The American Hospital Association, the American Medical Association and the American Nurses Association teamed up to release a new “Forever Grateful” TV and digital ad campaign on Monday to thank health care workers.
Why it matters: The campaign comes in the face of record levels of reported health care worker burnout tied, in part, to the prolonged emergency response to COVID-19.
The AHA also released a new video thanking health care professionals working in America’s hospitals and health systems for their work.
Some countries have stockpiles. Others have nothing. Getting a vaccine means living in the right place — or knowing the right people.
A 16-year-old in Israel can get a vaccine.
So can a 16-year-old in Mississippi.
And an 18-year-old in Shanghai.
But a 70-year-old in Shanghai can’t get one. Older people are at high risk for severe illness from Covid-19. But Chinese officials have been reluctant to vaccinate seniors, citing a lack of clinical trial data. Neither can an 80-year-old in Kenya. Low vaccine supply in many countries means only health care employees and other frontline workers are eligible, not the elderly.
Nor a 90-year-old in South Korea. Koreans 75 and older are not eligible until April 1. Only health care workers and nursing-home residents and staff are currently being vaccinated. The government initially said it was awaiting assurances that the AstraZeneca vaccine was safe and effective for older groups.
Anyone in Haiti.
Anyone in Papua New Guinea.
Anyone in these 67 countries. These countries have not reported any vaccinations, according to Our World in Data. Official figures can be incomplete, but many countries are still awaiting their first doses.
It wasn’t supposed to be like this: Covax, the global vaccine-sharing initiative, was meant to prevent unequal access by negotiating vaccine deals on behalf of all participating nations. Richer nations would purchase doses through Covax, and poorer nations would receive them for free.
But rich nations quickly undermined the program by securing their own deals directly with pharmaceutical companies. In many countries, they have reserved enough doses to immunize their own multiple times over.
Anyone who can afford a smartphone or an internet connection in India and is over 60 can get one. Mostly wealthy Indians are being inoculated in New Delhi and Mumbai, hospitals have reported, since vaccine appointments typically require registering online. Less than half of India’s population has access to the internet, and even fewer own smartphones.
And anyone who can pay $13,000 and travel to the U.A.E. for three weeks and is 65 or older or can prove they have a health condition.
A member of Congress in the United States. Friends of the mayor of Manaus, Brazil. Lawmakers in Lebanon. A top-ranking military leader in Spain. The extended family of the deputy health minister in Peru. The security detail to the president of the Philippines. Government allies with access to a so-called “V.I.P. Immunization Clinic” in Argentina. Around the world, those with power and connections have often been first in line to receive the vaccine — or have cut the line altogether.
A smoker in Illinois can get one.But not a smoker in Georgia.
A diabetic in the United Kingdom can. A diabetic in Connecticut can’t.
Countries have prioritized different underlying health conditions, with the majority focusing on illnesses that may increase the risk of severe Covid-19. In the U.S., health issues granted higher priority differ from state to state, prompting some people to travel across state borders.
A pregnant woman in New York.Not a pregnant woman in Germany. Up to two close contacts of a pregnant woman in Germany. Pregnant women were barred from participating in clinical trials, prompting many countries to exclude them from vaccine priority groups. But some experts say the risks to pregnant women from Covid-19 are greater than any theoretical harm from the vaccines.
A grocery worker in Texas, no. A grocery worker in Oklahoma, yes.
Many areas aim to stop the virus by vaccinating those working in frontline jobs, like public transit and grocery stores. But who counts as essential depends on where you live.
A police officer in the U.K. A police officer in Kenya. A postal worker in California. A postal worker in North Carolina. A teacher in Belgium. A teacher in Campeche, Mexico. Other jobs have been prioritized because of politics: Mexico’s president made all teachers in the southern state of Campeche eligible in a possible bid to gain favor with the teacher’s union.
Medical staff at jails and prisons in Colombia. A correctional officer in Tennessee. A prisoner in Tennessee. A prisoner in Florida. The virus spread rapidly through prisons and jails, which often have crowded conditions and little protective equipment. But few places have prioritized inoculating inmates.
An undocumented farm worker in Southern California. A refugee living in a shelter in Germany. An undocumented immigrant in the United Kingdom. Britain has said that everyone in the country is eligible for the vaccine, regardless of their legal status.
A Palestinian in the West Bank without a work permit. Despite leading the world in per-capita vaccinations, Israel has so far not vaccinated most Palestinians, unless they have permits to work in Israel or settlements in the occupied West Bank.
An adult in Bogotá, Colombia. An adult in the Amazonian regions of Colombia that border Brazil. In most of Colombia, the vaccine is only available to health care workers and those over 80.
But the government made all adults in Leticia, Puerto Nariño, Mitú and Inírida eligible, hoping to prevent the variant first detected in Brazil from arriving in other areas. A police officer in Mexico City. A teacher in rural Mexico.The government of populist president Andrés Manuel López Obrador has prioritized vaccinating the poor and those in rural communities, despite the country’s worst outbreaks occurring in major cities.
Native populations not federally recognized in the United States. The pandemic has been particularly deadly for Native Americans. But only tribes covered by the Indian Health Service have received vaccine doses directly, leaving about 245 tribes without a direct federal source of vaccines. Some states, including Montana, have prioritized all Native populations.
Indigenous people living on official indigenous land in Brazil.
These 43 countries, mostly high income, are on pace to be done in a year. These 148 countries, mostly low income, are on pace to take until next year or even longer. Countries like the U.S. continue to stockpile tens of millions of vaccine doses, while others await their first shipments.
“The vaccine rollout has been inequitable, unfair, and dangerous in leaving so many countries without any vaccine doses at all,” said Gavin Yamey, director of Duke University’s Center for Policy Impact in Global Health.
“It’s a situation in which I, a 52-year-old white man who can work from home and has no pre-existing medical conditions, will be vaccinated far ahead of health workers or a high-risk person in a middle- or low-income country.”
The first month of the pandemic was also supposed to be the month I got pregnant, but my clinic closed and plans changed. Doctors and nurses needed personal protective equipment to tend to patients with covid-19, not women with recurrent miscarriages.
When the clinic reopened several months later, it turned out my husband and I had only been delaying yet another loss: In late August, he obeyed the medical center’s strict coronavirus protocols by waiting anxiously in the car while I trudged inside, masked and hand-sanitized, to receive a miscarriage diagnosis alone. I searched the ultrasound screen for the rhythmic beat of a heart, and then accepted that whatever had once been there was now gone.
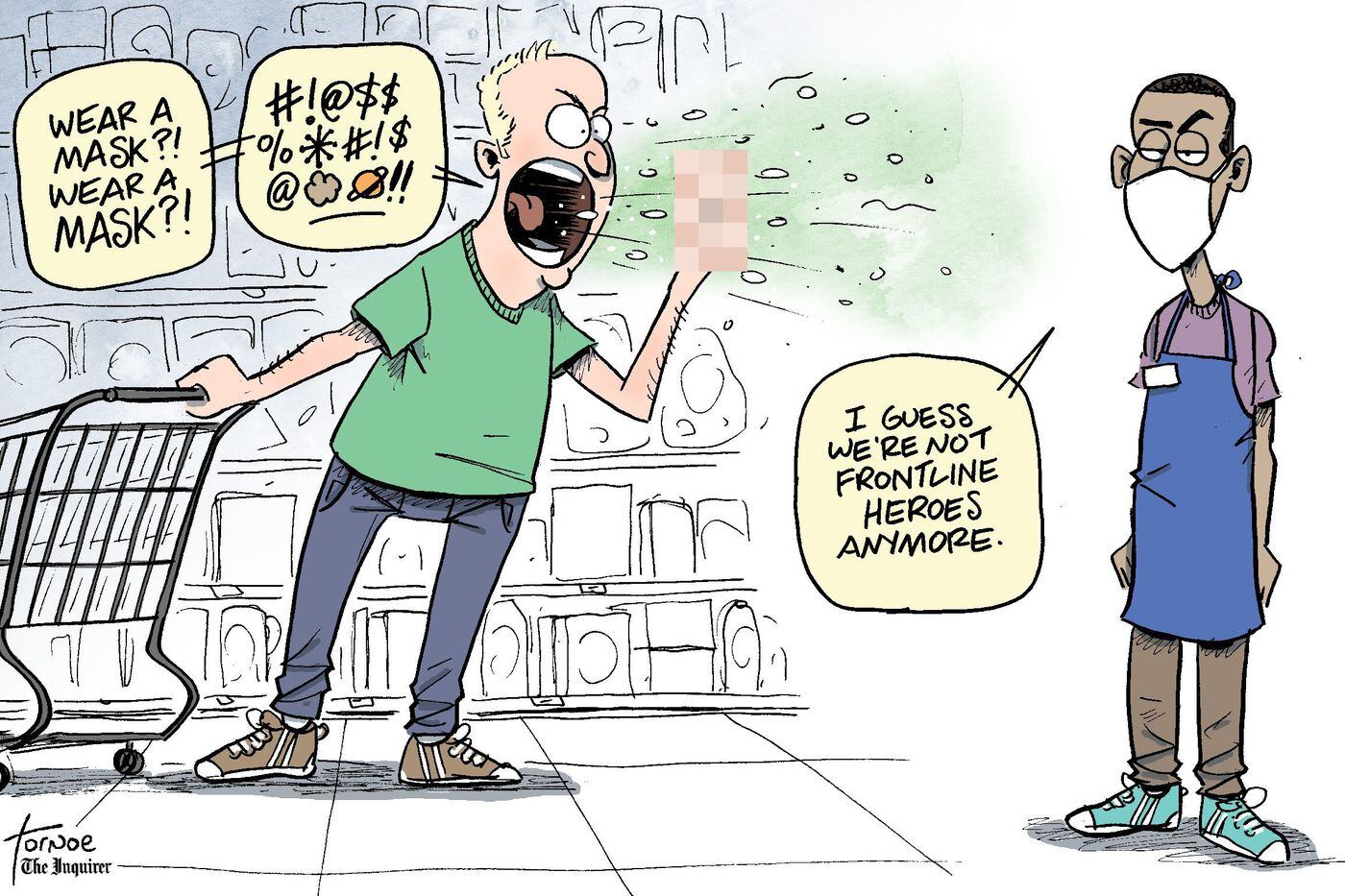
But that was 2020 for you, consistent only in its utter crappiness. For every inspiring video of neighbors applauding a shift change at the hospital, another video of a bone-tired nurse begging viewers to believe covid was real, it wasn’t a hoax, wear a mask.
For every protest organized by activists who understood racism is also a long-term crisis, an appearance by the Proud Boys; for every GoFundMe successfully raising money for a beloved teacher’s hospital bills, a bitter acknowledgment that online panhandling is our country’s version of a safety net.
Millions of citizens stood in line for hours to vote for the next president and then endured weeks of legal petitions arguing that their votes should be negated. The basis for these legal actions were conspiracy theories too wild to be believed, except that millions of other citizens believed them.
And that was 2020 for you, too: accepting the increasingly obvious reality that the country was in peril, built on iffy foundations that now buckled under pressure. My loved ones who worked as waiters or bartenders or physical therapists were choosing between health and paychecks, and even from the lucky safety of my work-from-home job, each day began to feel like watching America itself arrive at a hospital in bad shape, praying that doctors or clergy could find something they were able to save.
Is there a heartbeat?
You want the answer to be yes, but even so, it was hard to imagine how we would come back from this.
What kind of delusional person would even try to get pregnant in this world? In my case it would never be a happy accident; it would always be a herculean effort. And so it seemed I should have some answers.
How do you explain to a future child: Sorry, we can’t fix climate change; we can’t even get people to agree that we should wear masks in grocery stores? How do you explain the frustration of seeing brokenness, and then the wearying choice of trying to fix it instead of abandoning it? How do you say, Love it anyway. You’re inheriting an absolute mess, but love it anyway?
I found myself asking a lot of things like this in 2020, but really they were all variations of the same question: What does it mean to have hope?
But in the middle of this, scientists worked quietly in labs all over the world. They applied the scientific method with extraordinary discipline and speed. A vaccine was developed. Tens of thousands of volunteers rolled up their sleeves and said, Try it out on me.
It was approved, and a nurse from Long Island was the first American televised receiving it. Her name was Sandra Lindsay, an immigrant from Jamaica who had come to the United States 30 years ago and who had spent the last year overseeing critical care teams in back-to-back shifts. She said she had agreed to go first to show communities of color, long abused, brushed-off or condescended to by the medical system, that the vaccine was safe.
Here was hope. And more than that, here was hope from a woman who had more reason than most to be embittered: an exhausted health-care worker who knew too well America’s hideous racial past and present, who nonetheless also knew there was only one way out of the tunnel. Here she was, rolling up her own sleeve, and there were the lines of hospital employees ready to go after her, and there were the truck drivers ferrying shipments of syringes.
I can’t have been the only person to watch the video of those early inoculations, feeling elated and tired, and to then burst into tears. I can’t have been the only person to realize that even as 2020 revealed brokenness, it also contained such astounding undercurrents of good.
The scientific method works whether you accept it or not. Doctors try to save you whether you respected public-health guidelines or not. Voter turnout was astronomical because individual citizens realized they were all, every one of them, necessary pieces in a puzzle, even if they couldn’t see what the final picture was supposed to look like.
The way to believe in America is to believe those things are passed down, too.
Sometime in October, a couple of months after my last miscarriage — when the country was riding up on eight months of lonely and stoic birthdays, graduations, deaths and weddings — I went into the bathroom and saw a faint second line on a First Response pregnancy test. It was far from my first rodeo, so I knew better than to get excited. I mentioned it to my husband with studied nonchalance, I told him that I’d test again in a few days but that we should assume the worst would happen.
Two weeks after that, I had a doctor’s appointment, and then another a week later, each time assuming the worst, but each time scheduling another appointment anyway, until eventually I was further along than I’d ever gotten before — by one day, then three days, then thirty.
I am not a superstitious person. I don’t believe that good things always come to those who deserve them. I believe that stories regularly have sad endings and that it’s often nobody’s fault when they do, and that we should tell more stories with sad endings so that people who experience them know that they’re not alone.
But 2020 has taught me that I am, for better or worse, someone who wants to hope for things. To believe in the people who developed vaccines. In the people who administered them. In Sandra Lindsay. In the people who delivered groceries, who sewed masks, who have long cursed America’s imperfect systems and long fought to change them, who still donate $10 to a sick teacher’s GoFundMe.
At my most recent appointment, the doctor’s office was backed up in a holiday logjam. I sat in the exam room for nearly three hours while my husband again waited anxiously in the car. I texted him sporadic updates and tried to put hope in a process that so far had not seemed to warrant my hope.
It all felt precarious. The current reality always feels precarious.
And yet there we all are together, searching for signs of life, hoping that whatever we emerge to can be better than what we had before, and that whatever we build will become our new legacy. The sonographer finally arrived and turned on the machine.
While it sometimes seems like the coronavirus has been with us forever, it’s worth remembering that there are still parts of the country that are only now experiencing their first big spike in cases—that’s the nature of a “patchwork” pandemic working its way across a vast country.
One of our health system members in the Midwest, with whom we recently spent time, is in just this situation: they’re seeing their highest inpatient COVID census to date, just this month. As they shared with us, there are advantages and drawbacks to being a “late follower” on the epidemic curve. The good news is that they’re ready.
Back in March, like most systems, they stood up an “incident command center”, and began preparing for a wave of COVID patients, designating a floor of the hospital as a “hot zone”, creating negative pressure rooms, cross-training staff, developing treatment protocols, stockpiling protective equipment, and securing a pipeline of critical therapeutics and testing supplies. There was a moderate but manageable number of cases across the late spring and summer, but never to an extent that stressed the system.
Eventually, recognizing that they couldn’t ask their doctors, nurses, and administrators to stay on high alert indefinitely, they “stood down” to a more normal operational tempo, only to watch with dismay as the surrounding community seemingly forgot about the virus, and lessened precautions (masking, distancing, and so forth), wanting life to return to “normal”. And now, the post-Labor Day, post-return-to-school spike has arrived.
The challenge now is getting everyone, inside and outside the system, to stop talking about COVID in the past tense, as though they’ve already “gotten through it.”The preparations they’ve made are paying off now. Hospital operations continue to run smoothly even with a high COVID census, but the workforce is exhausted, and citizens aren’t stepping outside to bang gratefully on pots every night anymore.
Asking the team to return to war footing is no easy task, given the fatigue of the past seven months. A question looms: what is the trigger to restart “incident command”? As cases begin to increase again in some of the original COVID hot spots—New York, New England, the Pacific Northwest—healthcare leaders there will need to learn from the experiences of their colleagues in the newly-hit Midwest, about how to take an already virus-weary clinical workforce back onto the battlefield.
Those on the front lines of the fight against the novel coronavirus worry about keeping themselves, their families and their patients safe.
This story is part of a series examining the state of healthcare six months into the public health emergency declared for COVID-19.
There’s no end in sight for the country as it grapples with another surge of COVID-19 cases.
That’s especially true for nurses seeking the reprieve of their hospitals returning to normal operations sometime this year. Many in the South and West are now treating ICUs full of COVID-19 patients they hoped would never arrive in their states, largely spared from spring’s first wave.
And like many other essential workers, those in healthcare are falling ill and dying from COVID-19. The total number of nurses stricken by the virus is still unclear, though the Centers for Disease Control and Prevention has reported 106,180 cases and 552 deaths among healthcare workers. That’s almost certainly an undercount.
National Nurses United, the country’s largest nurses union, told Healthcare Dive it has counted 165 nurse deaths from COVID-19 and an additional 1,060 healthcare worker deaths.
Safety concerns have ignited union activity among healthcare workers during the pandemic, and also given them an opportunity to punctuate labor issues that aren’t new, like nurse-patient ratios, adequate pay and racial equality.
At the same time, the hospitals they work for are facing some of their worst years yet financially, after months of delayed elective procedures and depleted volumes that analysts predict will continue through the year. Many have instituted furloughs and layoffs or other workforce reduction measures.
Healthcare Dive had in-depth conversations with three nurses to get a clearer picture of how they’re faring amid the once-in-a-century pandemic. Here’s what they said.
Elizabeth Lalasz, registered nurse, John H. Stroger Hospital in Chicago
Elizabeth Lalasz has worked at John H. Stroger Hospital in Chicago for the past 10 years. Her hospital is a safety net facility, catering to those who are “Black, Latinx, the homeless, inmates,” Lalasz told Healthcare Dive. “People who don’t actually receive the kind of healthcare they should in this country.”
Data from the CDC show racial and ethnic minority groups are at increased risk of getting COVID-19 or experiencing severe illness, regardless of age, due to long-standing systemic health and social inequities.
CDC data reveal that Black people are five times more likely to contract the virus than white people.
This spring Lalasz treated inmates from the Cook County Jail, an epicenter in the city and also the country. “That population gradually decreased, and then we just had COVID patients, many of them Latinx families,” she said.
Permission granted by Elizabeth Lalasz
Once Chicago’s curve began to flatten and the hospital could take non-COVID patients, those coming in for treatment were desperately sick. They’d been delaying care for non-COVID conditions, worried a trip to the hospital could risk infection.
A Kaiser Family Foundation poll conducted in May found that 48% of Americans said they or a family member had skipped or delayed medical care because of the pandemic. And 11% said the person’s condition worsened as a result of the delayed care.
When patients do come into Lalasz’s hospital, many have “chest pain, then they also have diabetes, asthma, hypertension and obesity, it just adds up,” she said.
“So now we’re also treating people who’ve been delaying care. But after the recent southern state surges, the hospital census started going down again,” she said.
Amy Arlund, registered nurse, Kaiser Permanente Medical Center in Fresno, California:
Amy Arlund works the night shift at Kaiser Fresno as an ICU nurse, which she’s done for the past two decades.
She’s also on the hospital’s infection control committee, where for years she’s fought to control the spread of clostridium difficile colitis, or C. diff., in her facility. The highly infectious disease can live on surfaces outside the body for months or sometimes years.
The measures Arlund developed to control C. diff served as her litmus test, as “the top, most stringent protocols we could adhere to,” when coronavirus patients arrived at her hospital, she told Healthcare Dive.
But when COVID-19 cases surged in northern states this spring, “it’s like all those really strict isolation protocols that prior to COVID showing up would be disciplinable offenses were gone,” Arlund said.
Widespread personal protective equipment shortages at the start of the pandemic led the CDC and the Occupational Safety and Health Administration to change their longstanding guidance on when to use N95 respirator masks, which have long been the industry standard when dealing with novel infectious diseases.
The CDC also issued guidance for N95 respirator reuse, an entirely new concept to nurses like Arlund who say those changes go against everything they learned in school.
“I think the biggest change is we always relied on science, and we have always relied heavily on infection control protocols to guide our practice,” Arlund said. “Now infection control is out of control, we can no longer rely on the information and resources we always have.”
In Arlund’s ICU, she’s taken care of dozens of COVID positive patients and patients ruled out for coronavirus, she said. After a first wave in the beginning of April, cases dropped, but are now rising again.
Other changing guidance weighing heavily on nurses is how to effectively treat coronavirus patients.
“Are we doing remdesivir this week or are we going back to the hydroxychloroquine, or giving them convalescent plasma?”Arlund said. “Next week I’m going to be giving them some kind of lavender enema, who knows.”
Erik Andrews, registered nurse, Riverside Community Hospital in Riverside, California:
Erik Andrews, a rapid response nurse at Riverside Community Hospital in California, has treated coronavirus patients since the pandemic started earlier this year. He likens ventilating them to diffusing a bomb.
“These types of procedures generate a lot of aerosols, you have to do everything in perfectly stepwise fashion, otherwise you’re going to endanger yourself and endanger your colleagues,” Andrews, who’s been at Riverside for the past 13 years, told Healthcare Dive.
He and about 600 other nurses at the hospital went on strike for 10 days this summer after a staffing agreement between the hospital and its owner, HCA Healthcare, and SEIU Local 121RN, the union representing RCH nurses, ended without a renewal.
The nurses said it would lead to too few nurses treating too many patients during a pandemic. Insufficient PPE and recycling of single-use PPE were also putting nurses and patients at risk, the union said, and another reason for the strike.
But rapidly changing guidance around PPE use and generally inconsistent information from public officials are now making the nurses at his hospital feel apathetic.
“Unfortunately I feel like in the past few weeks it’s gotten to the point where you have to remind people about putting on their respirator instead of face mask, so people haven’t gotten lax, but definitely kind of become desensitized compared to when we first started,” Andrews said.
Permission granted by Erik Andrews
With two children at home, Andrews slept in a trailer in his driveway for 12 weeks when he first started treating coronavirus patients. The trailer is still there, just in case, but after testing negative twice he felt he couldn’t spend any more time away from his family.
He still worries though, especially about his coworkers’ families. Some coworkers he’s known for over a decade, including one staff member who died from COVID-19 related complications.
“It’s people you know and you know that their families worry about them every day,” he said. “So to know that they’ve had to deal with that loss is pretty horrifying, and to know that could happen to my family too.”