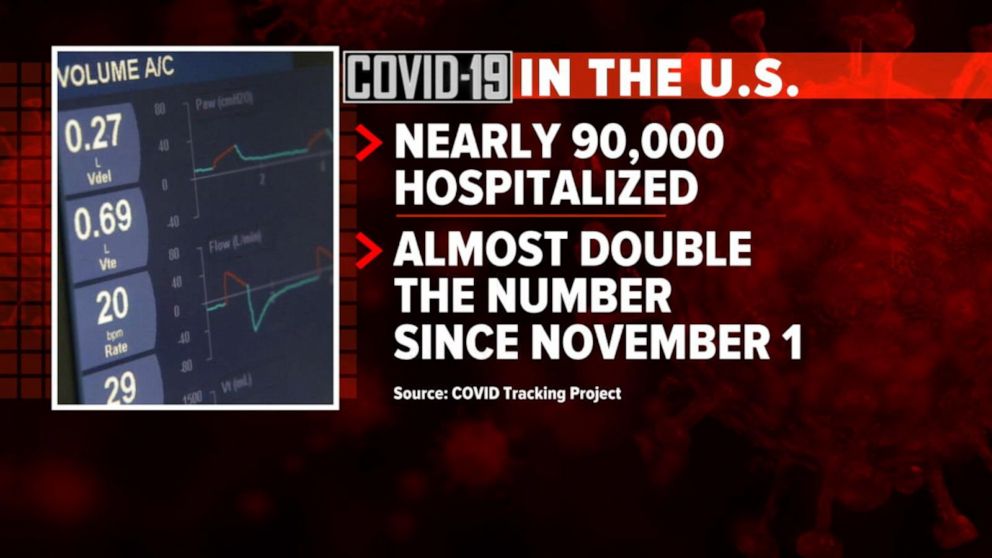
The United States recorded 90,481 people currently hospitalized with COVID-19 Nov. 26, marking the 17th consecutive day of record hospitalizations and the first time the daily count topped 90,000, according to The COVID Tracking Project.
The Project has noted that several data points will likely “wobble” over the next several days due to the Thanksgiving holiday, which may cause data points for COVID-19 testing, new cases and deaths to flatten or drop for several days before spiking. It is unlikely that Thanksgiving infections will be clearly visible in official case data until at least the second week of December.
However, the Project’s staff has noted that the new admissions metric in the public hospitalization dataset from HHS shows only moderate volatility and will likely be an additional source of useful data through the expected holiday dip and subsequent spike in test, case and death data.
“If you’re a reporter covering COVID-19, we recommend focusing on current hospitalizations and new admissions as the most reliable indicator of what is actually happening in your area and in the country as a whole,” reads the Nov. 24 blog from The COVID Tracking Project.
Sanford Health’s CEO Kelby Krabbenhoft is leaving the top exec role after almost 25 years, according to a Tuesday announcement from the Sioux Falls, South Dakota-based system, following controversial statements the outgoing CEO made about mask wearing during the coronavirus pandemic.
Krabbenhoft, who has served as CEO since 1996, sent an internal memo to Sanford’s 50,000 employees on Wednesday arguing wearing a mask would defeat its purpose, as he’d already contracted COVID-19 and was therefore immune for at least seven months, as first reported by Forum News Service.
Experts dispute, however, that people previously infected with the novel coronavirus are entirely immune, as the data is not yet definitive. Other Sanford executives sent an email to employees Friday recommending mask wearing and contradicting Krabbenhoft’s claims.
On the heels of the news, Sanford’s board of trustees and Krabbenhoft have now “mutually agreed to part ways,” according to the release. The turnover comes at an acutely crucial time for the major Midwest health system, as it signed a letter of intent last month to merge with Salt Lake City-based Intermountain Healthcare.
If the deal closes, the two would operate 70 hospitals and 435 clinics — many of which will be located in rural communities across the country — and insure 1.1 million people. The merger would form one of the nation’s largest nonprofit health systems with more than $13 billion in combined annual revenue. It’s expected to close in 2021, pending regulatory approvals.
While Intermountain CEO Marc Harrison is slated to lead the combined organization, Krabbenhoft was poised to serve as president emeritus. It’s unclear what the plans are now after Krabbenhoft’s exit.
Sanford, which operates 46 hospitals in 26 states, did not reply to requests for comment by time of publication.
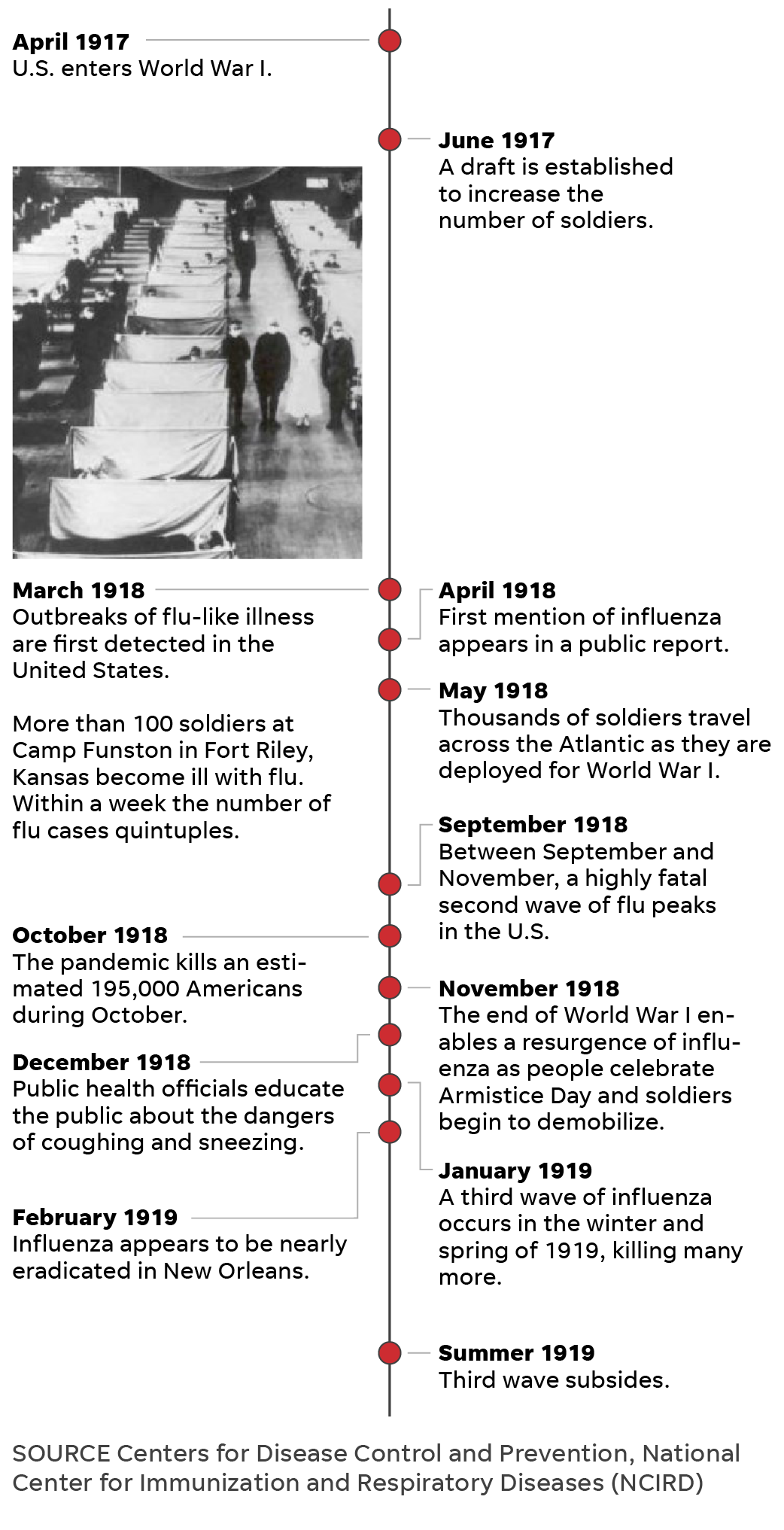
On Thanksgiving more than a century ago, many Americans were living under quarantines, and officials warned people to stay home for the holiday.
More than 200,000 dead since March. Cities in lockdown. Vaccine trials underway.
And a holiday message, of sorts: “See that Thanksgiving celebrations are restricted as much as possible so as to prevent another flare-up.”
It isn’t the message of Thanksgiving 2020. It’s the Thanksgiving Day notice that ran in the Omaha World Herald on Nov. 28, 1918, when Americans found themselves in a similar predicament to the millions now grappling with how to celebrate the holiday season amid the coronavirus pandemic.
“Every time I hear someone say these are unprecedented times, I say no, no, they’re not,” said Brittany Hutchinson, assistant curator at the Chicago History Museum. “They did this in 1918.”
On Thanksgiving more than a century ago, many Americans, like today, lived under various phases of quarantines and face mask orders. Millions mourned loved ones. And health officials in many cities issued the same holiday warning: Stay home and stay safe.
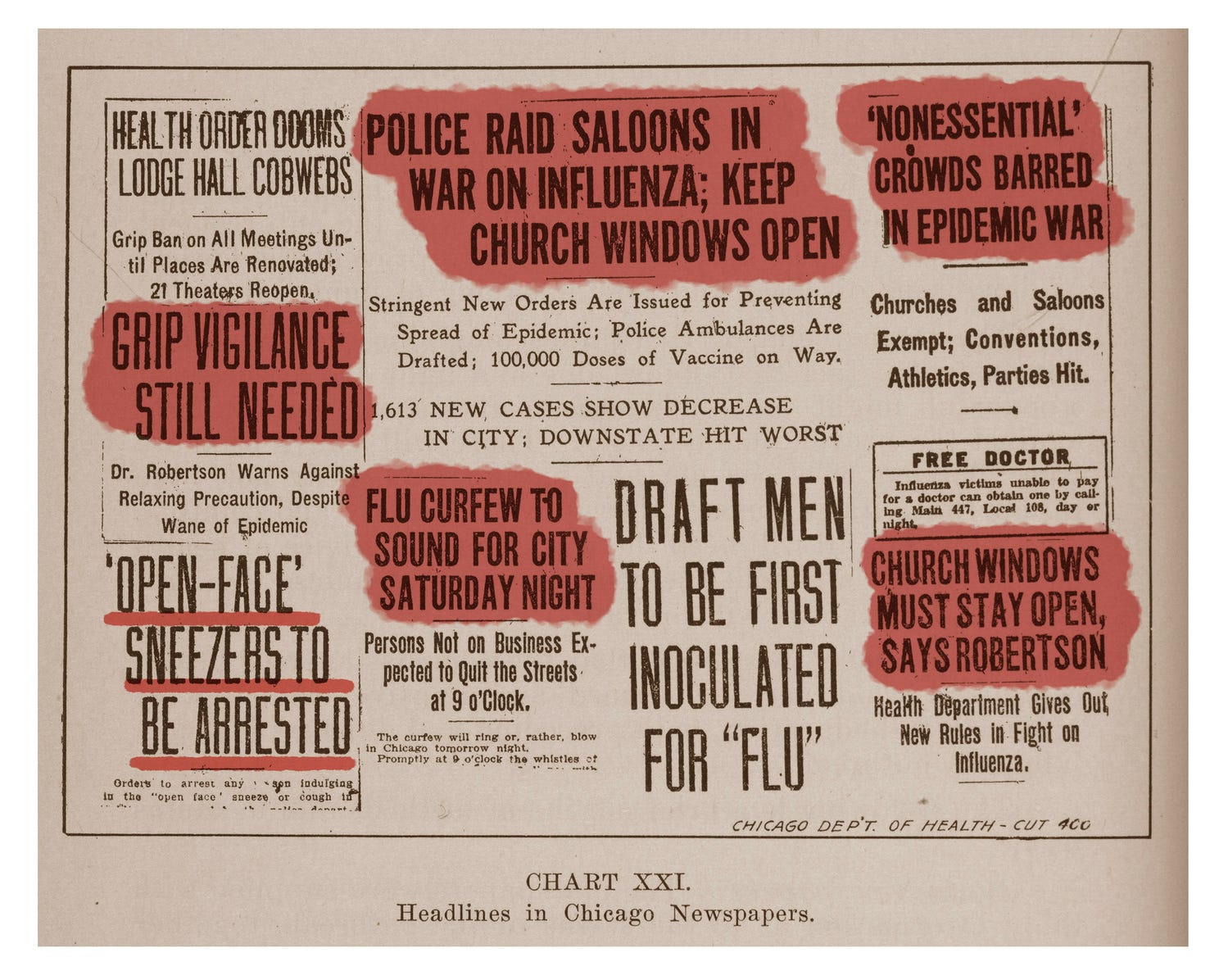
The first cases were detected in the USA in March of that year, growing exponentially by the fall. In October, the virus burned through the nation. Dozens of cities implemented face mask orders and curfews and locked down for two to three weeks, temporarily closing schools, libraries, theaters, movie houses, dance halls, churches, ice cream parlors and soda shops. The virus killed about 195,000 Americans during October alone.
As Thanksgiving rolled around, some cities celebrated the relaxation of flu-related restrictions– partly due to opposition campaigns by retailers, theater owners, unions, mass transportation companies and other economically stressed stakeholders. Washington, Indianapolis and Oakland, California, had lifted restrictions days before, and San Francisco was on the brink of lifting its mask mandate.
San Francisco had one of the nation’s largest anti-masking campaigns, spearheaded by the Anti-Mask League of San Francisco, according to Howard Markel, a professor of the history of medicine at the University of Michigan and co-editor-in chief of The American Influenza Epidemic of 1918-1919. Many people refused to wear masks and were arrested, and when the “line into the courtroom was so long, they laid off arresting people because the system couldn’t enforce it,” Markel said.
On Nov. 13, the San Francisco Examiner reported that “Thanksgiving Day will be celebrated in San Francisco by the discarding of gauze masks, if the present rate of decrease in influenza continues.”
A week later, San Franciscans ceremoniously removed their masks as a whistle sounded across the city at noon. “San Francisco Joyously Discards Masks In Twinkling; Faces Beam As Gauze Covers Come Off At Time Fixed,” the San Francisco Chronicle wrote on its front page Nov. 22.
Resistance to public health measures was not as “vociferous or widespread as today,” but it was there, Markel said. “A lot of these rules and regulations were wrapped up in the patriotism of World War I, and most people followed them. But we don’t have that unifying situation right now. You would think the pandemic would be unifying.”
In some cities, Thanksgiving rituals brought a welcome sense of normalcy. Many Americans returned to religious services, performed charity work and went through with planned football games, parties and performances.
In Portland, a “grand reunion service” was planned for the Sunday after Thanksgiving, “in honor of the reassembling after being debarred from worship on account of the epidemic for the last five weeks.” Members of various congregations were “ready to greet each other after the long absence,” according to the Oregon Daily Journal on Nov. 16.
“The chimes of church bells will once more be heard on Sunday morning throughout the city, beckoning one and all to attend their chosen place of worship, where a double celebration will be held, first over the suppression of autocracy and, second, over the eradication of a frightful plague,” the paper wrote.
Rabbis, priests, pastors and more conveyed a unified message, Hutchinson said – one of “forgiveness and compassion.”
“People are urging to be considerate of one another, to care for one another,” Hutchinson said. “There are messages of putting the smallness of the individual into perspective with the vastness of humanity.”
Other cities were still trending in the opposite direction.
Lockdowns, quarantines on Thanksgiving
By the end of November, cases were rising in cities such as Atlanta, Denver, Louisville, Kentucky, Milwaukee, Omaha, Nebraska, Portland, Oregon, and Richmond, Virginia. Many health experts attributed the “renewal of the grip epidemic” to festivities Nov. 11 – later designated as Armistice Day – when thousands flooded the streets to celebrate the end of WWI.
“It is not the lifting of the closure ban that is the cause of spreading of the epidemic but the putting aside of all precautions and restrictions by the people of Denver when they celebrated on Victory Day,” City Manager of Health and Charity William H. Sharpley told the Denver Post in a story Nov. 21.
On Nov. 27, the day before Thanksgiving, St. Louis reported its highest new daily case count since the epidemic began, and Buffalo, New York, reported its largest jump in daily cases since the lifting of its pandemic ban weeks earlier. Both cities subsequently cracked down on public gatherings, limited the number of passengers on streetcars and ordered those cars to be ventilated and cleaned.
In Salt Lake City, residents were under “quarantine” on Thanksgiving, shops were prohibited from holding sales and celebrations were postponed until Christmas Day. Placards indicating households infected with influenza were placed on the front and rear entrances of 2,000 homes.
“Owing to the influenza quarantine, the day’s festivities … had to be postponed till Christmas day. But Thanksgiving services of some sort are being held in nearly every home,” an article on the front page of the Desert Evening News said. “Because the influenza quarantine prevents public gatherings, the day in Utah is being observed quietly and without any spectacular features.”
Officials in Los Angeles promoted a “Stay at Home Week” over Thanksgiving. The Los Angeles Times issued a call on its front page to “REMEMBER AFFLICTED THANKSGIVING DAY; Influenza Ban Is Felt,” saying, “Thanksgiving Day held many attractions, although in a modified sense.”
“The salvation Army served fifty pounds of turkeys to fifty old men, but dispensed with its usual big dinner to the outcasts at the headquarters, because of the influenza ban,” the Times wrote.
Denver, which was under a face mask order, had just opened three emergency hospitals and issued an urgent call for nurses. Churches were expected to hold Thanksgiving services, but “extra precautions will be taken to guard against spread of epidemic,” the Rocky Mountain News reported the day before.
“Special pains have been taken to provide all the ventilation necessary and to make attendance at the services safe in spite of the influenza epidemic. In a number of churches electric fans have been placed in the auditoriums so as to change the air every few minutes,” the article said.
In many cities, traditional Thanksgiving Day pageants were held outside. In Cincinnati, which saw a surge in cases among children and firemen, Thanksgiving “exercises” at school were held in auditoriums instead of classrooms to “avoid crowding,” the Cincinnati Enquirer wrote Nov. 28.
A handful of cities began to see a surge in cases on Thanksgiving.
Cities see cases rise on Thanksgiving
Cincinnati health officials “requested parents to forego children’s parties and gatherings during the Thanksgiving vacation,” but the number of hospitalized patients rose on the holiday. Schools added an extra day of vacation to the Thanksgiving holiday break to promote “a beneficial result in the influenza situation.”
“We are not in a happy frame of mind tonight,” Dr. Walter List, superintendent of the city’s General Hospital, told the Cincinnati Enquirer on Thanksgiving. “An institution such as this can stand the strain of an epidemic for five or six weeks, but when it continues for such a long period the situation is complicated.”
Kansas City saw a similar trend. The week of Thanksgiving, the number of flu cases at the city’s General Hospital doubled, and on Thanksgiving Day, city health officials reinstituted home quarantine for influenza victims and their families. Schools on break for Thanksgiving were closed until further notice.
Public dance halls and restaurants were closed on Thanksgiving in Spokane, Washington, and private parties were prohibited. The next day, the city’s emergency hospital received more applications for admission than on any other day during the entire epidemic. On Thanksgiving, “the hospital was filled and death a frequent visitor,” the Spokesman-Review wrote.
Jefferson, Iowa, physician C.W. Blake spent much of his Thanksgiving evening making house calls on people ill from influenza, author Thomas Morain wrote in his 1998 book, “Prairie Grass Roots.” Blake was attending a Thanksgiving dinner at a farm outside town and let the local phone operator know he would be available later in the day. When he received the call about patients in the early evening, the operator had a list of 54 patients who had come down with the flu that day.
“At one farm north of Jefferson a family of four was too sick even to make themselves the most simple meal,” Morain wrote. “While Blake checked each one, (his assistant) made a soup from ingredients on hand and left it for the family.”
Hopes of a vaccine on Thanksgiving
By the fall of 1918, scientists were working on an influenza vaccine, and many were developed and used over the course of the pandemic. Researchers in New York, Boston, Pittsburgh, New Orleans and Seattle developed vaccines, and thousands of people in those cities and many others were inoculated.
Days before Thanksgiving, health officers in Rochester, New York, encouraged people to obtain the vaccine available at a health bureau. In Salt Lake City, the emergency hospital gave more than 100 vaccinations Nov. 30. By early December, free inoculation clinics were established across the city, and thousands of residents lined up for their vaccinations.
The problem? Researchers didn’t know influenza was a virus.
“The vaccine that was made was a vaccine against (a bacteria), which they thought was the cause of influenza,” Markel said. “So not only were vaccines of this era crude and not all that effective, the vaccine that they did produce was for the wrong organism.”
Vaccine science was nowhere near the scientifically advanced level of 2020, said Markel, whose mother died from COVID-19 this year. The study of virology was in its infancy, and researchers didn’t have the tools to see viruses. Though bacteria are much larger and can be viewed under a light microscope, viruses require an electron microscope, which had not been invented in 1918, Markel said.
The vaccines that researchers developed did not stop an impending third wave of the flu.
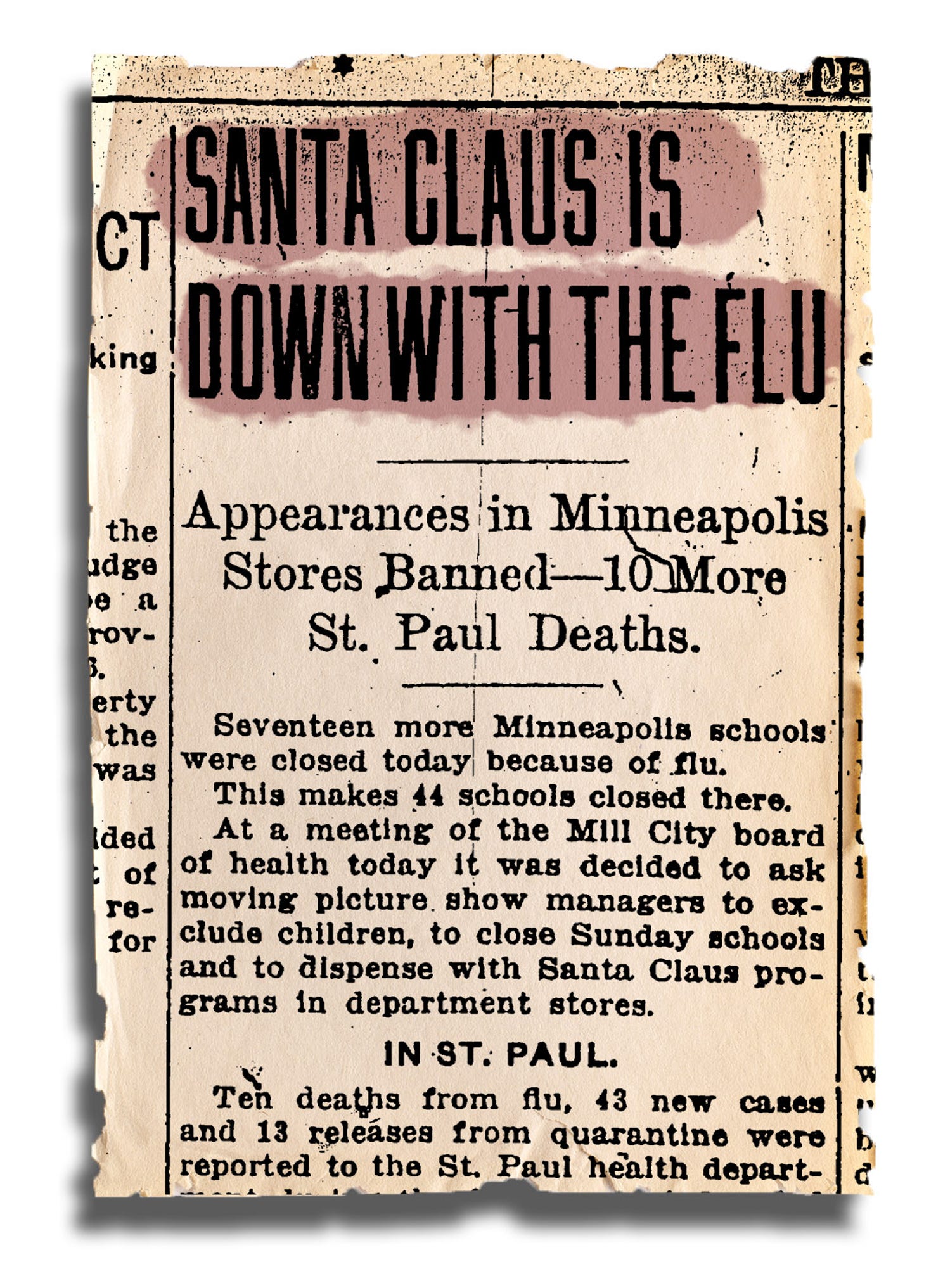
On Dec. 6, the St. Paul Daily Newsannounced that more than 40 Minneapolis schools were closed because of the flu, below the headline “SANTA CLAUS IS DOWN WITH THE FLU.” Health officials asked “moving picture show” managers to exclude children, closed Sunday schools and ordered department stores to dispense with “Santa Claus programs.”
On Christmas Eve, health officials in Nebraska made influenza a mandatory quarantine disease, and fines ranged from $15 to $100 for violations. Approximately 1,000 homes in Omaha were placarded, meaning their occupants were unable to leave for at least four days after the fever had subsided.
“What did they do wrong? That’s hard to say, but all of these measures are like Swiss cheese. They have holes, so you try to use as many layers as possible,” Markel said. “To me, those surges just represented whether there was social distancing or not. Flu didn’t stop circulating, the question was when did people go out and get exposed to it? And that’s what’s going on now.”
A warning for 2020: ‘Stay home and stay safe’
A century later, the nation has recorded more than 12 million cases of COVID-19, and more than 255,000 people in the USA have died. Dozens of states reimplemented coronavirus-related restrictions, and health officials echo the stay-at-home guidance issued decades ago.
“The risk of not traveling is less than the risk of traveling,” Anthony Fauci, the nation’s leading infectious disease expert, told USA TODAY Wednesday. “During this interesting period of a lot of infection going on, colder weather, indoors: Do you want to travel and go to a Thanksgiving meal where there may be 12, 15, 20 people?”
Fauci said his three adult daughters won’t come home for Thanksgiving this year. Hutchinson, the Chicago-based curator who had COVID-19 in April, said she plans to celebrate Thanksgiving at home with her dog and Facetime family members. Markel, in Ann Arbor, said he plans to eat Thanksgiving dinner alone, downsize from a full turkey to a sliced turkey breast and Zoom with family.
If history tells us anything, Markel said, it’s that “the risk of contracting the virus or spreading the virus by congregating in groups or even traditional holiday parties is right now too great.”
“It is disappointing, but let’s get through this, so we can celebrate many, many more Thanksgivings,” he said. “The better part of valor is to stay home and stay safe.”
BLINKING RED: This is a critical week in the coronavirus pandemic. Economists are nervously watching as much of the nation experiences a worsening fall wave, with U.S. case counts near 200,000 a day and record hospitalizations in many parts of the country, my colleagues Paulina Firozi, Lena H. Sun and Hannah Knowles report.
Whether a crest arrives soon could largely be determined by the Thanksgiving holiday, as the Centers for Disease Control and Prevention and health experts warn against traveling and many of the once commonplace rituals of family gatherings.
Early data doesn’t look great:More than 1 million people went through Transportation Security Administration checkpoints in the nation’s airports on Friday —that’s the second-highest single-day rush since March 16. Meanwhile, nearly 80 percent of epidemiologists surveyed recently by the New York Times said they were having Thanksgiving celebrations with people only in their households or not at all.
One bright spot: A third vaccine, made by AstraZeneca, is 90 percent effective if administered in two doses (a half-dose followed by a full-dose booster) and is easier to store than vaccines by Pfizer and Moderna, my colleagues reported this morning.
“The Oxford-AstraZeneca vaccine is likely to be cheaper than those made by Pfizer and Moderna, and it does not need to be stored at subzero temperatures but can be kept in ordinary refrigerators in pharmacies and doctor’s offices,” they wrote.
America’s coronavirus outbreak has surpassed Europe’s.
Why it matters: It wasn’t long ago that public health experts were pointing to Europe as a warning sign for the U.S. But the U.S. now has a higher per capita caseload than the EU ever has during its recent surge.
By the numbers: As of Saturday, 15 states had higher per capita caseloads, averaged over seven days, than the European country with the highest caseload — Luxembourg.
The U.S. overall saw 52.4 cases per 100,000 people. The EU saw 37.6 per 100,000 on Saturday, and peaked at 46.7 cases per 100,000 on Nov. 8.
The big picture: Europe’s steady rise in coronavirus cases over the last couple of months prompted many countries to bring back lockdowns or other strict behavioral restrictions.
Meanwhile, in the U.S., some of the hardest-hit states — like Iowa — are just now adopting mask mandates, and airports over the weekend were packed with people traveling for Thanksgiving.
Yes, but: Cases in the hardest-hit states are starting to trend down, a sign that people are modifying their behavior on their own.
What we’re watching: There’s no sign that the number of U.S. cases nationally is going to stop rising anytime soon, especially in the absence of strong federal or state restrictions.
Hospitalizations and deaths lag behind cases by a few weeks. That means that Europe likely has easier days ahead, while America’s dark days are just getting started.
In the U.S., today’s overwhelmed hospitals will continue to keep getting hit with ever-growing caseloads for awhile.
As record numbers of coronavirus cases overwhelm hospitals across the United States, there is something strikingly different from the surge that inundated cities in the spring: No one is clamoring for ventilators.
The sophisticated breathing machines, used to sustain the most critically ill patients, are far more plentiful than they were eight months ago, when New York, New Jersey and other hard-hit states were desperate to obtain more of the devices, and hospitals were reviewing triage protocols for rationing care. Now, many hot spots face a different problem: They have enough ventilators, but not nearly enough respiratory therapists, pulmonologists and critical care doctors who have the training to operate the machines and provide round-the-clock care for patients who cannot breathe on their own.
Since the spring, American medical device makers have radically ramped up the country’s ventilator capacity by producing more than 200,000 critical care ventilators, with 155,000 of them going to the Strategic National Stockpile. At the same time, doctors have figured out other ways to deliver oxygen to some patients struggling to breathe — including using inexpensive sleep apnea machines or simple nasal cannulas that force air into the lungs through plastic tubes.
But with new cases approaching 200,000 per day and a flood of patients straining hospitals across the country, public health experts warn that the ample supply of available ventilators may not be enough to save many critically ill patients.
“We’re now at a dangerous precipice,” said Dr. Lewis Kaplan, president of the Society of Critical Care Medicine. Ventilators, he said, are exceptionally complex machines that require expertise and constant monitoring for the weeks or even months that patients are tethered to them. The explosion of cases in rural parts of Idaho, Ohio, South Dakota and other states has prompted local hospitals that lack such experts on staff to send patients to cities and regional medical centers, but those intensive care beds are quickly filling up.
Public health experts have long warned about a shortage of critical care doctors, known as intensivists, a specialty that generally requires an additional two years of medical training. There are 37,400 intensivists in the United States, according to the American Hospital Association, but nearly half of the country’s acute care hospitals do not have any on staff, and many of those hospitals are in rural areas increasingly overwhelmed by the coronavirus.
“We can’t manufacture doctors and nurses in the same way we can manufacture ventilators,” said Dr. Eric Toner, an emergency room doctor and senior scholar at the Johns Hopkins Center for Health Security. “And you can’t teach someone overnight the right settings and buttons to push on a ventilator for patients who have a disease they’ve never seen before. The most realistic thing we can do in the short run is to reduce the impact on hospitals, and that means wearing masks and avoiding crowded spaces so we can flatten the curve of new infections.”
Medical association message boards in states like Iowa, Oklahoma and North Dakota are awash in desperate calls for intensivists and respiratory therapists willing to temporarily relocate and help out. When New York City and hospitals in the Northeast issued a similar call for help this past spring, specialists from the South and the Midwest rushed there. But because cases are now surging nationwide, hospital officials say that most of their pleas for help are going unanswered.
Dr. Thomas E. Dobbs, the top health official in Mississippi, said that more than half the state’s 1,048 ventilators were still available, but that he was more concerned with having enough staff members to take care of the sickest patients.
“If we want to make sure that someone who’s hospitalized in the I.C.U. with the coronavirus has the best chance to get well, they need to have highly trained personnel, and that cannot be flexed up rapidly,” he said in a news briefing on Tuesday.
Dr. Matthew Trump, a critical care specialist at UnityPoint Health in Des Moines, said that the health chain’s 21 hospitals had an adequate supply of ventilators for now, but that out-of-state staff reinforcements might be unlikely to materialize as colleagues fall ill and the hospital’s I.C.U. beds reach capacity.
“People here are exhausted and burned out from the past few months,” he said. “I’m really concerned.”
The domestic boom in ventilator production has been a rare bright spot in the country’s pandemic response, which has been marred by shortages of personal protective equipment, haphazard testing efforts and President Trump’s mixed messaging on the importance of masks, social distancing and other measures that can dent the spread of new infections.
Although the White House has sought to take credit for the increase in new ventilators, medical device executives say the accelerated production was largely a market-driven response turbocharged by the national sense of crisis. Mr. Trump invoked the wartime Defense Production Act in late March, but federal health officials have relied on government contracts rather than their authority under the act to compel companies to increase the production of ventilators.
Scott Whitaker, president of AdvaMed, a trade association that represents many of the country’s ventilator manufacturers, said the grave situation had prompted a “historic mobilization” by the industry. “We’re confident that our companies are well positioned to mobilize as needed to meet demand,” he said in an email.
Public health officials in Minnesota, Mississippi, Utah and other states with some of the highest per capita rates of infection and hospitalization have said they are comfortable with the number of ventilators currently in their hospitals and their stockpiles.
Mr. Whitaker said AdvaMed’s member companies were making roughly 700 ventilators a week before the pandemic; by the summer, weekly output had reached 10,000. The juggernaut was in part fueled by unconventional partnerships between ventilator companies and auto giants like Ford and General Motors.
Chris Brooks, chief strategy officer at Ventec Life Systems, which collaborated with G.M. to fill a $490 million contract for the Department of Health and Human Services, said the shared sense of urgency enabled both companies to overcome a thicket of supply-chain and logistical challenges to produce 30,000 ventilators over four months at an idled car parts plant in Indiana. Before the pandemic, Ventec’s average monthly output was 100 to 200 machines.
“When you’re focused with one team and one mission, you get things done in hours that would otherwise take months,” he said. “You just find a way to push through any and all obstacles.”
Despite an overall increase in the number of ventilators, some researchers say many of the new machines may be inadequate for the current crisis. Dr. Richard Branson, an expert on mechanical ventilation at the University of Cincinnati College of Medicine and an author of a recent study in the journal Chest, said that half of the new devices acquired by the Strategic National Stockpile were not sophisticated enough for Covid-19 patients in severe respiratory distress. He also expressed concern about the long-term viability of machines that require frequent maintenance.
“These devices were not built to be stockpiled,” he said.
The Department of Health and Human Services, which has acknowledged the limitations of its newly acquired ventilators, said the stockpile — nine times as large as it was in March — was well suited for most respiratory pandemics. “These stockpiled devices can be used as a short-term, stopgap buffer when the immediate commercial supply is not sufficient or available,” the agency said in a statement.
Projecting how many people will end up requiring mechanical breathing assistance is an inexact science, and many early assumptions about how the coronavirus affects respiratory function have evolved.
During the chaotic days of March and April, emergency room doctors were quick to intubate patients with dangerously low oxygen levels. They subsequently discovered other ways to improve outcomes, including placing patients on their stomachs, a protocol known as proning that helps improve lung function. The doctors also learned to embrace the use of pressurized oxygen delivered through the nose, or via BiPAP and CPAP machines, portable devices that force oxygen into a patient’s airways.
Many health care providers initially hesitated to use such interventions for fear the pressurized air would aerosolize the virus and endanger health care workers. The risks, it turned out, could be mitigated through the use of respirator masks and other personal protective gear, said Dr. Greg Martin, the chief of pulmonary and critical care at Grady Health Systems in Atlanta.
“The familiarity of taking care of so many Covid patients, combined with good data, has just made everything we do 100 times easier,” he said.
Some of the earliest data about the perils of intubating coronavirus patients turned out to be incomplete and misleading. Dr. Susan Wilcox, a critical care specialist at Massachusetts General Hospital, said many providers were spooked by data that suggested an 80 percent mortality rate among ventilated coronavirus patients, but the actual death rate turned out to be much lower. The mortality rate at her hospital, she said, was about 25 to 30 percent.
“Some people were saying that we should intubate almost immediately because we were worried patients would crash and have untoward consequences if we waited,” she said. “But we’ve learned to just go back to the principles of good critical care.”
Survival rates have increased significantly at many hospitals, a shift brought about by the introduction of therapeutics like dexamethasone, a powerful steroid that Mr. Trump took when he was hospitalized with the coronavirus. The changing demographics of the pandemic — a growing proportion of younger patients with fewer health risks — have also played a role in the improving survival rates.
Dr. Nikhil Jagan, a critical care pulmonologist at CHI Health, a hospital chain that serves Iowa, Kansas and Nebraska, said many of the coronavirus patients who were arriving at his emergency room now were less sick than the patients he treated in the spring.
“There’s a lot more awareness about the symptoms of Covid-19,” he said. “The first go-around, when people came in, they were very sick right off the bat and in respiratory distress or at the point of respiratory failure and had to be intubated.”
But the promising new treatments and enhanced knowledge can go only so far should the current surge in cases continue unabated. The country passed 250,000 deaths from the coronavirus last week, a reminder that many critically ill patients do not survive. The daily death toll has been rising steadily and is approaching 2,000.
“Ventilators are important in critical care but they don’t save people’s lives,” said Dr. Branson of the University of Cincinnati. “They just keep people alive while the people caring for them can figure out what’s wrong and fix the problem. And at the moment, we just don’t have enough of those people.”
For now, he said there was only one way out the crisis: “It’s not that hard,” he said. “Wear a mask.”
As we navigate the greatest health crisis of our lifetimes, it turns out that many aspects of our experiences in 2020 aren’t as “unprecedented” as we may think. The widely varied pandemic responses by local and state officials (and resulting political polarization) occurring today also transpired over 100 years ago during the Spanish Flu.
Lessons from a century ago may be worth revisiting: the left side of the graphic above details the health and economic case for public health mitigation strategies.Cities that enacted “longer interventions” (including mask mandates, closures, business capacity restrictions, and social distancing measures) in 1918 experienced fewer deaths per capita, as well as higher employment gains through 1919, compared to “similar” cities that enacted “shorter interventions.” For example, Los Angeles, which declared a state of emergency and banned all public gatherings early in the pandemic, had 25 percent fewer deaths per capita, and a 27 percentage-point greater gain in subsequent employment than San Francisco, which mainly focused on urging residents to wear masks in public.
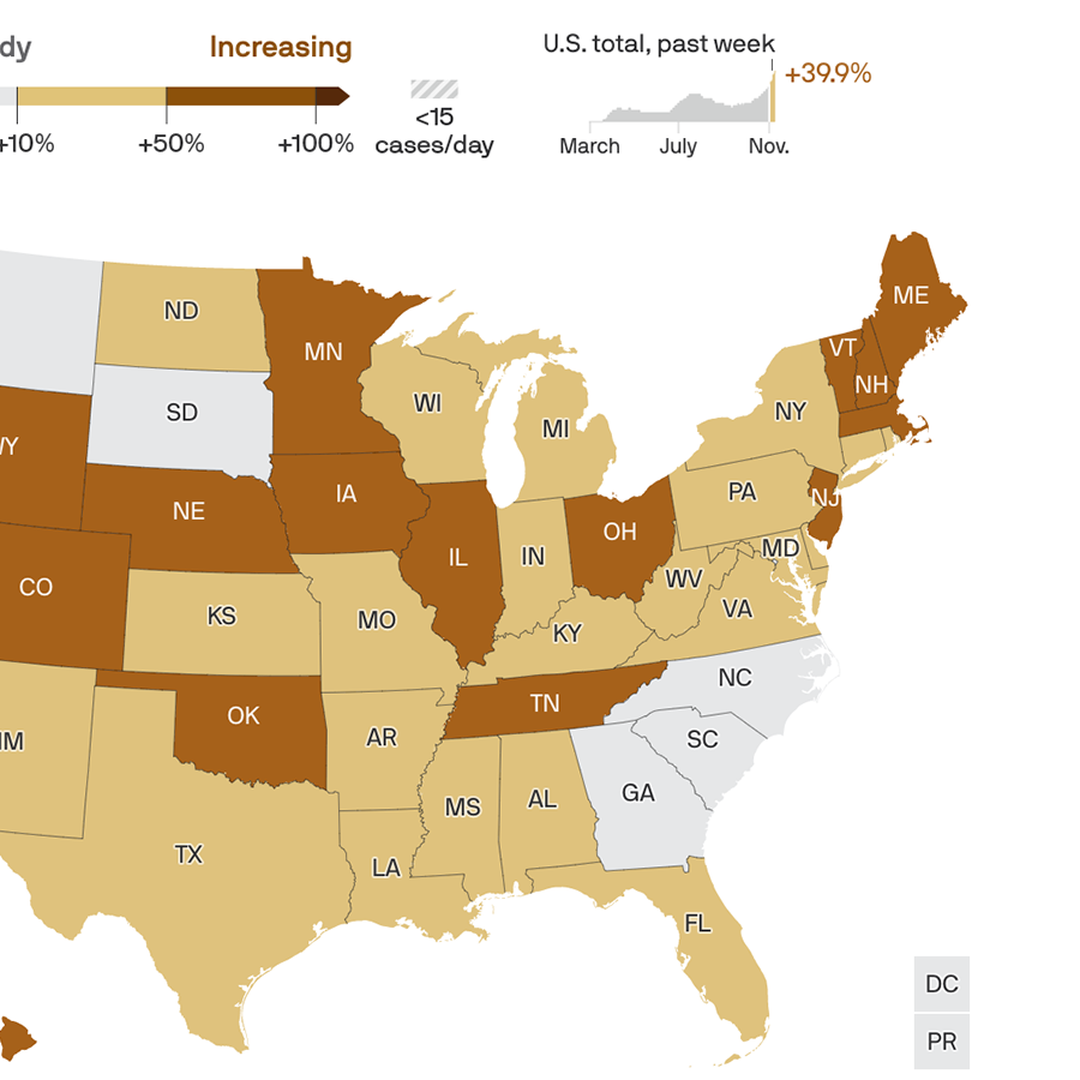
Fast forward to today, when we’re also seeing significant differences between COVID containment policies at the state level. The right side of the graphic shows thatstates with the weakest overall pandemic containment policies are currently experiencing the worst outbreaks, measured here by hospitalizations per capita. States like Hawaii and New York, which maintained many of the strict mitigation strategies first put into place in the spring, are seeing those restrictions pay off with fewer hospitalizations during the latest spike.
Conversely, Iowa and the Dakotas have fewer, and less stringent, public health measures, and are now seeing the highest surges in the country today. (New Mexico shows that state-level policy decisions don’t explain everything—it’s currently battling a serious outbreak despite maintaining some of the strongest containment measures over the course of the pandemic.)
As we head into the worst COVID wave so far, the debate over whether saving “lives” or “livelihoods” should dominate the pandemic response rages on.History shows that higher levels of public health intervention can both save lives and result in stronger economic recovery.
Sioux Falls, S.D.-based Sanford Health President and CEO Kelby Krabbenhoft shared his thoughts about having COVID-19 and why he won’t be wearing a mask in an email to health system staff, according to the Grand Forks Herald.
In the 1,000-word email sent Nov. 18, Mr. Krabbenhoft said he had COVID-19, but he’s now back in his office working without a mask. He said he won’t be wearing a mask because doing so would only be a “symbolic gesture.” He considers himself immune from the virus.
“The information, science, truth, advice and growing evidence is that I am immune for at least seven months and perhaps for years to come, similar to that of chicken pox, measles, etc. For me to wear a mask defies the efficacy and purpose of a mask and sends an untruthful message that I am susceptible to infection or could transmit it,” Mr. Krabbenhoft wrote. “I have no interest in using masks as a symbolic gesture when I consider that my actions in support of our family leave zero doubt to my support of all 50,000 of you. My team and I have a duty to express the truth and facts and reality and not feed the opposite.”
The CDC says those who have had COVID-19 should take steps to reduce the risk of spreading the virus, including wearing a mask in public places and staying at least 6 feet away from other people.
In his email, Mr. Krabbenhoft argues the “on-again, off-again” use of masks is absurd. “Masks have been a symbolic issue that frankly frustrates me,” he wrote.
“On the other hand, for people who have not contracted the virus and may acquire it and then spread it … it is important for them to know that masks are just plain smart to use and in their best interest,” Mr. Krabbenhoft wrote.
The health system CEO concluded his letter by sharing his optimism for the future, noting that some Sanford Health workers would be among the first to get a COVID-19 vaccine once it is available.
Sanford Health didn’t respond to Becker’s Hospital Review‘s request for comment by deadline.
Read the Grand Forks Herald article here, which includes full text of the email Mr. Krabbenhoft sent to employees.
No state in America could clear the threshold right now to safely allow indoor gatherings, Axios’ Sam Baker and Andrew Witherspoon report.
The big picture: This is bad as the pandemic has ever been — the most cases, the most explosive growth and the greatest strain on hospitals.
If businesses were closed right now, it would not be safe to reopen them. And holiday travel will be risky no matter where you’re coming from or where you’re going.
By the numbers: Over the past week, the U.S. averaged more than 154,000 new cases per day, the highest rate of the entire pandemic.
The number of new infections rose in 46 states, held steady in three, and declined in only one — Hawaii.
This week’s nationwide totals are a 30% increase over last week, which was a 40% increase over the week before that. Daily infections have been rising by at least 15% for the past six weeks.
Testing was up about 11% over the past week. The U.S. is now conducting about 1.5 million tests per day. That’s a lot, but cases clearly are still rising faster than testing.
Between the lines:Whatever metric you might use to decide whether it’s safe to have a large Thanksgiving get-together, or to sit inside a bar or restaurant, the answer is probably no.
Experts recently told The Atlantic that they wouldn’t feel comfortable attending an indoor dinner party at all, but that it would be least risky in areas with only about 10–25 new cases per day, per 100,000 people.
The bottom line: Eating and drinking indoors with large groups of people, at a time when 150,000 people are contracting the virus every day, is about as risky as it gets.