

The billionaire philanthropist predicted the pandemic several years ago. Now, he shares his views on the current situation.
In this TED talks interview, philanthropist billionaire Bill Gates discusses his expert views on COVID-19. He shares why he predicted a few years ago that a global pandemic would hit the world.
Gates explains that the real danger in COVID- 19 is that it is infectious before symptoms have started. He calls these types of viruses worst-case scenarios.
“Ebola, you’re actually flat on your back before you’re very infectious so you’re not at church or on a bus or at a store. With most respiratory viruses like the flu at first, you only feel a little bit of a fever and a little bit sick. So there’s the possibility you’re going about your normal activities and infecting other people. Human to human transmissible respiratory viruses that in the early stage aren’t stopping you from doing things, that’s kind of a worst-case,” says the Microsoft co-founder.
He goes on to say that people move around more now, making for more worldwide victims. Gates also says that he understood the virus would be very difficult to contain back in January when he heard that it was human to human transmissible.
Finally, the entrepreneur shares what was happening behind the scenes during that period. The interview is a must-see not only for Bill Gates fans but for everyone who is concerned about COVID-19.
/posttv-thumbnails-prod.s3.amazonaws.com/03-24-2020/t_8a8c5e491d224704beec957580f758f3_name_032420_AmericanDoctors_Thumb_v02.png)
The conversations are driven by the realization that the risk to staff amid dwindling stores of protective equipment — such as masks, gowns and gloves — may be too great to justify the conventional response when a patient “codes,” and their heart or breathing stops.
Northwestern Memorial Hospital in Chicago has been discussing a do-not-resuscitate policy for infected patients, regardless of the wishes of the patient or their family members — a wrenching decision to prioritize the lives of the many over the one.
Richard Wunderink, one of Northwestern’s intensive-care medical directors, said hospital administrators would have to ask Illinois Gov. J.B. Pritzker for help in clarifying state law and whether it permits the policy shift.
“It’s a major concern for everyone,” he said. “This is something about which we have had lots of communication with families, and I think they are very aware of the grave circumstances.”
Officials at George Washington University Hospital in the District say they have had similar conversations, but for now will continue to resuscitate covid-19 patients using modified procedures, such as putting plastic sheeting over the patient to create a barrier. The University of Washington Medical Center in Seattle, one of the country’s major hot spots for infections, is dealing with the problem by severely limiting the number of responders to a contagious patient in cardiac or respiratory arrest.
Several large hospital systems — Atrium Health in the Carolinas, Geisinger in Pennsylvania and regional Kaiser Permanente networks — are looking at guidelines that would allow doctors to override the wishes of the coronavirus patient or family members on a case-by-case basis due to the risk to doctors and nurses, or a shortage of protective equipment, say ethicists and doctors involved in those conversations. But they would stop short of imposing a do-not-resuscitate order on every coronavirus patient. The companies declined to comment.
Lewis Kaplan, president of the Society of Critical Care Medicine and a University of Pennsylvania surgeon, described how colleagues at different institutions are sharing draft policies to address their changed reality.
“We are now on crisis footing,” he said. “What you take as first-come, first-served, no-holds-barred, everything-that-is-available-should-be-applied medicine is not where we are. We are now facing some difficult choices in how we apply medical resources — including staff.”
The new protocols are part of a larger rationing of lifesaving procedures and equipment — including ventilators — that is quickly becoming a reality here as in other parts of the world battling the virus. The concerns are not just about health-care workers getting sick but also about them potentially carrying the virus to other patients in the hospital.
R. Alta Charo, a University of Wisconsin-Madison bioethicist, said that while the idea of withholding treatments may be unsettling, especially in a country as wealthy as ours, it is pragmatic. “It doesn’t help anybody if our doctors and nurses are felled by this virus and not able to care for us,” she said. “The code process is one that puts them at an enhanced risk.”
Wunderink said all of the most critically ill patients in the 12 days since they had their first coronavirus case have experienced steady declines rather than a sudden crash. That allowed medical staff to talk with families about the risk to workers and how having to put on protective gear delays a response and decreases the chance of saving someone’s life.
A consequence of those conversations, he said, is that many family members are making the difficult choice to sign do-not-resuscitate orders.
Health-care providers are bound by oath — and in some states, by law — to do everything they can within the bounds of modern technology to save a patient’s life, absent an order, such as a DNR, to do otherwise. But as cases mount amid a national shortage of personal protective equipment, or PPE, hospitals are beginning to implement emergency measures that will either minimize, modify or completely stop the use of certain procedures on patients with covid-19.
Some of the most anxiety-provoking minutes in a health-care worker’s day involve participating in procedures that send virus-laced droplets from a patient’s airways all over the room.
These include endoscopies, bronchoscopies and other procedures in which tubes or cameras are sent down the throat and are routine in ICUs to look for bleeds or examine the inside of the lungs.
Changing or eliminating those protocols is likely to decrease some patients’ chances for survival. But hospital administrators and doctors say the measures are necessary to save the most lives.
The most extreme of these situations is when a patient, in hospital lingo, “codes.”
When a code blue alarm is activated, it signals that a patient has gone into cardiopulmonary arrest and typically all available personnel — usually somewhere around eight but sometimes as many as 30 people — rush into the room to begin live-saving procedures without which the person would almost certainly perish.
“It’s extremely dangerous in terms of infection risk because it involves multiple bodily fluids,” explained one ICU physician in the Midwest, who did not want her name used because she was not authorized to speak by her hospital.
Fred Wyese, an ICU nurse in Muskegon, Mich., describes it like a storm:
A team of nurses and doctors, trading off every two minutes, begin the chest compressions that are part of cardiopulmonary resuscitation or CPR. Someone punctures the neck and arms to access blood vessels to put in new intravenous lines. Someone else grabs a “crash cart” stocked with a variety of lifesaving medications and equipment ranging from epinephrine injectors to a defibrillator to restart the heart.
As soon as possible, a breathing tube will be placed down the throat and the person will be hooked up to a mechanical ventilator. Even in the best of times, a patient who is coding presents an ethical maze; there’s often no clear cut answer for when there’s still hope and when it’s too late.
In the process, heaps of protective equipment is used — often many dozens of gloves, gowns, masks, and more.
Bruno Petinaux, chief medical officer at George Washington University Hospital, said the hospital has had a lot of discussion about how — and whether — to resuscitate covid-19 patients who are coding.
“From a safety perspective you can make the argument that the safest thing is to do nothing,” he said. “I don’t believe that is necessarily the right approach. So we have decided not to go in that direction. What we are doing is what can be done safely.”
However, he said, the decision comes down to a hospital’s resources and “every hospital has to assess and evaluate for themselves.” It’s still early in the outbreak in the Washington area, and GW still has sufficient equipment and manpower. Petinaux said he cannot rule out a change in protocol if things get worse.
GW’s procedure for responding to coronavirus patients who are coding includes using a machine called a Lucas device, which looks like a bumper, to deliver chest compressions. But the hospital has only two. If the Lucas devices are not readily accessible, doctors and nurses have been told to drape plastic sheeting — the 7-mil kind available at Home Depot or Lowe’s — over the patient’s body to minimize the spread of droplets and then proceed with chest compressions. Because the patient would presumably be on a ventilator, there is no risk of suffocation.
In Washington state which had the nation’s first covid-19 cases, UW Medicine’s chief medical officer, Tim Dellit, said the decision to send in fewer doctors and nurses to help a coding patient is about “minimizing use of PPE as we go into the surge.” He said the hospital is monitoring health-care workers’ health closely. So far, the percentage of infections among those tested is less than in the general population, which, he hopes, means their precautions are working.
Bioethicist Scott Halpern at the University of Pennsylvania is the author of one widely circulated model guideline being considered by many hospitals. In an interview, he said a blanket stop to resuscitations for infected patients is too “draconian” and may end up sacrificing a young person who is otherwise in good health. However, health-care workers and limited protective equipment cannot be ignored.
“If we risk their well-being in service of one patient, we detract from the care of future patients, which is unfair,” he said.
Halpern’s document calls for two physicians, the one directly taking care of a patient and one who is not, to sign off on do-not-resuscitate orders. They must document the reason for the decision, and the family must be informed but does not have to agree.
Wyese, the Michigan ICU nurse, said his own hospital has been thinking about these issues for years but still is unprepared.
“They made us do all kinds of mandatory education and fittings and made it sound like they are prepared,” he said. “But when it hits the fan, they don’t have the supplies so the plans they had in place aren’t working.”
Over the weekend, Wyese said, a suspected covid-19 patient was rushed in and put into a negative pressure room to prevent the virus spread. In normal times, a nurse in full hazmat-type gear would sit with the patient to care for him, but there was little equipment to spare. So Wyese had to monitor him from the outside. Before he walked inside, he said, he would have to put on a face shield, N95 mask, and other equipment and slather antibacterial foam on his bald head as the hospital did not have any more head coverings. Only one powered air-purifying respirator or PAPR was available for the room and others nearby that could be used when performing an invasive procedure — but it was 150 feet away.
While he said his hospital’s policy still called for a full response to patients whose heart or breathing stopped, he worried any efforts would be challenging, if not futile.
“By the time you get all gowned up and double-gloved the patient is going to be dead,” he said. “We are going to be coding dead people. It is a nightmare.”

/cdn.vox-cdn.com/uploads/chorus_asset/file/19830107/GettyImages_850254782.jpg)
Bill Gates rebuked proposals, floated over the last two days by leaders like Donald Trump, to reopen the global economy despite the Covid-19 coronavirus outbreak, saying that this approach would be “very irresponsible.”
Gates did not mention Trump by name, but the American president has said that he may decide to relax some of the country’s “social distancing” in order to jumpstart the country’s shut-down economy. Gates, the country’s leading philanthropist, has been among the most active tech leaders in using his resources to try and contain the virus.
“There really is no middle ground, and it’s very tough to say to people, ‘Hey, keep going to restaurants, go buy new houses, ignore that pile of bodies over in the corner. We want you to keep spending because there’s maybe a politician who thinks GDP growth is all that counts,’” Gates said in an interview with TED Tuesday. “It’s very irresponsible for somebody to suggest that we can have the best of both worlds.”
Trump has suggested that this middle ground would indeed be possible — by letting some healthy people return to work, for instance, while keeping more vulnerable workers in their homes. Experts have said that drastic and widespread social distancing is required to keep the pandemic from spreading further. Trump has said he would make a decision at the end of the month but has said that he believes the “cure” could be worse than the “problem itself.”
Asked what he would do if he were president, Gates returned to his concerns about reopening the economy.
“The economic effect of this is really dramatic. Nothing like this has ever happened to the economy in our lifetimes,” Gates said. “But bringing the economy back … that’s more of a reversible thing than bringing people back to life. So we’re going to take the pain in the economic dimension — huge pain — in order to minimize the pain in the diseases-and-death dimension.”
The Bill and Melinda Gates Foundation has put up $100 million for programs to fund testing and science around the pandemic, and he has begun using his public profile, too, to shape the coronavirus conversation. This month, Gates himself resigned from the board of Microsoft, which he founded, and is now effectively a full-time philanthropist — and the country’s most famous one.
And Gates has tried to cast himself as an optimist. He has said that the social distancing measures might need to last as little as six weeks, but said that “we have no choice,” despite the economic impacts.
“It’s disastrous for the economy,” Gates said. But “the sooner you do it in a tough way, the sooner you can undo it and go back to normal.”

President Trump said at a Fox News town hall Tuesday that he would “love” to have the country “opened up, and just raring to go” by Easter, or April 12, despite warnings from public health officials that easing social distancing restrictions too soon could cause the number of coronavirus cases to skyrocket.
New York City Mayor Bill de Blasio told a news conference Tuesday he plans to release from Rikers Island some 300 nonviolent inmates who are over 70 years old as a measure against the novel coronavirus pandemic.
The USS Theodore Roosevelt reported three cases of sailors contracting COVID-19 Tuesday, Navy officials said at a briefing — marking the first U.S. sailors to test positive aboard a Navy ship while at sea.
A minor died from the novel coronavirus in Los Angeles County, California, the county’s health department said Tuesday, although it later said that “there may be an alternate explanation” for the death of a California teenager whose “early tests indicated a positive result for COVID-19.”
The trade groups representing hospitals, doctors and nurses called on the public today to stay at home to slow the spread of the new coronavirus.
Up to 5,000 students will be allowed to return to Liberty University’s campus this week, as the Lynchburg, Virginia, college bucks the national trend of school closures.
https://www.axios.com/new-york-battle-coronavirus-58626845-3b0f-4afb-89e7-12be2346396b.html

New York’s fight against the novel coronavirus is also the nation’s fight, as the state — and the city in particular — emerges with “astronomical numbers” of cases, to quote Gov. Andrew Cuomo.
Why it matters: The Empire State has 5% of the world’s COVID-19 cases and about 50% of the nation’s. Its success — or failure — in fighting the virus, safeguarding citizens and treating the afflicted will tell us a lot about what can succeed in the rest of the U.S.
It’s a national travel hub, so it could be the catalyst for outbreaks elsewhere.
Cuomo is trying to shut the state down and stop the spread.
A pivotal moment: Cuomo spoke passionately at a press conference Tuesday about the importance of devoting all resources to New York’s rapidly escalating caseload.
Later in the day, at a media briefing by the White House coronavirus task force, the White House advised people who had recently left New York City to self-quarantine for 14 days.
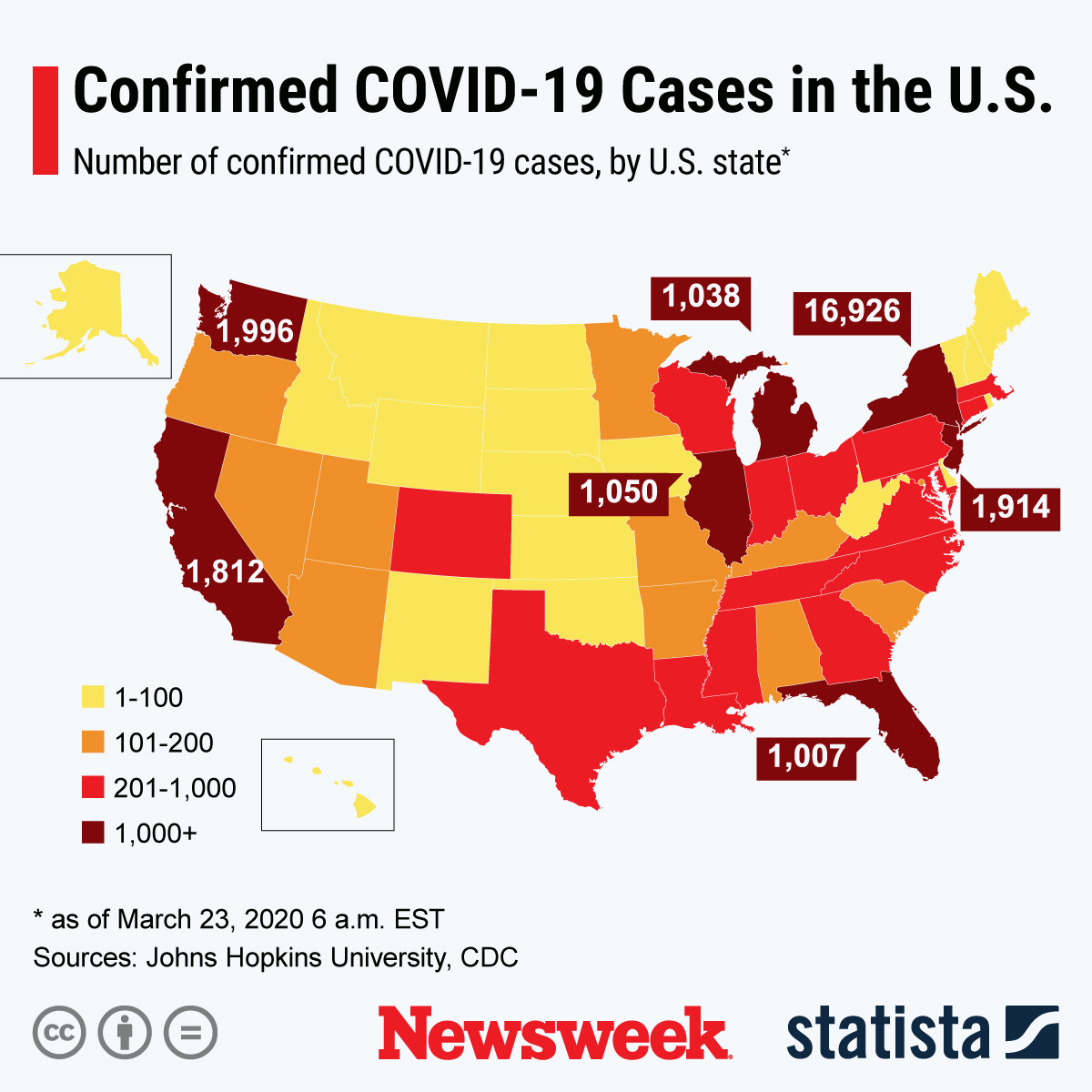
By the numbers: New York has 25,000 cases of the novel coronavirus, vs. 2,800 in California, 2,200 in Washington state and 1,200 in Florida, Cuomo said.
New York is throwing everything against the wall. Not only have residents been told to stay home whenever possible — and schools and most retail stores are closed — but the state is also trying experimental treatments and testing far more people for the virus than other places in the U.S.
“What happens in New York, we can expect to see in other cities around the world, but maybe not at the same scale,” Denis Nash, an epidemiologist at City University of New York’s school of public health, told Axios.
Be smart: Population density, which a New York Times headline called a “trait defining New York life,” is the reason the Big Apple has become the U.S. focal point.
As the densest city in the country, “New York is really a testing ground” for ways to fight the coronavirus, Tomas Hoyos, co-founder of Voro, an online social network where people share recommendations for doctors, told Axios.
My thought bubble: As a born-and-bred New Yorker who watched from my office window as the second plane hit the Twin Towers on 9/11, I find eerie similarities between the empty streets I see this week — and the constant wail of emergency sirens — and the days after the terror attacks.

If President Trump follows through on his statements that he wants to “open” the U.S. up again, an already patchwork shield of state “stay at home” orders could look like even more of a patchwork, Axios’ David Nather reports.
The big picture: Just 17 states have ordered people to stay at home, and most of those are states with Democratic governors. Only Ohio, Indiana, Massachusetts and West Virginia have Republican governors.
Between the lines: Some Republican governors, like Greg Abbott of Texas, have resisted calls to issue statewide stay-at-home orders, leaving it to cities and counties to issue their own restrictions.
The bottom line: The “mitigation strategy” of social distancing urged by health experts has been uneven throughout the U.S. — and it’s likely to get more uneven.

The U.S. keeps reacting too late to the novel coronavirus, prolonging its economic pain and multiplying its toll on Americans’ health.
Why it matters: The spread and impact of the coronavirus may be unfathomable, but it’s not unpredictable. And yet the U.S. has failed to respond accordingly over and over again.
First, it happened with testing — a delay that allowed the virus to spread undetected.
Between the lines: Proactive containment and mitigation steps would have required extraordinary political and economic capital, especially if they had come early in the process, when many Americans didn’t grasp the full weight of this challenge.
Now, even as testing and hospital capacity remain limited, President Trump is eager for an economic recovery — even though, by all estimates, the outbreak is only going to get worse.
The bottom line: When I asked one senior Health and Human Services official how all of this keeps happening, the official said it’s at least partially due to disconnects — between Trump and his administration; between the government and the private sector, and between the U.S. and the rest of the world.
