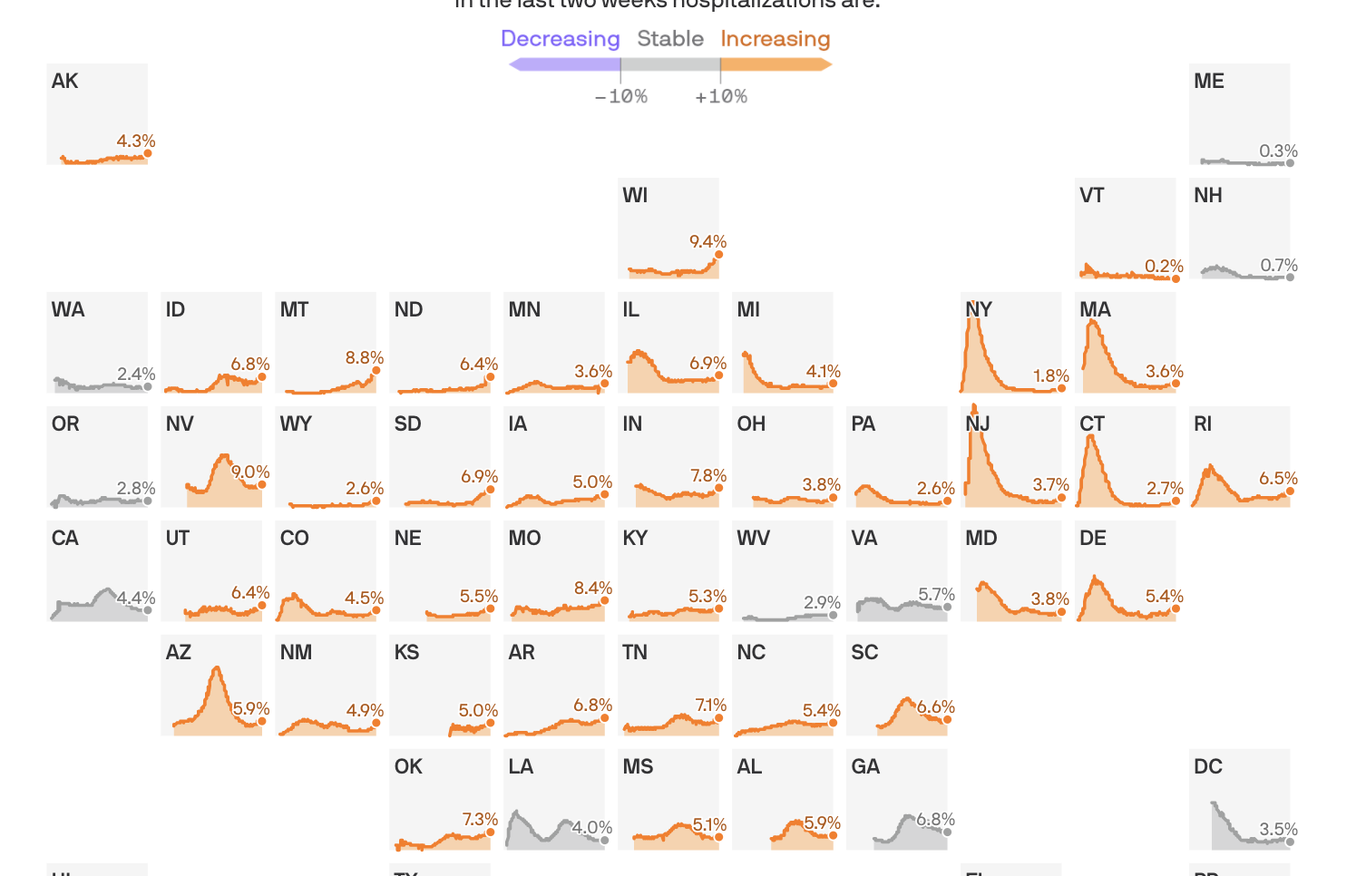
Share of hospital beds occupied by COVID-19 hospitalizations
States shown from first date of reported data, from March 17 to Oct. 17, 2020
In the last two weeks hospitalizations are:
Coronavirus hospitalizations are increasing in 39 states, and are at or near their all-time peak in 16.
The big picture: No state is anywhere near the worst-case situation of not having enough capacity to handle its COVID-19 outbreak. But rising hospitalization rates are a sign that things are getting worse, at a dangerous time, and a reminder that this virus can do serious harm.
By the numbers: 39 states saw an increase over the past two weeks in the percentage of available hospital beds occupied by coronavirus patients.
Wisconsin is faring the worst, with 9.4% of the state’s beds occupied by COVID patients.
Sixteen states are at or near the highest hospitalization rates they’ve seen at any point in the pandemic.
Yes, but: The all-time peak of coronavirus hospitalizations happened in the spring, when 40% of New Jersey’s beds were occupied by COVID patients. Thankfully, even the the worst-performing states today are still a far cry from that.
Between the lines:These numbers, combined with the nationwide surge in new infections, confirm that the pandemic in the U.S. is getting worse — just as cold weather begins to set in in some parts of the country, which experts have long seen as a potentially dangerous inflection point.
They also suggest that most parts of the country won’t need to pause or scale back non-coronavirus treatments, as hospitals did in the spring when no one was quite sure how bad things could get.
In rural areas, however, even a modestly sized outbreak can strain local hospital capacity.
As a new wave of coronavirus cases hits the U.S. and Europe, governments are shifting away from total shutdowns toward more geographically targeted lockdowns to stifle the virus’ spread.
Why it matters:Precision shutdowns can slow emerging outbreaks while lessening the overall economic impact of the response. But they risk a backlash from those who are targeted, and may not be strong enough to keep a highly contagious virus under control.
Driving the news: New York City tried to control a flare-up of new coronavirus cases this month by instituting partial shutdowns on a neighborhood-by-neighborhood basis, curtailing economic and social activity in areas harder hit by the virus while continuing reopening elsewhere.
British Prime Minister Boris Johnson on Monday instituted a similar response for the U.K., putting in place a three-tier escalating system of lockdowns on a city or regional basis.
“We don’t want to go back to another national lockdown,” Johnson told the British Parliament. But “we can’t let the virus rip.”
What’s new: Some early research indicates more-targeted lockdowns can effectively smother outbreaks while leaving broader city and regional economies mostly intact.
A paper published by a team of economists in July found a more precise shutdown focused on places where viral spread was most common could have reduced economic losses in New York by as much as 50% compared to a uniform lockdown.
As long as new outbreaks are still in the relatively low flare-up stage, targeted lockdowns can efficiently cut off the oxygen to new spread. That seems to be the case in New York, where data released on Thursday indicates transmission has slowed in six of the ZIP codes that had been the focus of targeted lockdowns.
Yes, but: Individuals move around a city, and some epidemiologists worry that over time cases will break out of targeted lockdown areas and spark a wider outbreak.
A preprint paper published in August found people were willing to travel outside of lockdown areas to get services they needed, potentially spreading the virus along the way.
That was especially true for religious services. The paper found that during March, even as the total number of visits to churches declined, between 10% and 30% of churches nationwide saw increases in attendance. Those who were motivated to go simply went to churches outside of restricted areas.
The small, seemingly geographically isolated outbreaks officials are focusing on may actually be the first signs that a city or region’s control measures simply aren’t working. As a result, “targeted measures can end up chasing the outbreak wider and wider, to the point where restrictions are equivalent to a broader blanket policy,” epidemiologist Adam Kucharski told Wired.
What to watch:A targeted lockdown is inevitably going to appear to single out specific groups of people, which risks creating a backlash that can undermine public support for long-term control measures.
That’s already been the case in New York, where Orthodox Jewish communities have taken to the street to protest targeted lockdowns in their neighborhoods.
In New York’s Queens borough, stores and restaurants in one mall have been ordered closed, while those in an adjacent mall are still open, simply because of which side of the line they fall on.
The experience of COVID-19 has already been a deeply unfair one, with both the direct health effects and indirect economic costs falling on those who can least afford it, and focused lockdowns will exacerbate that unfairness.
The bottom line:Targeted lockdowns can throttle the virus while minimizing economic damage, at least in the short term. But one thing we’ve learned is that if COVID-19 gets out of control in one place, it may be only a matter of time before it ends up everywhere else.
Dueling petitions about what to do about COVID19 — the Great Barrington Declaration and the John Snow Memorandum — are circulating online amongst physicians, public policy makers, and academics. I am not against policy statements, consensus building, or even petitions, but both of these documents trouble me. They are the dropping anchors when we should be open to sailing where the wind blows.
Let’s start with the obvious. SARS-CoV-2 kills people. When infected, older people and those with serious comorbidities are more likely to die than younger people. This age-gradient (extra risk of death among older people) is steep. At the same time, dramatic interventions to halt SARS-CoV-2 — such as closing schools, business, travel, economic activity, normal hospital functions — also kills people. Some of these deaths occur immediately — a person with a heart attack is dissuaded from seeking care, an uncontrolled tuberculosis epidemic in a low income nation, or even depression and suicide — and some of the downsides take a long time to kill: loss of upward mobility and economic potential for the next generation will shorten lives.
Downsides to lockdowns can also be hard to predict. Harms may include destabilizing democratic governments, civil unrest, and political turmoil. The goal of policy in each and every place on earth is to minimize the total harm to the people who live there. It may vary by place and even moment based on viral spread, age of population, safety nets (or lack there-of), and a number of other factors, including values and preferences.
First, consider the Great Barrington Declaration. It’s just 540 words long, and outlines a strategy of focused protection. Based on the idea that the risk of death varies dramatically with age, it proposes we shield and protect the vulnerable while allowing the young, and others at lower risk, to get on with life as normally as possible. It offers some ideas about how to guard nursing homes, which have experienced massive causalities, and endorses simple measures like handwashing. It nods to the idea that the herd immunity threshold (fraction of people in a population who have become immune before viral spread abates) is not a fixed value: it depends on the way in which populations mix and interact and on simple measures we choose to take, such as improved hygiene. It recommends that schools, universities, bars, and restaurants be allowed to open fully.
Limitations to the statement are its lack of guidance as to who exactly the vulnerable are, how they should shield themselves, and the fact that it lumps together very different things — such as bars and schools. Open bars can be replaced with drinking beers in the backyard with a friend seated at a distance with little loss of pleasure, but education, particularly for the poor, is one of the few ladders left in American society for a better life, a place to feed children, and a vehicle for detecting abuse. Another limitation is its lack of acknowledgement that in moments of explosive spread, temporary measures likely need to be taken to prevent, for example, hospitals from overflowing. Surely, policy responses must depend on the specifics of the time and place.
The John Snow Memorandum was filed in response. It’s longer, at 930 words. It calls Great Barrington’s suggestions to achieve immunity through naturally occurring infections a “dangerous fallacy unsupported by scientific evidence.” Instead it advocates for continued restrictions, along with social programs to minimize the harms of these restrictions. Signers believe this would lower viral spread to very low levels where contact tracing can be utilized to eliminate outbreaks. Finally, the strategy ends when we have an effective vaccine, which it predicts will occur in the coming months.
Limitations to the Snow memorandum include: How exactly will one create social programs to minimize the harms, and what exactly will those programs look like? What will you do in places like the U.S. where even basic economic stimulus talks have stalled? Millions of people are entering poverty in this country, and many more may face starvation globally. How precisely and quickly will you help them? Those who criticize the Barrington authors for not providing a plan to protect the vulnerable from the virus, must criticize the Snow authors for not explaining how they will shield the vulnerable from the harms of restrictions. Additionally, calling for contact tracing is easy, but practically, this faces severe limitations in a nation like the U.S. when many individuals contacted are reluctant to share information. Here too the Snow memorandum falls short on specifics.
The declaration and memorandum are both online and taking signatures, but is this how complex policy should be decided? I find the idea that the fate of the globe will hinge on who garners the most signatures to be Kafkaesque.
Worse, the dueling petitions further divide us, when we should be talking together and working together. It does not escape me that many forces seek to tie these petitions to the Republican and Democratic parties — a dangerous but growing movement to equate pandemic policy with politics.
Signing these petitions may already be a form of identity or virtue signaling, letting others in our political circles know that we are on the virtuous team. Moreover, having signed them, we may be less likely to be willing to change our mind: To think one moment “we ought to open universities,” and the next moment, “let’s consider alternative policies, if hospitalizations rise.”
Instead of these divisive petitions, surely there are things we can all agree to. There is a hierarchy of importance to activities and events in life. Bars, strip clubs, conferences for work — fall on the low end. Schools for young kids, particularly public schools in poor or minority communities, and hospitals are among the most important. There are simple interventions that we can test in controlled trials and implement in the meantime, such as face-shields, plexiglass barriers, widespread hand sanitizer, and masks. We must prioritize schools over bars, and policy must remain individualized (to specific nation/state/county and local preferences) and fluid — able to scale up and down, as we balance the harms of the virus with the harms of closure.
Finally, we have to separate rules from behavior. You can allow restaurants to open, but it won’t help the economy if no one eats there. And, you can close everything, but you won’t slow the spread if people have backyard barbecues with dozens of people. What are the best ways to encourage desired behavior? That’s a harder problem.
Finally, there is no one-size-fits-all solution. What works in a remote island nation with a strong safety net, that can cut off contact with the rest of the world, may not work in a nation with hundreds of millions who face the threat of starvation if the economy grinds to a halt.
We need fewer pompously named petitions and instead, a COVID policy response that engages with people who hold views and perspectives different than our own; which acknowledges the lives lost from the virus and lost through the response; which is nimble and responsive to new data, new facts, and new perspectives; which engages values and preferences and local norms and the messy reality of the world as it is, not as we wish it were.
And, almost most importantly, one which is bipartisan, spanning political ideology, which unites rather than divides us.
The number of new unemployment claims jumped last week, the latest sign of the toll the coronavirus pandemic continues to take on the economy.
States across the country processed 898,000 new unemployment claims, up more than 50,000 from the previous week, the largest increase in first-time jobless applications since August.
These numbers marked another unfortunate milestone: The number of unemployment claims has been above the pre-pandemic one-week record of 695,000 for 30 weeks now.
Claims for Pandemic Unemployment Assistance, for gig and self-employed workers, went down, to 373,000 from about 460,000.
And the total number of people on all unemployment programs dropped slightly, to 25.3 million for the last week of September, down from 25.5 million the previous week.
The number of new claims has fallen greatly from its peak in the spring, but economists say they are concerned that the number remains so high.
“No question this report casts doubt on the recovery,” said Andrew Chamberlain, the chief economist at Glassdoor. “This is a sign covid is still dealing heavy blows to the labor market. We’re nowhere near having the virus under control.”
The news comes amid a string of poor economic news, with headlines punctuated with reports of large companies announcing layoffs in recent weeks.
These companies include Disney, insurance company Allstate, American and United Airlines, Aetna, and Chevron.
“It’s not coming down quickly,” said Julia Pollak, a labor economist at the jobs site ZipRecruiter. “It’s unclear how quickly we can recover. We’re likely to see additional layoffs and high numbers of unemployment for the foreseeable future.”
Pollak said there are indications that consumer spending has fallen since the expiration of government aid programs — another warning sign about more economic trouble ahead.
Many economists, including those at the Federal Reserve, have urged Congress and the White House to pass a new package of aid. House Democrats passed a $2.2 trillion plan earlier this month that Republicans have declined to advance, while Treasury Secretary Steven Mnuchin has been pushing a $1.8 trillion plan.
Still, there are signs that Senate Republicans would not be willing to accept that plan, either. Senate Majority Leader Mitch McConnell told reporters that he would not bring the plan to the floor, saying Senate Republicans believed the deal should top out at $1.5 trillion.
One sign of the severity of the economic crisis is the growing number of people who are transitioning to Pandemic Emergency unemployment compensation — for those who hit the maximum number of time that their state plans allow for. That number grew 818,000, according to the most recent figures, from the end of September.
Questions remain about the integrity of the data, as well.
A number of issues have complicated a straightforward read of the weekly release, such as issues with fraud, which are believed to have driven up these numbers an unknown amount, and backlogs in states like California. The country’s largest state typically accounts for about 20-28 percent of the country’s total weekly claims, but has put its claims processing on hold temporarily.
Instead, the Department of Labor is using a placeholder number for the state — 226,000, the number of new initial claims in the state from mid-September.
But some economists like Chamberlain are critical of this method.
“The idea of cutting and pasting the data from a state is so absurd,” he said. “They could at least use a model. But instead they’re carrying over the number. It’s quite a crisis.”
Quirks in the new filing process require people to apply for traditional unemployment and get rejected before applying for PUA — a source of potential duplicate claims.
Economists have been warning for months that the unemployment rate, which has improved steadily since its nadir in April, is at risk of getting worse without further government intervention.
States that saw significant jumps in unemployment claims last week include Indiana, Alaska, Arizona, Illinois, New Mexico and Washington.
Still, some economists have found reasons to hope. Pollak said job postings on ZipRecruiter have topped 10 million for the first time since the start of the pandemic, equaling a number last seen in January.
The jobs are different now, she said — fewer tech and business jobs and more warehousing jobs, temporary opportunities and contracting work.
Dr. Anthony Fauci, the nation’s top infectious disease expert, tells CBS Evening News anchor and managing editor Norah O’Donnell that Americans need to “double down” on mask-wearing and social distancing to help control a surge in new coronavirus cases.
He also spoke about President Trump’s recovery from COVID-19, progress towards a vaccine, and how the pandemic will affect this year’s holiday gatherings. Watch the full interview.
Dr. Anthony Fauci on Thursday denounced the concept of herd immunity — the notion that if a large enough group of people contract an infection, it will ultimately stop the disease from spreading — calling it “nonsense” during an interview with Yahoo News.
“Anybody who knows anything about epidemiology will tell you that is nonsense and very dangerous,” Fauci said, “because what will happen is that if you do that, by the time you get to herd immunity, you will have killed a lot of people that would have been avoidable.”
Fauci, the director of the National Institute of Allergy and Infectious Diseases and member of the White House coronavirus task force, discussed the coronavirus pandemic and the country’s response to it during a live interview Thursday morning with Yahoo News Editor in Chief Daniel Klaidman and Chief Investigative Correspondent Michael Isikoff.
The coronavirus has killed more than 216,000 people in the U.S. and infected almost 8 million, according to data from Johns Hopkins University.
Now, more than seven months after the coronavirus was declared a pandemic, Fauci said Thursday that the U.S. is not in a good place.
“We talk about a second wave,” he said. “We’ve never really gotten out of the first wave. If you look at the baseline number of daily infections that we have had over the last several weeks, [it’s] been around 40,000 per day. It’s now gone up to about 50,000 per day. So right away, we have a very unfortunate baseline from which we need to deal.”
President Trump and his administration have been pushing the herd immunity approach as a possible solution to ending the pandemic, the New York Times reported Wednesday. During a call with reporters, two officials who requested anonymity cited a petition called the Great Barrington Declaration, which calls for states to lift coronavirus restrictions for the bulk of American citizens, the Times reported.
When asked about the herd immunity approach, Fauci said that while he agrees with what the declaration says about protecting the vulnerable and not closing down the country, virtually anyone with a solid understanding of epidemiology would disagree with the idea of letting everyone get infected.
“My position is known. Dr. Deborah Birx’s position is known, and Dr. [Robert] Redfield,” he said. “So you have me as the director of the National Institute of Allergy and Infectious Diseases, Debbie Birx, as the coordinator and a very experienced infectious disease person, the coordinator of the task force — and you have Bob Redfield, who’s the director of the [Centers for Disease Control and Prevention]. All three of us very clearly are against that.”
The White House is reportedly embracing a herd-immunity approach focused on “protecting the elderly and the vulnerable” but experts are calling the plan dangerous, “unethical”, and equivalent to “mass murder”.
“Current lockdown policies are producing devastating effects on short and long-term public health,” the declaration states, adding, “The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk. We call this Focused Protection.”
Essentially, herd immunity is when enough people are immune to a disease, like Covid-19, that the disease can’t be transmitted as easily and thus provides indirect protection.
It’s been rumoured that the government has been leaning towards this plan of action for some time now, although this is the first real admission.
In response to today’s news, experts around the world have been voicing their concerns.
And this isn’t the first time we’ve heard experts say herd immunity is not a good idea.
For example, the head of the World Health Organization said Monday that allowing the novel coronavirus to spread in an attempt to reach herd immunity was “simply unethical.”
Similarly, the National Institutes of Health (NIH) director Francis Collins also denounced herd immunity as a viable plan.
“What I worry about with this is it’s being presented as if it’s a major alternative view that’s held by large numbers of experts in the scientific community. That is not true. This is a fringe component of epidemiology. This is not mainstream science. It fits into the political views of certain parts of our confused political establishment,” he said in an interview.
Not to mention studies continue to show that Sweden’s attempts at herd immunity have failed and have resulted in a higher Covid-19 death toll than expected.
As more research comes out, scientists are starting to learn that Covid-19 immunity, even in those who were severely infected, can fade after a few weeks.
This is why we’ve seen cases of reinfection and why many experts are advising against a herd immunity plan.
To put that into context, that means around 197 million people would need to be infected in America. And assuming that the Covid-19 fatality rate is somewhere between 0.5% and 1%, based on numbers from the World Health Organization (WHO), more than 1 million people would die – at minimum.
William Haseltine, Chair and President of ACCESS Health International, told CNN “herd immunity is another word for mass murder. We are looking at two to six million Americans dead – not just this year but every year.”
“This is an unmitigated disaster for our country – to have people at the highest levels of our government countermanding our best public health officials. We know this epidemic can be put under control. Other countries have done it. We are doing the opposite.”
Government spending on testing and contact tracing pays for itself more than 30 times over, according to yet another paper published in JAMA (good series!).
What they found: Harvard economists David Cutler and Lawrence Summers calculated the total cost of the coronavirus pandemic at more than $16 trillion in the U.S. alone. Of that, about $7 trillion is attributable to loss of life and long-term impairment from the disease, Axios’ Felix Salmon writes.
Enhanced testing and tracing would cost about $6 million per 100,000 inhabitants, they calculate. Out of that population, 14 lives would be saved, on which they place a value of $96 million, and 33 critical and severe cases would be avoided, representing savings of $80 million.
That adds up to $176 million in benefits from $6 million in costs — before taking into account any second-order effects from even fewer cases down the road.
The bottom line: “Currently, the U.S. prioritizes spending on acute treatment,” write Cutler and Summers, “with far less spending on public health services and infrastructure.”
Going forward, they write, “a minimum of 5% of any COVID economic relief intervention should be devoted to such health measures.”
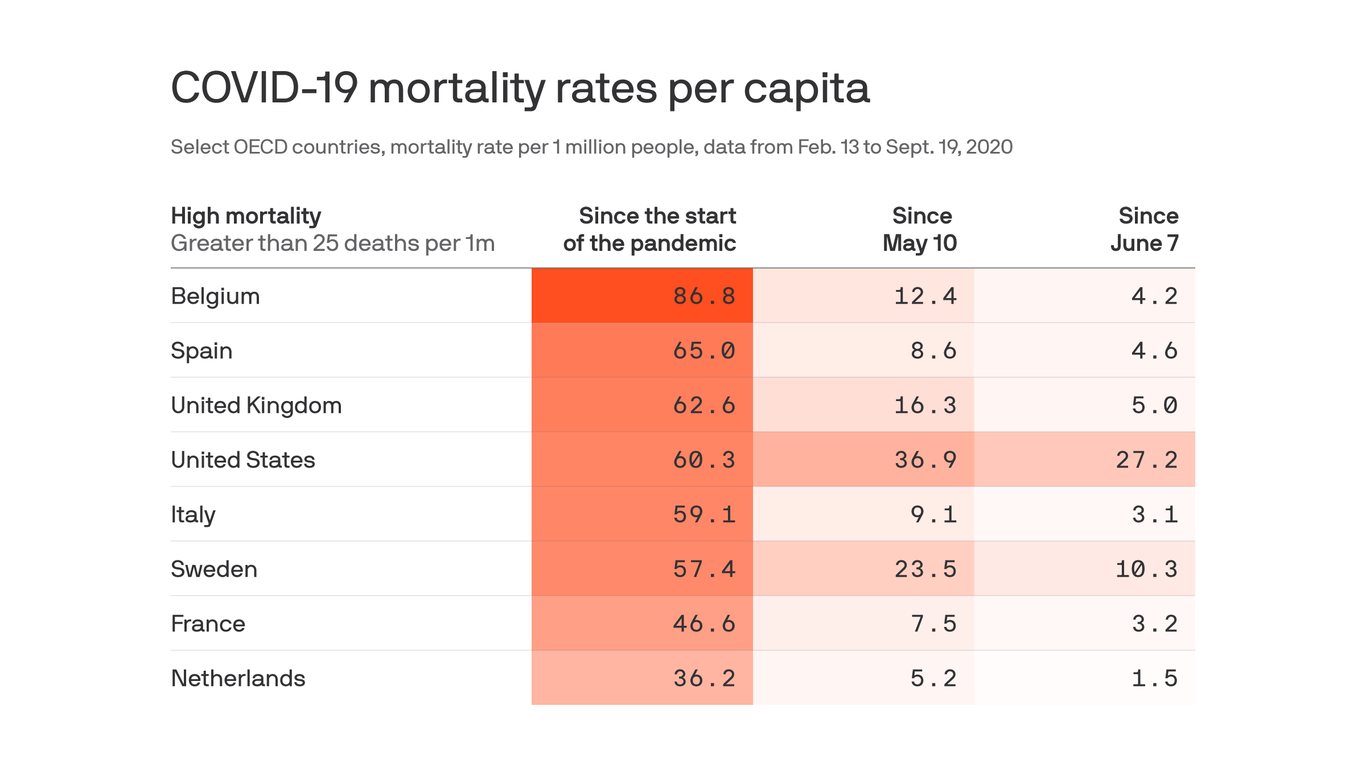
Although other wealthy countries have higher overall coronavirus mortality rates than the United States, the U.S. death rate since May is unrivaled among its peers, according to a new study published in JAMA.
Between the lines:After the first brutal wave of outbreaks, other countries did much better than the U.S. at learning from their mistakes and preventing more of their population from dying.
Why it matters:“If the U.S. had comparable death rates with most high-mortality countries beginning May 10, it would have had 44,210 to 104,177 fewer deaths,” the authors conclude.
Excess deaths have followed a similar pattern: The hardest-hit European countries had similar or higher rates of excess deaths of all causes to the U.S. early on, but these fell much lower than the America did after the first wave.
Yes, but: Death rates are not static, as this study proves, and outbreaks in several European countries have taken a turn for the worse lately.