The Democrats’ reconciliation bill includes several major health care pieces backed by different lawmakers and advocates, setting up a precarious game of policy Jenga if the massive measure needs to be scaled back.
Between the lines:Health care may be a priority for Democrats. But that doesn’t mean each member values every issue equally.
Why it matters: As the party continues to hash out the overall price tag of its giant reconciliation bill, it’s worth gaming out which policies are on the chopping block — and which could potentially take the entire reconciliation bill down with them.
There are clear winners of each pillar of Democrat’s health plan:
Seniors benefit from expanding Medicare to cover dental, vision and hearing benefits.
Low-income people — primarily in the South and disproportionately people of color — in non-expansion states benefit if the Medicaid gap is closed, giving them access to health coverage.
Affordable Care Act marketplace enrollees benefit if the increased subsidy assistance that Democrats enacted earlier this year is extended or made permanent.
Elderly and Americans with disabilities benefit from an expansion of their home-based care options, and their caretakers benefit from a pay bump.
Seniors — and potentially anyone facing high drug costs — benefit if Medicare is given the authority to negotiate drug prices, although the drug industry argues it will lead to fewer new drugs.
Yes, but:Each of these groups face real problems with health care access and affordability. But when there’s a limited amount of money on the table — which there is — even sympathetic groups can get left in the dust.
Each policy measure, however, also has powerful political advocates. And when Democrats have a razor-thin margin in both the House and the Senate, every member has a lot of power.
Seniors are disproportionately powerful on their own, due to their voting patterns. But expanding what Medicare covers is extremely important to progressives — including Sen. Bernie Sanders.
Closing the Medicaid gap is being framed as a racial justice issue, given that it disproportionately benefits people of color. And although many Democrats hail from expansion states — particularly in the Senate — some very powerful ones represent non-expansion states.
These members include Sen. Raphael Warnock, who represents Georgia and is up for re-election next year in an extremely competitive seat, and Rep. Jim Clyburn, who arguably is responsible for President Biden winning the 2020 primary.
The enhanced ACA subsidies are scheduled to expire right before next years’ midterm elections. Democrats’ hold on the House is incredibly shaky already, making extending the extra help a political no-brainer.
Expanding home-based care options was one of the only health care components of Biden’s original framework for this package. But aside from the president’s interest in the issue, unions care a lot about it as their members stand to gain a pay raise — and Democrats care a lot about what unions care about.
And finally, giving Medicare the power to negotiate drug prices has the most powerful opponents, theoretically making it vulnerable to the chopping block. But it also polls very highly, and perhaps even more importantly, produces enough government savings to help pay for these other health care policies.
The bottom line: “From a political perspective, none of these health care proposals seem very expendable,” said KFF’s Larry Levitt.
Most — if not all of them — can be scaled to save money.
But there are also powerful constituencies for the other components of the bill that address issues like child care and climate change, meaning these health care measures aren’t only competing against one another.
And, Levitt points out, “there’s always a difference between members of Congress staking out positions and being willing to go to nuclear war over them.”
Health spending in the United States is highest in the world, driven in part by administrative complexity. To date, studies examining the administrative costs of American health care have primarily focused on clinicians and organizations—rarely on patients.
A new study in Health Services Research finds administrative complexity in the U.S. health care system has consequences for access to care that are on par with those of financial barriers like copays and deductibles. In other words, we pay for health care in two ways: in money and in the hassle of dealing with a complex, confusing, and error-riddled system. Both are barriers to access. The study was led by Michael Anne Kyle, and coauthor, Austin Frakt.
Main Findings
Nearly three-quarters (73%) of people surveyed reported doing at least one health care-related administrative task in the past 12 months. Such administrative tasks include: appointment scheduling; obtaining information from an insurer or provider; obtaining prior authorizations; resolving insurance or provider billing issues; and resolving premium problems.
Administrative tasks often impose barriers to care: Nearly one-quarter (24.4%) of survey respondents reported delaying or foregoing needed care due to administrative tasks.
This estimate of administrative barriers to access to care is similar to those of financial barriers to access: a 2019 Kaiser Family Foundation survey, found that 26% of insured adults 18-64 said that they or a family member had postponed or put off needed care in the past 12 months due to cost.
Administrative burden has consequential implications for equity. The study finds administrative burden falls disproportionately on people with high medical needs (disability) and that existing racial and socioeconomic inequities are associated with greater administrative burden.
Methods
To measure the size and consequences of patients’ administrative roles, we used data from the nationally representative March 2019 Health Reform Monitoring Survey of insured, nonelderly adults (18-64) to assess the annual prevalence of five common types of administrative tasks patients perform: (1) appointment scheduling; (2) obtaining information from an insurer or provider; (3) obtaining prior authorizations; (4) resolving insurance or provider billing issues; (5) and resolving insurance premium problems. The study examined the association of these tasks with two important measures of their burden: delayed and forgone care.
Conclusions
High administrative complexity is a central feature of the U.S. health care system. Largely overlooked, patients frequently do administrative work that can create burdens resulting in delayed or foregone care. The prevalence of delayed or foregone care due to administrative tasks is comparable to similar estimates of cost-related barriers to care. Administrative complexity is endemic to all post-industrial health systems, but there may be opportunity to design administrative tools with greater care to avoid exacerbating or reinforcing inequities.
The Centers for Medicare & Medicaid Services (CMS) issued its final payment rule for inpatient hospitals for FY22 this week, giving providers a 2.5 percent pay increase, and implementing a number of other regulatory changes. Of particular note, the rule puts in place a requirement for hospitals and long-term care providers to report on COVID vaccination rates among their workers, amid growing calls for healthcare organizations to mandate vaccines.
The final rule will also extend additional payments to hospitals for delivering COVID care until the end of the public health emergency is declared.
On top of a number of changes to quality reporting programs aimed at reducing the adverse impact of the pandemic on hospital metrics, CMS also used the final inpatient rule to begin acting on the Biden administration’s stated desire of improving health equity by adding a maternal morbidity measure to hospital quality reporting requirements.
The measure will require hospitals to report whether they participate in initiatives to improve perinatal health, an area in which unequal treatment has led to disproportionately adverse outcomes for women of color. In what will surely be welcome news for hospitals, CMS will no longer require disclosure of the contract terms providers strike with Medicare Advantage insurers, which was a key provision of Trump-era transparency regulations.
Nevertheless, based on earlier proposed changes to physician and outpatient surgery payment rules, and the President’s recent executive order on competition policy, we’d anticipate the Biden administration will continue to boost efforts to increase transparency of provider pricing.
First things first, however: there’s a pandemic to get through, and this final inpatient payment rule should largely come as good news to hospitals who are increasingly feeling the strain of a fourth surge of COVID cases.
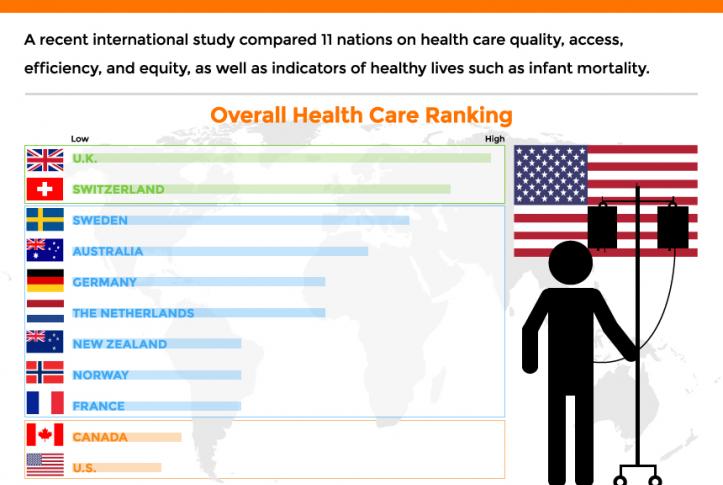
The performance of the U.S. healthcare system ranked last among 11 high-income countries, according to a report released Aug. 4 by the Commonwealth Fund.
To compare the performance of the healthcare systems in 11 high-income countries, the Commonwealth Fund analyzed 71 performance measures across five domains: access to care, care process, administrative efficiency, equity and patient outcomes.
Despite spending far more of its gross domestic product on healthcare than the other nations included in the report, the U.S. ranked last overall, as well as last for access to care, administrative efficiency, equity and patient outcomes. However, the U.S. ranked second on measures of care process, trailing only New Zealand.
Norway, the Netherlands and Australia had the best healthcare system performance, according to the report. In all seven iterations of the study conducted by the Commonwealth Fund since 2004, the U.S. has ranked last. It is the only country included in the study that does not provide its citizens with universal health insurance coverage.
Four features separate the top performing countries from the U.S., according to the report: universal health insurance coverage and removal of cost barriers; investment in primary care systems to ensure equitable healthcare access; reduction of administrative burdens that divert time and spending from health improvement efforts; and investment in social services, particularly for children and working-age adults.
Medicare helps to reduce racial and ethnic disparities and close gaps in insurance coverage, a new study in JAMA Network shows.
Why it matters: This raises the possibility that expanding the program could further reduce health disparities — a timely idea, as Senate Democrats debate lowering the Medicare eligibility age and broadening its benefits, Axios’ Marisa Fernandez reports.
What they found: Medicare access at age 65 sharply reduced the share of Black and Hispanic people reporting poor health and poor access to care, but not mortality, the study notes.
Respondents were “significantly more likely” to be insured immediately after age 65 compared to before turning 65, and coverage increased more for Black and Hispanic adults than white adults.
Medicare eligibility alone doesn’t completely eliminate disparities among the elderly, suggesting other social determinants of health need to be addressed.
State of play:Senate Democrats have signaled that they’ll attempt to expand Medicare to include dental, hearing and vision coverage in the coming months.
Although lowering the Medicare eligibility age from 65 to 60 wasn’t included in their original proposal, Axios has reported it’s still possible that the measure gets included.
During Pride Month we feel it’s especially important to shine a light on the significant health disparities faced by transgender and gender-nonconforming individuals.
Transgender healthcare has been under growing attack in recent months; while the Biden administration formally reinstated Affordable Care Act protections for transgender Americans against discrimination in healthcare, 20 states have introduced anti-trans bills since the start of the year, most featuring provisions that bar physicians from providing trans children with gender-affirming care.
The graphic above shows that transgender individuals are twice as likely as the broader LGBTQ+ population to delay care for fear of discrimination. Trans individuals deal with myriad types of medical discrimination, from being misgendered in routine interactions to being denied treatment. And trans people of color report experiencing this mistreatment even more frequently. Transgender people are also more likely to be uninsured or to delay care for financial reasons, in part because their unemployment and uninsured rates are higher than the national average. Even when they do find supportive providers, nearly 40 percent report that their insurance will not cover essential elements of transitional care, such as hormone therapy.
It’s incumbent on doctors and health systems to strengthen their policies for treating trans individuals. Trans-specific training for clinicians and staff is a great place to start. Even simple shifts in operations—like including preferred name and pronouns on patient records and providing equal access to public restrooms—are small but important steps to providing a safer, more inclusive healthcare experience and reducing transgender health disparities.
For some time, we’ve been focused on the efforts of Walmart to launch and grow a care delivery business, especially as it has piloted an expanded primary care clinic offering in a handful of states. We’ve long thought that access to basic care at the scale that Walmart brings could be transformative, given that more than half of Americans visit a Walmart store every week. Along those same lines, we’ve always wondered why Dollar General and Dollar Tree—each with around four times as many retail locations as Walmart—haven’t gotten into the retail clinic or pharmacy businesses.
(Part of the answer is ultra-lean staffing—this piece gives a good sense of the basic, and troubling, economics of dollar stores.) Now, as the federal government ramps up its efforts to widely distribute the COVID vaccines, it turns out that the CDC is actively discussing a partnership with Dollar General to administer the shots.
A fascinating new paper (still in preprint) from researchers at Yale shows why this could be a true gamechanger. The Biden administration, through its partnership with national and independent pharmacy providers, aims to have a vaccination site within five miles of 90 percent of the US population by next week. Compared to those pharmacy partners, researchers found,Dollar General stores are disproportionately located in areas of high “social vulnerability”, with lower income residents and high concentrations of disadvantaged groups. Particularly in the Southeast, a partnership with Dollar General would vastly increase access for low-income Black and Latino residents, allowing vaccine access within one mile for many, many more people. And the partnership could form the basis for future expansions of basic healthcare services to vulnerable and rural communities, particularly if some of the $7.5B in funding for COVID vaccine distribution went to helping dollar store locations bolster staffing and equipment to deliver basic health services. We’ll be watching with interest to see if the potential Dollar General partnership comes to fruition.
The Biden administration has proposed giving rehabilitation facilities a 2.2% payment increase for the 2022 federal fiscal year that starts in October.
The payment rate outlined in a proposed rule released late Thursday is slightly below the 2.4% that CMS gave rehab facilities for the 2021 federal fiscal year. CMS proposed in a separate rule a 2.3% increase for payments to inpatient psychiatric facilities as well.
Both payment rules also give updates on outlier payments, which help facilities deal with the costs of treating extremely costly beneficiaries.
For rehab facilities, CMS proposes to maintain outlier payments to 3% of the total facility payments for fiscal 2022, which begins on Oct. 1.
CMS also aims to keep the outlier payments for psychiatric facilities at 2% for 2022.
A major change for both rules is a new addition aimed to track coverage of COVID-19 vaccinations among healthcare personnel.
CMS also wants to add vaccination coverage among healthcare personnel as a measure to the quality reporting program for psychiatric facilities. The program outlines quality metrics that facilities need to meet.
“This measure would be reported using the COVID-19 modules on the [Centers for Disease Control and Prevention’s] National Healthcare Safety Network web portal,” a fact sheet on the psychiatric payment rule said.
The agency also is proposing a similar measure for rehab facilities to report any vaccinations of healthcare personnel for COVID-19.
“This proposed measure is designed to assess whether [IRFs] are taking steps to limit the spread of COVID-19 among their [healthcare personnel], reduce the risk of transmission within their facilities and help sustain the ability of [rehabilitation facilities] to continue serving their communities through the public health emergency and beyond,” a fact sheet on the rehab rule said.
In the rehab facility rule, CMS also asked for comments on how to improve health equity for all patients.
CMS is seeking comments on whether to add more measures that address patient equity in standardized patient assessment data elements, which must be collected by facilities after post-acute care.
The agency also wants comments on ways to attain health equity for psychiatric facilities as well.
“CMS is committed to addressing the significant and persistent inequities in health outcomes in the United States through improving data collection to better measure and analyze disparities across programs and policies,” the agency said in a fact sheet.
There’s widespread agreement that it’s important to help older adults and people with disabilities remain independent as long as possible. But are we prepared to do what’s necessary, as a nation, to make this possible?
That’s the challenge President Joe Biden has put forward with his bold proposal to spend $400 billion over eight years on home and community-based services, a major part of his $2 trillion infrastructure plan.
It’s a “historic and profound” opportunity to build a stronger framework of services surrounding vulnerable people who need considerable ongoing assistance, said Ai-jen Poo, director of Caring Across Generations, a national group advocating for older adults, individuals with disabilities, families and caregivers.
It comes as the coronavirus pandemic has wreaked havoc in nursing homes, assisted living facilities and group homes, killing more than 174,000 people and triggering awareness of the need for more long-term care options.
“There’s a much greater understanding now that it is not a good thing to be stuck in long-term care institutions” and that community-based care is an “essential alternative, which the vast majority of people would prefer,” said Ari Ne’eman, senior research associate at Harvard Law School’s Project on Disability.
“The systems we do have are crumbling” due to underfunding and understaffing, and “there has never been a greater opportunity for change than now,” said Katie Smith Sloan, president of LeadingAge, at a recent press conference where the president’s proposal was discussed. LeadingAge is a national association of more than 5,000 nonprofit nursing homes, assisted living centers, senior living communities and home care providers.
But prospects for the president’s proposal are uncertain. Republicans decry its cost and argue that much of what the proposed American Jobs Plan contains, including the emphasis on home-based care, doesn’t count as real infrastructure.
“Though this [proposal] is a necessary step to strengthen our long-term care system, politically it will be a challenge,” suggested Joseph Gaugler, a professor at the University of Minnesota’s School of Public Health, who studies long-term care.
Even advocates acknowledge the proposal doesn’t address the full extent of care needed by the nation’s rapidly growing older population. In particular, middle-income seniors won’t qualify directly for programs that would be expanded. They would, however, benefit from a larger, better paid, better trained workforce of aides that help people in their homes — one of the plan’s objectives.
“This [plan] isn’t everything that’s needed, not by any step of the imagination,” Poo said. “What we really want to get to is universal access to long-term care. But that will be a multistep process.”
Understanding what’s at stake is essential as communities across the country and Congress begin discussing Biden’s proposal.
The services in question.Home and community-based services help people who need significant assistance live at home as opposed to nursing homes or group homes.
Services can include home visits from nurses or occupational therapists; assistance with personal care such as eating or bathing; help from case managers; attendance at adult day centers; help with cooking, cleaning and other chores; transportation; and home repairs and modifications. It can also help pay for durable medical equipment such as wheelchairs or oxygen tanks.
The need. At some point, 70% of older adults will require help with dressing, hygiene, moving around, managing finances, taking medications, cooking, housekeeping and other daily needs, usually for two to four years. As the nation’s aging population expands to 74 million in 2030 (the year all baby boomers will have entered older age), that need will expand exponentially.
Younger adults and children with conditions such as cerebral palsy, blindness or intellectual disabilities can similarly require significant assistance.
The burden on families. Currently, 53 million family members provide most of the care that vulnerable seniors and people with disabilities require — without being paid and often at significant financial and emotional cost. According to AARP, family caregivers on average devote about 24 hours a week, to helping loved ones and spend around $7,000 out-of-pocket.
This reflects a sobering reality: Long-term care services are simply too expensive for most individuals and families. According to a survey last year by Genworth, a financial services firm, the hourly cost for a home health aide averages $24. Annually, assisted living centers charge an average $51,600, while a semiprivate room in a nursing home goes for $93,075.
Medicare limitations. Many people assume that Medicare — the nation’s health program for 61 million older adults and people with severe disabilities — will pay for long-term care, including home-based services. But Medicare coverage is extremely limited.
In the community, Medicare covers home health only for older adults and people with severe disabilities who are homebound and need skilled services from nurses and therapists. It does not pay for 24-hour care or care for personal aides or homemakers. In 2018, about 3.4 million Medicare members received home health services.
In nursing homes, Medicare pays only for rehabilitation services for a maximum of 100 days. It does not provide support for long-term stays in nursing homes or assisted living facilities.
Medicaid options. Medicaid — the federal-state health program for 72 million children and adults in low-income households — can be an alternative, but financial eligibility standards are strict and only people with meager incomes and assets qualify.
Medicaid supports two types of long-term care: home and community-based services and those provided in institutions such as nursing homes. But only care in institutions is mandated by the federal government. Home and community-based services are provided at the discretion of the states.
Although all states offer home and community-based services of some kind, there’s enormous variation in the types of services offered, who is served (states can set caps on enrollment) and state spending. Generally, people need to be frail enough to need nursing home care to qualify.
Nationally, 57% of Medicaid’s long-term care budget goes to home and community-based services — $92 billion in the 2018 federal budget year. But half of states still spend twice as much on institutional care as they do on community-based care. And 41 states have waiting lists, totaling nearly 820,000 people, with an average wait of 39 months.
Based on the best information available, between 4 million and 5 million people receive Medicaid-funded home and community-based services — a fraction of those who need care.
Workforce issues. Biden’s proposal doesn’t specify how $400 billion in additional funding would be spent, beyond stating that access to home and community-based care would be expanded and caregivers would receive “a long-overdue raise, stronger benefits, and an opportunity to organize or join a union.”
Caregivers, including nursing assistants and home health and personal care aides, earn $12 an hour, on average. Most are women of color; about one-third of those working for agencies don’t receive health insurance from their employers.
By the end of this decade, an extra 1 million workers will be needed for home-based care — a number of experts believe will be difficult, if not impossible, to reach given poor pay and working conditions.
“We have a choice to keep these poverty-wage jobs or make them good jobs that allow people to take pride in their work while taking care of their families,” said Poo of Caring Across Generations.
Next steps.Biden’s plan leaves out many details. For example: What portion of funding should go to strengthening the workforce? What portion should be devoted to eliminating waiting lists? What amount should be spent on expanding services?
How will inequities of the current system — for instance, the lack of accessible services in rural counties or for people with dementia — be addressed? “We want to see funding to states tied to addressing those inequities,” said Amber Christ, directing attorney of the health team at Justice in Aging, an advocacy organization.
Meanwhile, supporters of the plan suggest it could be just the opening of a major effort to shore up other parts of the safety net. “There are huge gaps in the system for middle-income families that need to be addressed,” said David Certner, AARP’s legislative counsel.
Reforms that should be considered include tax credits for caregivers, expanding Medicare’s home health benefit and removing the requirement that people receiving Medicare home health be homebound, said Christ of Justice in Aging.
”We should be looking more broadly at potential solutions that reach people who have some resources but not enough to pay for these services as well,” she said.
Some countries have stockpiles. Others have nothing. Getting a vaccine means living in the right place — or knowing the right people.
A 16-year-old in Israel can get a vaccine.
So can a 16-year-old in Mississippi.
And an 18-year-old in Shanghai.
But a 70-year-old in Shanghai can’t get one. Older people are at high risk for severe illness from Covid-19. But Chinese officials have been reluctant to vaccinate seniors, citing a lack of clinical trial data. Neither can an 80-year-old in Kenya. Low vaccine supply in many countries means only health care employees and other frontline workers are eligible, not the elderly.
Nor a 90-year-old in South Korea. Koreans 75 and older are not eligible until April 1. Only health care workers and nursing-home residents and staff are currently being vaccinated. The government initially said it was awaiting assurances that the AstraZeneca vaccine was safe and effective for older groups.
Anyone in Haiti.
Anyone in Papua New Guinea.
Anyone in these 67 countries. These countries have not reported any vaccinations, according to Our World in Data. Official figures can be incomplete, but many countries are still awaiting their first doses.
It wasn’t supposed to be like this: Covax, the global vaccine-sharing initiative, was meant to prevent unequal access by negotiating vaccine deals on behalf of all participating nations. Richer nations would purchase doses through Covax, and poorer nations would receive them for free.
But rich nations quickly undermined the program by securing their own deals directly with pharmaceutical companies. In many countries, they have reserved enough doses to immunize their own multiple times over.
Anyone who can afford a smartphone or an internet connection in India and is over 60 can get one. Mostly wealthy Indians are being inoculated in New Delhi and Mumbai, hospitals have reported, since vaccine appointments typically require registering online. Less than half of India’s population has access to the internet, and even fewer own smartphones.
And anyone who can pay $13,000 and travel to the U.A.E. for three weeks and is 65 or older or can prove they have a health condition.
A member of Congress in the United States. Friends of the mayor of Manaus, Brazil. Lawmakers in Lebanon. A top-ranking military leader in Spain. The extended family of the deputy health minister in Peru. The security detail to the president of the Philippines. Government allies with access to a so-called “V.I.P. Immunization Clinic” in Argentina. Around the world, those with power and connections have often been first in line to receive the vaccine — or have cut the line altogether.
A smoker in Illinois can get one.But not a smoker in Georgia.
A diabetic in the United Kingdom can. A diabetic in Connecticut can’t.
Countries have prioritized different underlying health conditions, with the majority focusing on illnesses that may increase the risk of severe Covid-19. In the U.S., health issues granted higher priority differ from state to state, prompting some people to travel across state borders.
A pregnant woman in New York.Not a pregnant woman in Germany. Up to two close contacts of a pregnant woman in Germany. Pregnant women were barred from participating in clinical trials, prompting many countries to exclude them from vaccine priority groups. But some experts say the risks to pregnant women from Covid-19 are greater than any theoretical harm from the vaccines.
A grocery worker in Texas, no. A grocery worker in Oklahoma, yes.
Many areas aim to stop the virus by vaccinating those working in frontline jobs, like public transit and grocery stores. But who counts as essential depends on where you live.
A police officer in the U.K. A police officer in Kenya. A postal worker in California. A postal worker in North Carolina. A teacher in Belgium. A teacher in Campeche, Mexico. Other jobs have been prioritized because of politics: Mexico’s president made all teachers in the southern state of Campeche eligible in a possible bid to gain favor with the teacher’s union.
Medical staff at jails and prisons in Colombia. A correctional officer in Tennessee. A prisoner in Tennessee. A prisoner in Florida. The virus spread rapidly through prisons and jails, which often have crowded conditions and little protective equipment. But few places have prioritized inoculating inmates.
An undocumented farm worker in Southern California. A refugee living in a shelter in Germany. An undocumented immigrant in the United Kingdom. Britain has said that everyone in the country is eligible for the vaccine, regardless of their legal status.
A Palestinian in the West Bank without a work permit. Despite leading the world in per-capita vaccinations, Israel has so far not vaccinated most Palestinians, unless they have permits to work in Israel or settlements in the occupied West Bank.
An adult in Bogotá, Colombia. An adult in the Amazonian regions of Colombia that border Brazil. In most of Colombia, the vaccine is only available to health care workers and those over 80.
But the government made all adults in Leticia, Puerto Nariño, Mitú and Inírida eligible, hoping to prevent the variant first detected in Brazil from arriving in other areas. A police officer in Mexico City. A teacher in rural Mexico.The government of populist president Andrés Manuel López Obrador has prioritized vaccinating the poor and those in rural communities, despite the country’s worst outbreaks occurring in major cities.
Native populations not federally recognized in the United States. The pandemic has been particularly deadly for Native Americans. But only tribes covered by the Indian Health Service have received vaccine doses directly, leaving about 245 tribes without a direct federal source of vaccines. Some states, including Montana, have prioritized all Native populations.
Indigenous people living on official indigenous land in Brazil.
These 43 countries, mostly high income, are on pace to be done in a year. These 148 countries, mostly low income, are on pace to take until next year or even longer. Countries like the U.S. continue to stockpile tens of millions of vaccine doses, while others await their first shipments.
“The vaccine rollout has been inequitable, unfair, and dangerous in leaving so many countries without any vaccine doses at all,” said Gavin Yamey, director of Duke University’s Center for Policy Impact in Global Health.
“It’s a situation in which I, a 52-year-old white man who can work from home and has no pre-existing medical conditions, will be vaccinated far ahead of health workers or a high-risk person in a middle- or low-income country.”