The healthcare industry has made some strides in the “journey to value” across the last decade, but in reality, most health systems and physician groups are still very much entrenched in fee-for-service incentives.
While many health plans report that significant portions of their contract dollars are tied to cost and quality performance, what plans refer to as “value” isn’t necessarily “risk-based.”
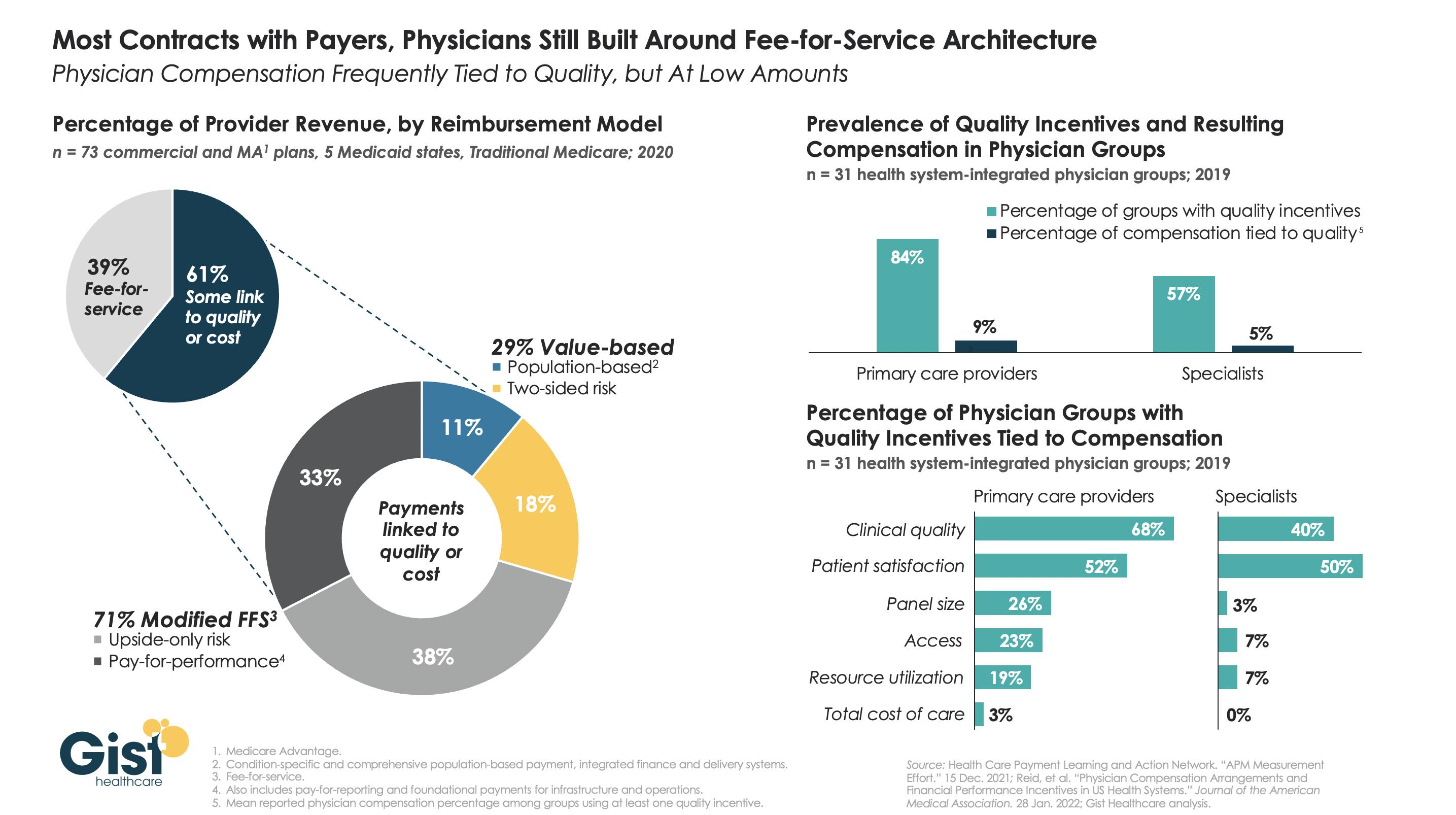
The left-hand side of the graphic below shows that, although a majority of payer contracts now include some link to quality or cost, over two-thirds of those lack any real downside risk for providers.
Data on the right show a similar parallel in physician compensation. Whilethe majority of physician groups have some quality incentives in their compensation models, less than a tenth of individual physician compensation is actually tied to quality performance.
Though myriad stakeholders, from the federal government to individual health systems and physician groups, have collectively invested billions of dollars in migrating to value-based payment over the last decade, we are still far from seeing true, performance-based incentives translate into transformation up and down the healthcare value chain.
“Follow the money,” was the advice of Deep Throat to the Watergate journalists. But now, new Federal Trade Commission Chair Lina Khan says that’s not enough when analyzing monopolies in both healthcare and rest of the economy. Follow the algorithms and follow the power, too, not just the money.
We all know how monopolies harm consumers with higher prices. But monopolies and powerful corporations cause harm in other ways. Some examples:
Facebook using algorithms that “wire” teenage girls to engage with it (and boost Facebook’s profits) but “probably” hurt their mental health
Remington Arms baiting insecure men to buy guns as a badge of masculinity, with tragic results in the case of the Sandy Hook mass murder.
Not all of these examples are linked directly to potentially illegal anticompetitive activities. But all are linked to the exercise of insufficiently checked corporate power. Commissioner Khan has signaled that she will consider such harms when analyzing mergers and other potentially anticompetitive activities.
This expanded view of anticompetitive harm is a departure from Robert Bork’s more narrow approach to antitrust enforcement taken by the F.T.C. since publication of Bork’s 1978 book The Antitrust Paradox. Bork noted that in many cases, mergers resulted in economies of scale that lowered prices for consumers. By his standard, such mergers were permissible as benefiting the consumer.
But now Commissioner Khan – and others like-minded theorists called neo-Brandeisians – point to the other harmful effects beyond the seeming benefit of lower prices. For example, the flip-side of a monopoly’s position as seller is its monopsony as a purchaser of labor. If there is only one big potential employer, workers do not have a competitive labor market, depressing their bargaining power and wages. In the digital economy there is also potential jeopardy to data privacy and security, and coercion to use certain digital products. Think the teenage girls on Instagram.
Employees of a single powerful employer are also inhibited from rocking the boat with innovations, critiques, or whistleblowing. This enervates a truly competitive marketplace.
Commissioner Khan views the antitrust issue not as being one of bigness but rather of power, power that reduces true competition. Beyond merely looking at prices, she seeks to identify and quantify the other elements of power and competition.
This blog has implicated healthcare monopolies as one direct cause of relentless increases in spending. It has also embraced the view of Steven Brill that “over the last five decades a new ‘best and brightest’ meritocracy rigged not only healthcare, but also the entire American financial, legal, and political system to build ‘moats’ of protection to perpetuate their wealth and power.”
Commissioner Khan is now highlighting a key mechanism – anticompetitive political and financial power — by which healthcare corporations rig healthcare and by which other corporations have blocked reform in pursuit of short-sighted profits. She summarizes the remedy:
If you allow unfettered monopoly power to concentrate, its power can rival that of the state., right? And historically, the antitrust laws have a rich tradition and rich history, and a key goal was to ensure that our commercial sphere was characterized by the same types of checks and balances and protections against concentration of economic power that we had set up in our political and governance sphere. And so the desire to kind of check those types of concentrations of power, I think, is deep in the American tradition.
A recent New Yorker article details the history of the American Medical Association’s (AMA) opposition to single-payer healthcare, and the grassroots movement that nearly changed its position in 2019.
Since its founding in the 1840s, the largest association of the nation’s doctors has wielded significant influence over healthcare policy, and has been the most effective opponent of several waves of progressive healthcare reform proposals across the last century. More recent changes in the demographic makeup of its physician constituents have begun to mirror the US population. A quarter of today’s practicing physicians graduated from foreign medical schools, and gender and racial gaps in medical schools have been reduced. Today, half of medical students are female, and half are people of color.
The Gist: The perspectives, needs, and politics of the physician community are changing. Younger physicians tend to be more left-leaning, and more are employees, rather than entrepreneurial business owners. While physician pocketbook issues historically dominated the AMA’s policy positions, today’s younger physicians are increasingly motivated by social justice concerns, leading to advocacy positions that would have been unimaginable a few decades ago.
Physician societies continue to move closer to endorsing more extensive healthcare reform policies, over trying to ensure economic protection for the profession—and in the long run, this shift in physician support could prove a key driver in increasing public approval of “Medicare for All” and other coverage reforms.
The California Assembly is poised to vote on a bill Jan. 31 that aims to create a single-payer healthcare system in the state — the bill’s first major battle since a funding proposal for the program was introduced Jan. 6 — according to KTVU FOX 2.
The state’s plan to create a universal healthcare system involves two bills — AB 1400 and ACA 11 — that would implement and subsequently fund the program, dubbed CalCare. The Assembly is expected to only vote on AB 1400 on Jan. 31.
The Assembly must pass the bill Jan. 31 if it hopes to pass the single-payer framework bill by the end of the year. If the bill passes in the Assembly, it would then need approval in the Senate and from voters.
The plan is being met with public pressure that believesthe system would “create a new and exorbitantly expensive government bureaucracy.” Lawmaker opposition also largely focuses on the bill’s cost, which would be between $314 billion and $391 billion annually, according to KTVU. The bill’s funding counterpart, ACA 11, proposes to pay for it with a tax increase on businesses and high-earning individuals.
However, proponents argue that CalCare would cost less than the state’s current system, which equates to $517 billion when considering both taxes and household spending.
We’ve closely tracked Colorado’s pursuit of its own public option insurance plan, which seems now to have reached a compromise that will allow a bill to move forward, according to reporting from Colorado Public Radio. The saga began two years ago when state legislators passed a law requiring Democratic Governor Jared Polis’ administration to develop a public option proposal. Amid the pandemic and broad industry opposition, progress stalled last year on the proposal. Lawmakers picked up the proposal this session, and have made progress on a compromise bill now poised to pass the state’s Democratic legislature.
Unlike the earlier version, the new legislation would not lay the groundwork for a government-run insurance option, but rather would force insurers to offer a plan in which the benefits and premiums are defined and regulated by the state. The bill would also allow the state to regulate how much hospitals and doctors are paid.
In the current version,hospital reimbursement is set at a minimum of 155 percent of Medicare rates, and premiums are expected to be 18 percent lower than the current average. While state Republicans and some progressive Democrats are still opposed, the Colorado Hospital Association and State Association of Health Plans are neutral on the bill, largely eliminating industry opposition.
The role hospitals played in fighting the pandemic surely paved the way toward the compromise bill, which is viewed as much more friendly to providers than the previous proposal.With the Biden administration unlikely to pursue Medicare expansion or a national public option, we expect more Democratic-run states to pursue these sorts of state-level efforts to expand coverage.
In the wake of the pandemic, providers are well-positioned to negotiate—and should use the goodwill they’ve generated to explore more favorable terms, rather than resorting to their usual knee-jerk opposition to these kinds of proposals.






/cdn.vox-cdn.com/uploads/chorus_asset/file/18046968/web_1863137.jpg)


