American Hospitals is the fourth in a series of documentaries produced by the Unfinished Business Foundation, founded by Richard Master, CEO of MCS Industries Inc., who took a deep dive into the economics of the U.S. health-care system after his company was hit year after year with double-digit health insurance rate increases.
Master teamed up with filmmaker Vincent Mondillo to produce Fix It: Healthcare at the Tipping Point; Big Pharma: Market Failure; Big Money Agenda: Democracy on the Brink, and now, American Hospitals.
A provocative look at the cost and inequities of American Hospitals, often more motivated by money and power than in providing for the health needs of individuals and the communities they were founded to serve. From the filmmakers behind the hit documentaries Fix It: Healthcare at the Tipping Point, Big Money Agenda, and Big Pharma.
Learn more and find out where to see the latest film at fixithealthcare.com/events
Last Friday, the Centers for Medicare and Medicaid Services (CMS) announced that it will begin phasing in major Medicare Advantage (MA) risk-adjustment changes over a three-year period, slower than previously anticipated. Thanks to this delay in full implementation, MA plans will see an average 3.3 percent payment increase in 2024, up from the one percent projected in the earlier draft notice.
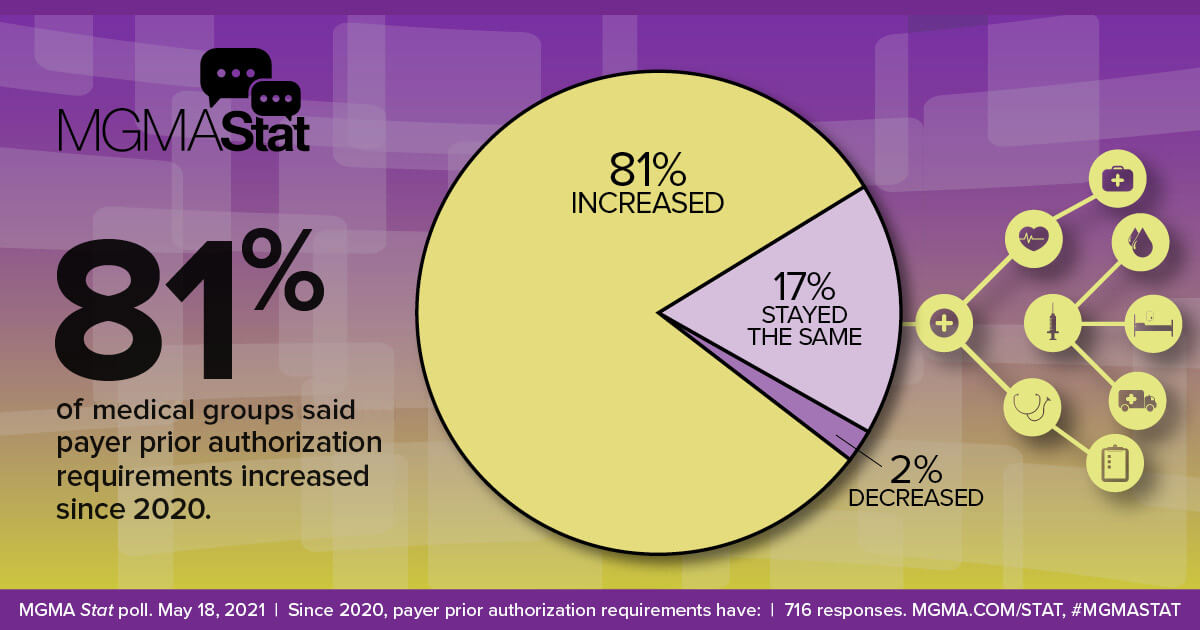
CMS also finalized regulations this week that aim to limit MA prior authorizations and denials by requiring that coverage decisions align with traditional Medicare.
The Gist: After CMS began proposing changes to MA payment formulas last year, aimed at reining in pervasive abuses and fraud,
the insurance industry responded with a $13M marketing blitz to oppose the changes.
The ads, one of which aired during the Super Bowl, tied Medicare Advantage “cuts” to the time-tested “Hands Off My Medicare” messaging directed at seniors.
With MA enrollment projected to overtake traditional Medicare this year,the federal government finds itself walking a tightrope in clamping down on overpayments to MA plans, given that any reductions will impact a growing number of seniors.
Constrained by the Affordable Care Act’s medical loss ratio (MLR) requirement that health insurers must spend 80-85 percent of their revenue on medical services, payers have been pivoting to providing care, managing pharmacy benefits, and supporting other healthcare services, in order to fuel earnings growth. The graphic above shows why UnitedHealth Group (UHG) is seen as the health insurance industry’s most noteworthy model of this vertical integration strategy, thanks to its flourishing Optum division.
Optum is now as big a profit driver for UHG as its UnitedHealthcare insurance arm, with each bringing in $14B of net earnings in 2022.
Optum’s 7.7 percent operating margin is almost two points higher than UnitedHealthcare’s, which owes much of its revenue and earnings growth to its expanding Medicare Advantage (MA) business. As both sides of UHG’s business have grown, so too have intercompany eliminations, which have increased by over 80 percent in five years, reaching $108 billion in 2022. These payments from one division of UHG to another—mostly from the insurance business to the provider arm—allow the company to shift profit-capped insurance revenues into other divisions, driving increased profitability for the overall enterprise.
It will be worth watching the trend in intercompany eliminations at other vertically integrated insurance companies, with an eye for whether integration truly results in lower cost of care for patients or just higher margins for the insurers.
Jaime King On Consolidation and Competition — The Trials and Triumphs of Health Care Antitrust Law New England Journal of Medicine March 18, 2023; 388:1057-1060 DOI: 10.1056/NEJMp2201629
“Over the past 30 years, health care consolidation has gone largely unchecked by federal and state antitrust enforcers, which has resulted in higher prices, stagnant quality of care, and limited access to care for patients. Similarly, consolidation has contributed to the availability of fewer employment options, limited wage growth, longer hours, and staff shortages for health care providers.
Antitrust law is designed to prevent such harms, but its failure to evolve alongside the health care industry has led to pervasive consolidation, which now necessitates regulation in some markets to address market-power abuses that competitive forces can no longer govern…
Although mergers are often justified with promises of improved quality or patient access, evidence supporting these claims is lacking.
Clinical integration as envisioned in accountable care organizations, for example, requires substantial oversight, training, and investment that goes well beyond the financial integration involved in most mergers. Most studies have found either no changes or a reduction in quality after provider mergers. Consolidation can also limit access to care; post-merger facility closures, reductions in charity care, and elimination of abortion and other reproductive health services have often occurred.
Consolidation among insurers also affects health care prices and quality. Insurers with market power can increase premiums above competitive levels by exercising monopoly power or can push provider payments below competitive levels by exercising monopsony power. Lower premiums are commonly found in areas with more insurers, whereas in the absence of competition, insurers that obtain price concessions from providers may not pass savings on to consumers.4 Some evidence suggests, however, that moderate amounts of insurer consolidation may be associated with improved patient experience, since providers in such markets have an incentive to compete on quality.
Given the health care industry’s growing complexity, future oversight could involve a combination of more responsive antitrust enforcement and creative regulatory interventions. Combining competitive and regulatory forces may offer the only hope for controlling health care prices, restoring high-quality care, protecting health care workers, and preserving and expanding access to care.”
On Wednesday, UnitedHealth Group (UHG) announced that it will reduce its prior authorization claims volume by 20 percent for its commercial, Medicare Advantage, and Medicaid businesses later this year. Next year, it will launch a “gold card” program for qualifying providers that will further streamline care approvals. Cigna also shared that it has removed nearly 500 services from prior authorization review since 2020, relying on an electronic process for faster response times. These changes come in the wake of a Centers for Medicare and Medicaid Services (CMS) proposed rule, set to be finalized in April, that aims to streamline prior authorization by requiring certain payers to establish a method for electronic transmission, shorten response time for physician requests, and provide a reason for denials.
The Gist: These changes address two of providers’ primary complaints around prior authorizations: there are too many of them, and payers take too long to process them. However, technology options aiming to solve this problem through automation are by no means a foolproof solution.
As ProPublica recently reported, algorithm-based electronic claims processing solutions that improve response times can create other challenges, including improper automatic denials, and can expand prior authorization to lower-cost services, for which it was previously determined to be inefficient to rely on human review. Quicker responses must still be accurate and fair, necessitating that insurance companies closely monitor, audit, and hone technology solutions.
A recent Urban Institute report highlights the issue of medical debt but fails to examine two of the chief driving forces of this debt: inadequate enrollment in comprehensive health care coverage and high-deductible health plans that intentionally push more costs onto patients. It also fails to appreciate the looming crisis when the public health emergency ends and Medicaid enrollment could plummet.
As the extent of medical debt shows, both the government and the private market is failing too many patients, leaving too many either uninsured or with subpar plans that expose too many people to bills they cannot afford to pay. While hospital financial assistance is crucial to helping many individuals of limited means access care, it is no substitute for a solution that gets to the root causes of medical debt.
Affordable, comprehensive health care coverage is the most important protection against medical debt. While the U.S. health care system has achieved record rates of coverage, significant gaps remain and new threats are on the horizon. One of the gaps is the failure by some states to expand Medicaid, while the most imminent threat is the potential loss of Medicaid coverage for millions of people as the public health emergency ends. We must ensure that every individual has access to some form of comprehensive coverage.
In doing so, we must put an end to deceptively inadequate health plans. These include short-term limited duration health plans and health sharing ministries that often appeal to consumers because they are cheaper and often marketed to appear comprehensive. The reason they are cheaper is because when you read the fine print you discover they cover fewer benefits and include few-to-no consumer protections, like required coverage of pre-existing conditions and limits on out-of-pocket costs. Subscribers for these types of plans often find themselves responsible for their entire medical bill without any help from their health plan and can accumulate significant medical debt.
Many of the same concerns apply to high-deductible health plans. These plans are specifically designed to increase patients’ financial exposure through high cost-sharing – the amount the subscriber must pay out-of-pocket. Yet, many individuals enrolled in these plans find they can’t manage the gap between what their insurance pays and what they themselves owe as a result. It’s not a mystery why high-deductible health plans contribute to medical debt.
Hospitals and other providers do not determine how much insured patients owe for their care. Instead, that amount is set by the health plan. While every hospital has a financial assistance policy to help those most in need, they can only help so much and so many. And no matter how generous, hospital financial assistance will never be a substitute for a health plan that covers preventive and necessary care at an affordable price on the front and back end of coverage.
We must tackle the problem of medical debt, and we must do so at the root: ensuring all individuals are enrolled in comprehensive health care coverage and ending deceptive marketing of health plans and unaffordable cost-sharing.
Potential solutions include:
Restricting the sale of high-deductible health plans to only those individuals with the demonstrated means to afford the associated cost-sharing.
Prohibiting the sale of health sharing ministry products and short-term limited duration plans that go longer than 90 days.
Lowering the maximum out-of-pocket cost-sharing limits.
Eliminating the use of deductibles and co-insurance and rely solely on flat co-payments, which are easier for patients to anticipate.
Removing providers from the collection of cost-sharing altogether and require that health plans collect directly from their enrollees the cost-sharing payments they impose. This approach would eliminate the vast majority of patient bills from providers altogether.
Moreover, the AHA has been actively engaged in identifying and promoting best practices in patient billing for decades. The AHA updated our voluntary patient billing guidance in 2020. The guidelines include assisting patients who cannot pay for the care they receive and protecting patients from certain debt collection practices, such as garnishment of wages, liens, interest on debt, adverse credit reporting and lawsuits. Most hospitals provide free care for patients with the most limited means as defined by income below 200% of the federal poverty limit. In the event of an unpaid bill, the Internal Revenue Service has prescribed an extensive series of steps and wait times that most hospitals must adhere to before taking any collection actions, which is a last resort.
Hospitals’ doors are always open to anyone who needs care, regardless of ability to pay. In total, hospitals and health systems of all types provided in 2020 more than $42 billion in uncompensated care, or care for which they received no payment.
Hospitals and health systems will continue to work to advance solutions that make care more affordable and accessible for all patients. But health plans must do their part by providing adequate coverage that does not subject patients to unaffordable bills and medical debt.
The health of a community is measured by the health of its individual members, and the health of its members depends on their access to local, high-quality medical care. Health coverage is a key indicator of the health and wellness of an individual. When people have health insurance, they have greater access to care, reduced mortality, and better health outcomes, according to a report from the American Hospital Association.
However, the current approach taken by some of the nation’s largest health insurers, or payers, is putting this at jeopardy as payers focus on profits and quarterly earnings, strip rates and put the long-term viability of health systems at risk. With hospitals in the middle of the worst economic performance in decades, it is time for payers to own up to how their actions negatively impact the communities and those they claim to serve.
As a physician and the chief of population health at a large metro-area health system, Northeast Georgia Health System, my patients’ ability to readily access medical care at our facilities — and have that care be covered by insurance — matters greatly. Any disruption in a patient’s experience, such as restricting access to care by their health plan or going out of network with an insurance company, can wreak havoc on population health. It’s no secret that many health systems across the country have felt the weight of increased administrative and contractual burdens from health insurers as denial rates continue to creep upwards.
Health insurance companies, like the nation’s largest, UnitedHealthcare, have seen profits soar in recent years. UnitedHeatlhcare’s profits were up 28 percent during the third quarter of 2022 – achieving a profit of $5.3 billion in just those three months – before closing the year at $28.4 billion in net earnings in 2023. Elevance (formerly Anthem), Cigna, and Aetna have also posted record profits recently.
We have seen the impact of the pressure payers are putting on hospitals across the country. Nearly 200 hospitals have closed since 2005, according to the Sheps Center for Health Services Research at the University of North Carolina. Many of these hospitals have closed because they failed to receive fair contracted rates from large payers and thus were insolvent.
Community benefits like charity care, health education and economic impact are provided by hundreds of hospitals nationally, but that impact is at risk if they are not fairly compensated for the services they provide.
A health insurer launched a pilot program that takes aim at food insecurity in addressing the healthcare needs of beneficiaries—the first time that’s ever happened, according to those who spearheaded the effort.
Kaiser Permanente and Geisinger Health Plan have also used a food-as-medicine approach in attempting to improve health outcomes, but here’s the difference: They are integrated health systems that own their own hospitals and physician practices, while Blue Cross and Blue Shield of North Carolina is not.
Blue Cross NC unveiled data published in NEJM Catalyst about its proof-of-concept pilot program that involved delivering food to individuals in Affordable Care Act plans who suffer from Type 2 diabetes as well as connecting them with health advisers. Despite the success of the effort, the findings included many caveats that suggest that it could be some time before the pilot program evolves and lands a spot on the insurer’s roster of benefits packages.
Still, the authors called it a good first step that underscores great potential.
They also noted that “payers are in a unique position to integrate food-as-medicine interventions into more sustainable financial models. As a payer, the business case needs to be made for offering products and services that address the food and nutritional needs of its members.”
More than 600,000 North Carolina residents struggle to put food on the table, with the state ranking as the tenth hungriest in the country. The pilot’s results come at a time when the expansion of food-aid programs because of the COVID-19 pandemic has run out and inflation is driving up the price of groceries.
Blue Cross NC’s program was launched in December 2020, and invitations to eligible beneficiaries were sent out in January 2021. The insurer hired the digital health coaching vendor Pack Health, a division of Quest Diagnostics, to help administer the program.
A typical box of food could include salmon, carrots, beans, rice, pasta, sauce, applesauce, milk and crushed tomatoes. Deliveries included easy-to-make recipes, according to the study.
Blue Cross NC researchers compared the results of surveys at three and six months to baseline metrics. The surveys measured physical and mental health, body mass index, hemoglobin A1c levels, self-reported food security and member satisfaction.
They also looked at medical expenses for the 555 “completes,” those who finished the program, and the 327 “partials.” Completes received 12 boxes of food and six months of coaching. Partials received six to 11 boxes of food and three to five months of coaching but dropped out of the program.
Most participants (81%) were satisfied with the frequency of food delivery as well as the amount of food delivered (82%).
Food insecurity for the completes dipped from 38% to 20%, BMI (35 kg/m2 to 33 kg/m2) and obesity (72% to 61%). Completes saw an increase in individuals who reached the U.S. average for physical health measures (51% to 65%) and mental health measures (70% to 80%).
In addition, completes saw a $139 reduction per member per month in total medical costs and an increase of $8 per member per month in pharmacy costs, which the researchers interpreted as evidence of greater medication adherence.
Partials, meanwhile, saw a decrease of $10 per member per month in pharmacy costs, but an increase in all other cost types.
“The relative number of partials responding to the 3- and 6-month surveys was low; therefore, we do not discuss the 6-month results of this group, nor do we attempt to draw meaningful conclusions regarding differences across participation groups,” the study said.
Nonetheless, researchers estimate that if the program becomes available to all eligible beneficiaries, it could cut medical expenses by as much as $8.5 million to $13.1 million a year.
“These findings highlight that an upfront investment by an insurer can help improve health outcomes,” according to a Blue Cross NC spokesperson. “The food delivery and health coaching pilot program is one of a series focused on long-term strategies for eliminating health disparities, strengthening communities and making health care more affordable, accessible and easier to navigate for all North Carolinians.”
In April 2021, the health plan unveiled partnerships with state organizations including Benefits Data Trust, Manna Food Bank, Food Bank of Central & Eastern North Carolina and Second Harvest Food Bank of Northwest NC that focused on trying to boost enrollment in the Supplemental Nutrition Assistance Program.
“With an initial focus on food security, the insurer is advancing its work to promote health equity with new prevention programs and value-added services,” Blue Cross NC said in a statement at the time. “Beyond just offering these services for members, the insurer is also measuring their impact. This research will identify which steps will be effective long-term strategies for eliminating health disparities, strengthening communities, developing impactful member products, and reducing health care costs for North Carolinians.”
Researchers also note that the results from its food delivery and health coaching program published in NEJM Catalyst are far from conclusive, and further study needs to be done.
“Because all program participants received health coaching, the design makes it impossible to disentangle the effects of the food delivery component from those of the health coaching,” the study states. “Interaction with the [health adviser] was regular, with program participants and [health advisers] communicating at least once per week by telephone and six to seven times per week via text message.”
In addition, researchers want to evaluate whether the gains seen in a six-month period could be sustained over the long haul and what effect greater member participation might have on the program’s sustainability.
“Analyses are planned to evaluate the long-term impact of the … program,” the study states.
In last week’s graphic, we showed how the nation’s largest health insurance companies earn annual revenues several times greater than the largest health systems. In the graphic above, we unpack the 2022 revenue of five of the largest payers, to show just how diversified they have become.
UnitedHealth Group (UHG) continues to lead the way not only as the largest US payer, but also the most vertically integrated, growing its OptumCare provider business by over 30 percent last year.
Playing catch-up, the other payers have also shown willingness to spend large sums on provider acquisitions, with CVS dropping nearly $20B on primary care company Oak Street and home health company Signify last year. UHG and Humana also recently spent over $5B each, on their own home health companies, in pursuit of lower cost settings for treating their Medicare Advantage enrollees.
In contrast, Cigna and Elevance have not been as active in the M&A space of late, prompting Cigna investors to question the CEO on whether the company may be at a competitive disadvantage. We’d expect the race to create full-stack, vertically integrated healthcare platforms, of the kind illustrated by these large payers, to gain steam across the rest of 2023 and beyond. Looming even larger than UHG, CVS Health, and the like: Amazon and Walmart, both of which are actively pursuing their own platform visions in healthcare.
The deal, first announced in March 2022, will bring LHC’s home health locations, hospice sites, and long-term acute care hospitals across 37 states into UHG’s Optum division. LHC also has over 400 joint-venture arrangements with hospitals. The acquisition received heightened scrutiny from antitrust regulators, but was ultimately allowed to proceed.
The Gist: LHC’s postacute footprint expands UHG’s Medicare Advantage value play, guaranteeing postacute capacity and providing a platform to funnel care into lower-cost settings.
UHG’s strategy is right in line with its peers: Humana fully owns home health provider Kindred at Home (now branded CenterWell Home Health), and CVS Health plans to acquire Signify Health, which provides home care services with an emphasis on risk scoring. But achieving lower cost of care will require integration of postacute referrals and care management across rapidly expanding physician networks.