader inflation picture was more favorable in July than economists had expected.
By the numbers: Gasoline prices fell 7.7% in July, dragging down headline inflation. Other items with falling prices included used cars and trucks (-0.4%) and airfares (down 7.8%).
But rents kept rising, a major factor in stubbornly high underlying inflation. Renters faced a 0.7% rise in costs.
What’s next: The Federal Reserve has indicated it intends to keep raising interest rates until there is clear evidence inflation is waning. After two straight months of extremely hot inflation readings, this report will be welcome news.
Hiring is getting less challenging on some level, even amid a tight labor market, several employers said, according to The Wall Street Journal.
Take Nashville, Tenn.-based HCA Healthcare, for example.
In July, the hospital operator released its second-quarter earnings, and CEO Sam Hazen said turnover was down more than 20 percent in the second quarter compared to the first, The Wall Street Journal reported Aug. 8. Other large companies like Verizon, Uber and Marriott also indicated improvements in hiring or less turnover.
The decreased turnover comes as employers have faced workforce shortages during the COVID-19 pandemic. While employers continue to face challenges with shortages and hiring certain roles, some say the situation is improving to some degree, according to The Wall Street Journal.
Companies and economists cited multiple factors contributing to the trend, including some workers returning to their former employers, as well as inflationary pressures motivating workers to accept jobs more quickly or keeping workers in their existing jobs.
Overall, healthcare gained 69,600 jobs in July, an increase from the amount added in June, according to the latest jobs report from the U.S. Bureau of Labor Statistics. The July count compares to 56,700 jobs added in June and 28,300 jobs added in May.
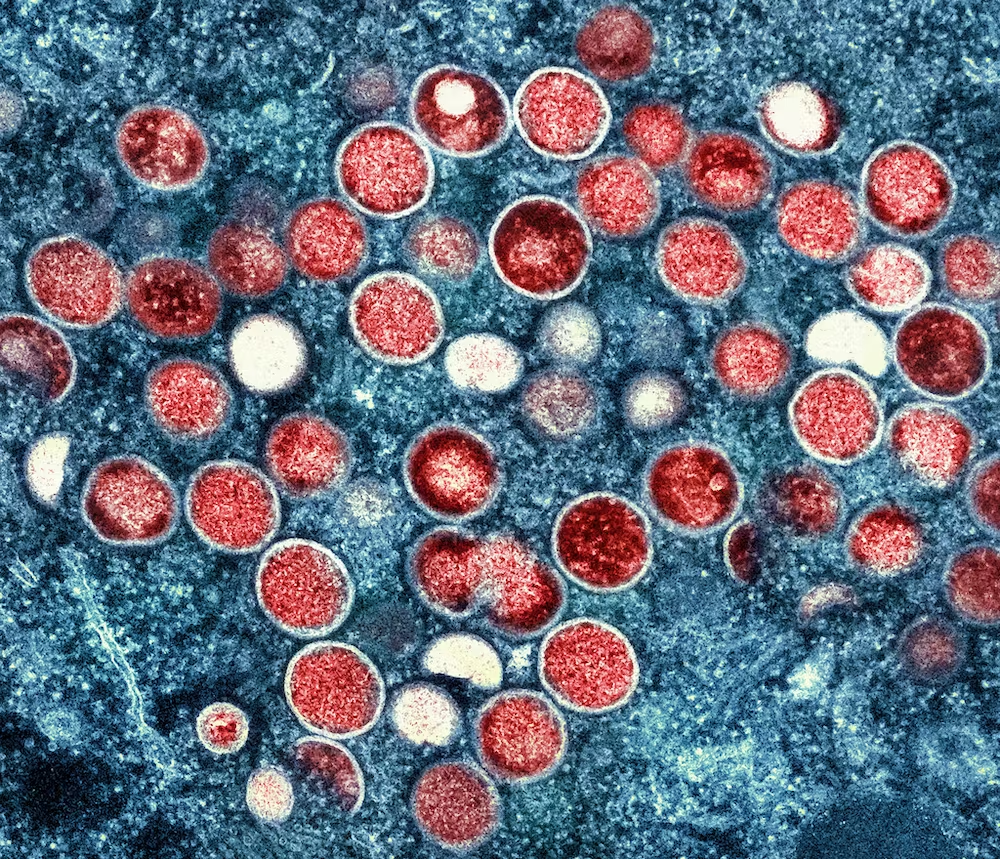
The monkeypox virus typically spreads through direct contact with respiratory secretions, such as mucus or saliva, or skin lesions. Skin lesions traditionally appear soon after infection as a rash – small pimples or round papules on the face, hands or genitalia. These lesions may also appear inside the mouth, eyes and other parts of the body that produce mucus. They can last for several weeks and be a source of virus before they are fully healed. Other symptoms usually include fever, swollen lymph nodes, fatigue and headache.
I am an epidemiologist who studies emerging infectious diseases that cause outbreaks, epidemics and pandemics. Understanding what’s currently known about how monkeypox is transmitted and ways to protect yourself and others from infection can help reduce the spread of the virus.
How is this outbreak different from prior ones?
The current monkeypox epidemic is a bit unusual in a few ways.
First, the sheer scope of the current epidemic, with over 25,000 cases worldwide as of early August and in countries where the virus has never appeared, sets it apart from previous outbreaks. Monkeypox is endemic to specific areas in central and western Africa, where cases occur sporadically and outbreaks are usually contained and quickly burn out. In the current outbreak, global spread has been rapid. Young men, mostly ages 18 to 44, account for the majority of cases, and over 97% identify as men who have sex with men (MSM). Some superspreading events associated with air travel, international gatherings and multiple-partner sexual encounters contributed to early transmission of the virus.
Second, the way symptoms are appearingmay facilitate spread among people who don’t yet know they are infected. Mostpatients reported mild symptoms without fever or swollen lymph nodes, symptoms that typically appear before a skin rash is visible. While most people do develop skin lesions, many reported having only a single papule that was often obscured inside a mucosal area, such as inside the mouth, throat or rectum, making it easier to miss.
A number of people reported no symptoms at all. Asymptomatic infections are more likely to go undiagnosed and unreported than those with symptoms. But it is not yet known how asymptomatic individuals may be contributing to spread or how many asymptomatic cases may be undetected so far.
Who is at risk of getting monkeypox?
For most people, the risk of getting monkeypox is currently low. Anyone who has prolonged, close contact with an infected person is at risk, including partners, parents, children or siblings, among others. The most common settings for transmission are within households or health care settings.
Because of sustained transmission within the community of men who have sex with men, they are considered an at-risk group, and targeted recommendations can help allocate resources and limit transmission. While monkeypox is spreading primarily among MSM, this does not mean that the virus will remain confined to this group or that it won’t jump to other social networks. The virus itself has no regard for age, gender, ethnicity or sexual orientation.
Anyone who comes into direct contact with the monkeypox virus is at risk of being infected.New cases are recorded daily, with additional countries and regions reporting their first cases and already affected countries observing a continued rise in infections.
As with most infections, other factors, such as the amount of viral exposure, type of contact and individual immune response, play a role in whether an infection takes hold.
Is monkeypox an STI?
While sexual encounters are currently the predominant mode of transmission among reported cases, monkeypox is not a sexually transmitted infection. STIs are spread primarily through sexual contact, while monkeypox can spread through any form of prolonged, close contact.
Close contact that transmits the monkeypox virus involves encounters that are typically more intimate or involved than having a casual conversation or standing next to someone in an elevator. Transmission requires exchange of mucosal fluids or direct contact with the virus in sufficient quantity to seed an infection. This could occur through physical contact during kissing or cuddling.
Because sexual encounters involve direct skin-to-skin physical contact where bodily fluids may be exchanged, these close encounters can transmit viruses more easily. Recently, monkeypox DNA has been detected in feces and various body fluids, including saliva, blood, semen and urine. But the presence of viral DNA does not necessarily mean that the virus can infect someone else. Transmission from these sources is still under investigation.
As the virus moves through populations, public health officials focus on getting the message out to the most at-risk and hardest hit communities about how to stay safe. Currently, breaking the transmission chain among sexual contacts is a priority, including but not limited to MSM communities. Targeted messaging is meant to protect the health of a specific group, not to stigmatize the intended audience.
Other modes of transmission may play a greater role outside the MSM community. Household transmission, where individuals may come into close contact with infected people or contaminated items, is one of the most common types of exposure. Research is ongoing into the potential airborne and respiratory droplet spread of monkeypox in the current situation.
Outbreaks are dynamic situations that evolve over time, which is why public health messages may change as the epidemic progresses. Not every outbreak looks or behaves the same way – even pathogens seen in previous outbreaks can be different the next time around. As researchers learn more about how the disease is transmitted and identify changes in patterns of spread, public health officials will provide updates about specific forms of contact, behaviors or other factors that could increase infection risk. While changing guidelines can be frustrating or confusing, keeping up to date with the latest recommendations can help you protect yourself and stay safe.
What do I do if I’ve been exposed to monkeypox?
Anyone who has been infected can help contain spread by isolating from others, including pets. Covering skin lesions, wearing a mask in shared spaces and decontaminating shared surfaces or items, such as bed linens, dishes, clothes or towels, can also reduce spread.
You can also help interrupt the transmission chain by participating in contact tracing, notifying public health officials of others who may have been exposed through you, which is a basic tenet and common practice of disease control.
All but two of the seven largest insurers saw profits climb in the second quarter as hospital operators continued to struggle with weak volumes and higher labor costs.
The nation’s top health insurers again raised financial targets for the year as revenues climbed on increased membership, while some signs indicated demand for medical services was tepid.
All but two of the seven largest insurers saw profits climb in the second quarter compared with the prior-year period, as many saw a key metric for medical spending decrease.
Many of the largest insurers saw profits climb in the second quarter
Industry observers have been closely watching for signals of pent-up demand as many patients delayed care amid the varying spikes in COVID-19 cases.
That didn’t seem to materialize in the second quarter as insurance executives didn’t report a surge in care. Almost all insurers saw their medical loss ratios either decline or remain the same from the second quarter last year.
Executives at Cigna, one of the nation’s largest insurers with nearly 18 million members, said there were fewer surgeries, fewer emergency room visits and fewer people admitted to the hospital in the second quarter compared to the prior-year period.
Direct COVID-19 costs were also better-than-expected, Cigna executives told investors on the second-quarter earnings call. As fewer Cigna patients sought medical care, net income climbed 6% to $1.6 billion.
Cigna wasn’t alone in reporting lighter patient volumes.
UnitedHealthcare, the insurer arm of UnitedHealth Group with more than 51 million members, reported a lower level of COVID-19 patient care and said usage of some medical services still fell below pre-pandemic levels, including pediatrics and the emergency department. UnitedHealth’s net income increased to $5.1 billion.
Q2 performances led insurers to raise their financial expectations for the full year.
“The lower utilization trends and lack of COVID-19 headwinds seen to date, give us confidence in raising our full year adjusted [earnings per share] guide,” Humana CFO Susan Diamond said on a call with investors.
On the other hand, the nation’s for-profit hospital chains reported fewer admissions and a dip in profits as they continued to deal with labor and other expenses amid record high inflation.
A New York federal judge on Wednesday dismissed a surgeon’s legal challenge that sought to roll back key pieces of a federal law that protects patients from surprise out-of-network bills.
Judge Ann Donnelly ruled against the surgeon, finding that the law is constitutional, and dismissed the case for lack of standing and dismissed the surgeon’s request for a preliminary injunction.
Katie Keith, a lawyer and health policy expert at Georgetown University who tracks surprise billing litigation, called the ruling good news for consumers.
The lawsuit threatened to once again expose millions of patients to surprise out-of-network bills, Keith previously said in a Health Affairs report on the litigation.
Daniel Haller, a surgeon, and his private practice filed suit in December against federal regulators alleging that the ban on surprise billing was unconstitutional along with the independent dispute resolution process, the way in which providers and payers are supposed to resolve payment disagreements.
Haller said the law deprives physicians the right to be paid a reasonable value for their services, according to the complaint.
Under the law, physicians and insurers can enter into an independent dispute resolution process to come to an agreement on the payment for services. The process was intended to keep patients out of the middle of these payment disputes.
Haller argued the process favored insurers — not providers.
However, a key part of that process was struck down by a Texas judge, who ruled in favor of providers in February.
Donnelly said Haller and his team did not show that they even went through the arbitration, or IDR, process, “much less that the IDR process resulted in a payment amount below the reasonable value,” according to Wednesday’s opinion.
“At the time of oral argument — almost six months after the Act went into effect — the plaintiffs could not say whether they had participated in the IDR process. They do not allege that the IDR process has caused any concrete harm, so their claims of constitutional injury are speculative,” Donnelly said.
Haller’s practice, Long Island Surgical, and its team of six physicians perform procedures on patients who are admitted after an emergency department visit.
Almost 80% of Long Island Surgical’s patients have an insurance plan that does not have a contractual relationship with the surgical group. In other words, Haller and his colleagues are almost always out-of-network, potentially putting patients at risk of a surprise medical bill.
The No Surprises Act tried to solve this problem, and it bans surprise billing in most cases.
The law aimed to tackle one of the most frustrating issues in healthcare, which could ensnare even savvy patients. Patients could be unknowingly treated by out-of-network providers, and then get bills their insurers refused to pay in full or part, leaving them stuck to pay the remaining balance.
With a 51-50 vote, Senate Democrats passed a sweeping $739 billion bill Aug. 7 that furthers some of the largest changes to healthcare in years.
Titled the Inflation Reduction Act, the bill touches energy, tax reform and healthcare. The House is expected to take it up Aug. 12, with Democrats aiming to approve it and send it to President Joe Biden’s desk.
Here are seven healthcare takeaways from the 755-page bill:
Drug pricing
1. For the first time, Medicare would be allowed to negotiate the price of prescription medicines with manufacturers. Negotiation powers will apply to the price of a limited number of drugs that incrementally increases over the next seven years. Ten drugs will be eligible for negotiations beginning in 2026; eligibility expands to 15 drugs in 2027 and 20 by 2029.
2. The HHS secretary will provide manufacturers of selected drugs with a written initial offer that contains HHS’ proposal for the maximum fair price of the drug and reasoning used to calculate that offer. Manufacturers will have 30 days to either accept HHS’ offer or propose a counteroffer.
3. Members of Medicare Part D prescription drug plan would see their out-of-pocket costs for prescription drugs capped at $2,000 per year, with the option to break that amount into monthly payments, beginning in 2025.
4. Democrats lost on a provision to place a $35 cap on insulin for Americans covered by private health plans. The provision to cap insulin at $35 dollars for Medicare enrollees passed by a of 57-43.
5. Drug companies will be required to rebate back price differences to Medicare if they raise prices higher than the rate of inflation, coined an “inflation rebate.”
6. The legislation makes all vaccines covered under Medicare Part D free to beneficiaries with no deductibles, co-insurance or cost-sharing, starting in 2023.
Tax subsidies
7. The legislation extends the Affordable Care Act’s federal health insurance subsidies, now set to expire at the end of the year, through 2025. Democrats say the extension will prevent an estimated 3.4 million Americans from losing health coverage.
Kaiser Permanente reported lower revenues in the second quarter of this year than in the same period a year earlier, and the Oakland, Calif.-based healthcare giant ended the period with a net loss.
Kaiser, which provides healthcare and health plans, reported operating revenue of $23.47 billion in the second quarter of 2022, down from $23.69 billion in the same quarter of 2021. The organization’s expenses climbed from $23.34 billion in the second quarter of last year to $23.38 billion in the same period this year.
“Much like the entire health care industry, we continue to address deferred care while navigating COVID-19 surges and associated expenses,” Kathy Lancaster, Kaiser executive vice president and CFO, said in an Aug. 5 earnings release. “Kaiser Permanente’s integrated model of providing both care and coverage enables us to meet these challenges as demonstrated by our moderate increase in year-over-year operating expenses for the second quarter.”
Kaiser ended the second quarter of this year with operating income of $89 million, down from $349 million a year earlier.
After factoring in a nonoperating loss of $1.4 billion, Kaiser reported a net loss of $1.3 billion for the second quarter of this year, compared to net income of $2.97 billion in the same period last year. Kaiser said the loss was largely attributable to market conditions.
This is the second quarter in a row that Kaiser has reported a loss. The organization closed out the first quarter of this year with a net loss of $961 million, compared to net income of $2 billion in the same quarter of 2021.
As RNs struggle to work through staffing shortages, their job satisfaction has sharply declined, with 67% saying they plan to leave their jobs within the next few years, according to a survey from the American Association of Critical-Care Nurses (AACN) published in Critical Care Nurse.
RNs cite poor work environments
For the survey, AACN collected responses from 9,862 nurses, 9,335 of which met the study criteria of being currently practicing RNs, in October 2021. The mean age was 46.5 years, and the mean years of experience was 17.8 years.
Of the participants, 78.3% worked in direct care, and 19.4% worked in a Beacon unit, meaning that their unit had been recognized by an AACN Beacon Award for Excellence. Half of the participants said they spent 50% or less of their time caring for Covid-19 patients, while the other half said they spent 50% or more.
To measure the health of a work environment, AACN looked at six standards:
Skilled communication
True collaboration
Effective decision-making
Meaningful recognition
Authentic leadership
Appropriate staffing
Overall, AACN found that nurses’ perceptions of quality on these six measures had declined across the board since the organization’s 2018 survey.
In particular, appropriate staffing was the lowest rated of all the standards at 2.33 out of 4, which is the lowest rating the standard has received since AACN first began the survey in 2006. Only 24% of RNs said their units had the right number of nurses with the right knowledge and skills more than 75% of the time—down from 39% who said the same in 2018.
In addition, there was a significant decline in how RNs rated the quality of care in their organizations and their units. Only 16% rated their organizations’ quality of care as excellent (compared to 24% in 2018), and 30% rated their units’ quality of care as excellent (compared to 44% in 2018). Over 50% of nurses said quality of care in their organization or unit has gotten somewhat or much worse over the last year.
Many nurses also reported difficulties with their physical and psychological well-being in the survey. For example, less than 50% of RNs said they felt their organization values their health and safety, a significant decline from 68% who said the same in 2018.
In addition, 40% of participants reported that they were not emotionally healthy. The percentage of RNs who reported experiencing moral distress also doubled from 11% in 2018 to 22% in 2021.
A significant portion of RNs also reported experiencing verbal abuse, physical abuse, sexual harassment, or discrimination over the past year. Of the 7,399 RNs who answered this question, 72% said they had experienced at least one negative incident, with verbal abuse being the most common at 65%, followed by physical abuse at 28%.
RN job satisfaction
Only 40% of RNs said they were “very satisfied” with their job, down from 62% who said the same in 2018. Further, a significant number of RNs in the survey reported planning to leave their jobs within the next few years.
Overall, 67% of RNs said they planned to leave their current position within the next three years, compared to 54% in 2018. Of this group, 36% said they planned to leave within the next year, with 20% planning to leave within the next six months.
According to the respondents, the top factors that could lead them to reconsider their decision to leave their job were a higher salary and more benefits (63%), better staffing (57%), and more respect from administration (50%).
“Without improvements in the work environment, the results of this study indicate that nurses will continue to exit the workforce in search of more meaningful, rewarding, and sustainable work,” the survey’s authors wrote. “It is time for bold action, and this study shows the way.” (Firth, MedPage Today, 8/3; Ulrich et al., Critical Care Nurse, 8/1)
Hard truths on the current and future state of the nursing workforce
Concerns about an imbalance in supply and demand in the nursing workforce have been around for years. The number of nursing professionals nationally may be healthy, but many nurses are not in the local areas, sites of care, or roles where they’re needed most. And many of today’s nurses don’t have the specialized skills they need, widening the existing gap between nurse experience and job complexity.
As a result, gaping holes in staffing rosters, prolonged vacancies, unstable turnover rates, and unchecked use of premium labor are now common.
Health care leaders need to confront today’s challenges in the nursing workforce differently than past cyclical shortages. In this report, we present six hard truths about the nursing workforce. Then, we detail tactics for how leaders can successfully address these challenges—stabilizing the nursing workforce in the short term and preparing it for the future.









{kind=link}