Two pioneers of mRNA research — the technology that helped the world tame the virus behind the Covid-19 pandemic — won the 2023 Nobel Prize in medicine or physiology on Monday.
Overcoming a lack of broader interest in their work and scientific challenges, Katalin Karikó and Drew Weissman made key discoveries about messenger RNA that enabled scientific teams to start developing the tool into therapies, immunizations, and — as the pandemic spread in 2020 — vaccines targeting the SARS-CoV-2 coronavirus. Moderna and the Pfizer-BioNTech partnership unveiled their mRNA-based Covid-19 shots in record time thanks to the foundational work of Karikó and Weissman, helping save millions of lives.
Karikó, a biochemist, and Weissman, an immunologist, performed their world-changing research on the interaction between mRNA and the immune system at the University of Pennsylvania, where Weissman, 64, remains a professor in vaccine research. Karikó, 68, who later went to work at BioNTech, is now a professor at Szeged University in her native Hungary, and is an adjunct professor at Penn’s Perelman School of Medicine.
The duo will receive 11 million Swedish kronor, or just over $1 million. Their names are added to a list of medicine or physiology Nobel winners that prior to this year included 213 men and 12 women.
The award was announced by Thomas Perlmann, secretary general of Nobel Assembly, in Stockholm. Perlmann said he had spoken to both laureates, describing them as grateful and surprised even though the pair has won numerous awards seen as precursors and had been tipped as likely Nobel recipients at some point.
Every year, the committee considers hundreds of nominations from former Nobel laureates, medical school deans, and prominent scientists from fields including microbiology, immunology, and oncology. Members try to identify a discovery that has altered scientists’ understanding of a subject. And according to the criteria laid out in Alfred Nobel’s will, that paradigm-shifting discovery also has to have benefited humankind.
The Nobel committee framed Karikó and Weissman’s work as a prime example of complementary expertise, with Karikó focused on RNA-based therapies and Weissman bringing a deep knowledge about immune responses to vaccines.
But it was not an easy road for the scientists. Karikó encountered rejection after rejection in the 1990s while applying for grants. She was even demoted while working at Penn, as she toiled away on the lower rungs of academia.
But the scientists persisted, and made a monumental discovery published in 2005 based on simply swapping out some of the components of mRNA.
With instructions from DNA, our cells make strands of mRNA that are then “read” to make proteins. The idea underlying an mRNA vaccine then is to take a piece of mRNA from a pathogen and slip it into our bodies. The mRNA will lead to the production of a protein from the virus, which our bodies learn to recognize and fight should we encounter it again in the form of the actual virus.
It’s an idea that goes back to the 1980s, as scientific advances allowed researchers to make mRNA easily in their labs. But there was a problem: The synthetic mRNA not only produced smaller amounts of protein than the natural version in our cells, it also elicited a potentially dangerous inflammatory immune response, and was often destroyed before it could reach target cells.
Karikó and Weissman’s breakthrough focused on how to overcome that problem. mRNA is made up of four nucleosides, or “letters”: A, U, G, and C. But the version our bodies make includes some nucleosides that are chemically modified — something the synthetic version didn’t, at least until Karikó and Weissman came along. They showed that subbing out some of the building blocks for modified versions allowed their strands of mRNA to sneak past the body’s immune defenses.
While the research did not gain wide attention at the time, it did catch the attention of scientists who would go on to found Moderna and BioNTech. And now, nearly 20 years later, billions of doses of mRNA vaccines have been administered.
For now, the only authorized mRNA products are the Covid-19 shots. But academic researchers and companies are exploring the technology as a potential therapeutic platform for an array of diseases and are using it to develop cancer vaccines as well as immunizations against other infectious diseases, from flu to mpox to HIV. An mRNA vaccine is highly adaptable compared to earlier methods, which makes it easier to alter the underlying recipe of the shot to keep up with viral evolution.
As she gained global fame, Karikó has been open about the barriers she encountered in her scientific career, which raised broader issues about the challenges women and immigrants can face in academia. But she’s said she always believed in the potential of her RNA research.
“I thought of going somewhere else, or doing something else,” Karikó told STAT in 2020, recalling the moment she was demoted. “I also thought maybe I’m not good enough, not smart enough. I tried to imagine: Everything is here, and I just have to do better experiments.”
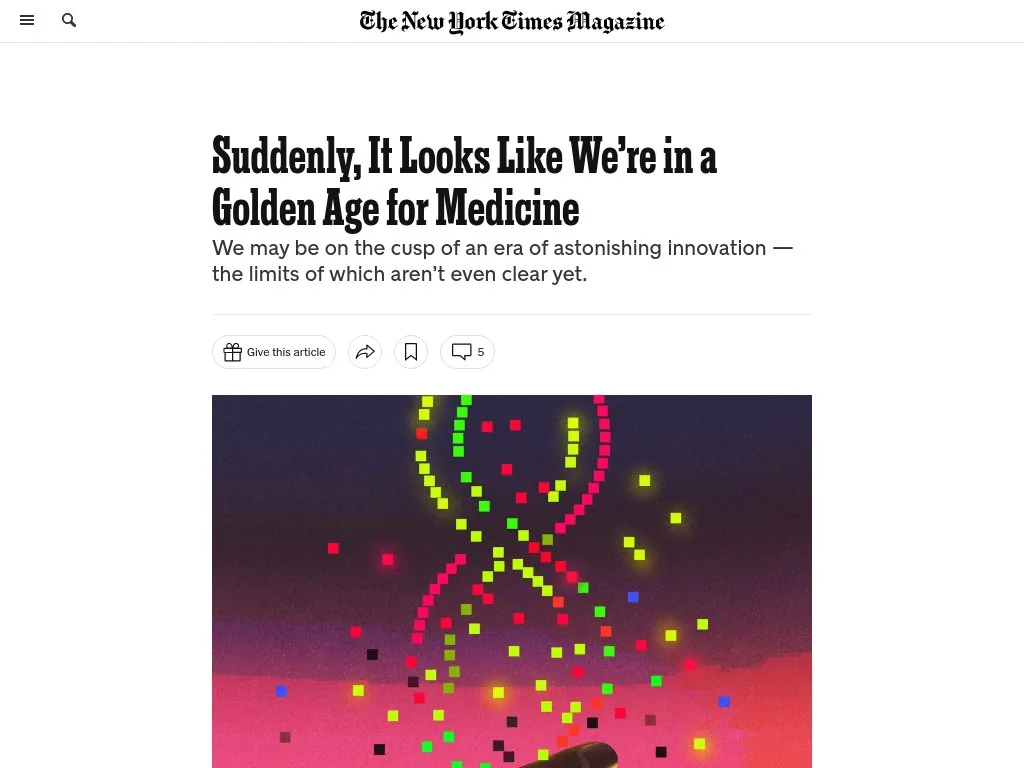
The New York Times Magazine published an encouraging piece about the impressive series of recent medical breakthroughs, many of which have been in the works for decades.
Challenging the conventional wisdom that disruptive scientific breakthroughs have slowed over time, the article points out that the last five years of medicine have featured the rollout of mRNA vaccines, the first instance of a person receiving CRISPR gene therapy, and development of next-generation cancer treatment and weight-loss drugs.
The Gist: The expanding innovation pipeline not only brings excitement and optimism for patients and physicians, but also has the potential to dramatically impact long-established care delivery pathways.
Case in point: used at scale, new weight loss drugs could curb obesity-related chronic diseases and joint replacements—while possibly increasing the incidence of Alzheimer’s disease and cancer as more people live longer lives.
Providers planning for facility and other long-term investments must think through scenarios about how these early, but very promising, innovations could alter demand and shift care delivery needs over coming decades.
A new COVID calamity is hammering China, with a surge in infections prompting a return of lockdowns, including in some manufacturing areas that supply the West.
China reported a record number of infections this week, amid lockdowns and mass testing that are fueling unrest and darkening the country’s economic outlook. Schools in Beijing returned to online teaching.
Why it matters: In addition to the human misery for the world’s most populous country, the effects will be felt around the globe, Axios China author Bethany Allen-Ebrahimian reports from Taipei.
Supply chains are likely to be disrupted, causing prices to rise in an already rocky global economy.
Rare protests broke out today in China’s far western Xinjiang region. Crowds shouted at hazmat-suited guards after a deadly fire triggered anger by prolonged COVID lockdowns, Reuters reports.
“End the lockdown!” shouted protesters in the Xinjiang capital Urumqi, where an apartment fire killed 10.
What’s happening: The moment of truth for China’s zero-COVID policy has finally come.
Either party leaders will need to plunge much of the country into draconian lockdowns, as we saw at the beginning of the pandemic — or they’ll decide it’s time to learn to live with COVID.
Reality check: China’s doctors have warned Xi Jinping that the healthcare system isn’t prepared for the huge outbreak likely to follow the easing of strict anti-COVID measures, the Financial Times reports.
Chinese-made vaccines, which don’t use the mRNA technology employed by many produced by the West, aren’t as effective compared to those made in the U.S. And China has worrisomely low vaccination rates among older people.
But the number of cases in China is actually still very low for anywhere but China.
The big picture: “Zero COVID” restrictions have damaged the economy and undermined people’s trust in government.
That’s a stark about-face from the height of the pandemic. Then, many Chinese people felt the tight central control had protected them better than any other governance model in the world.
But it’s that very model that has plunged China into its current predicament. Xi tied his reputation, and the party’s legitimacy, to the success of “zero COVID.”
Between the lines: Chinese leaders made a huge, politically motivated mistake. They resisted the import of Western-made mRNA vaccines (including Pfizer and Moderna) for its citizens. These vaccines were only recently made available to foreigners.
That’s likely because of Beijing’s big vaccine diplomacy push: Chinese officials touted their own vaccines as the best and safest.
It was politically unpalatable to admit “defeat,” and allow Chinese people to get more effective — but Western-made — jabs.
Exactly 300 years ago, in 1721, Benjamin Franklin and his fellow American colonists faced a deadly smallpox outbreak. Their varying responses constitute an eerily prescient object lesson for today’s world, similarly devastated by a virus and divided over vaccination three centuries later.
As a microbiologist and a Franklin scholar, we see some parallels between then and now that could help governments, journalists and the rest of us cope with the coronavirus pandemic and future threats.
Smallpox strikes Boston
Smallpox was nothing new in 1721. Known to have affected people for at least 3,000 years, it ran rampant in Boston, eventually striking more than half the city’s population. The virus killed about 1 in 13 residents – but the death toll was probably more, since the lack of sophisticated epidemiology made it impossible to identify the cause of all deaths.
What was new, at least to Boston, was a simple procedure that could protect people from the disease. It was known as “variolation” or “inoculation,” and involved deliberately exposing someone to the smallpox “matter” from a victim’s scabs or pus, injecting the material into the skin using a needle. This approach typically caused a mild disease and induced a state of “immunity” against smallpox.
Even today, the exact mechanism is poorly understood and not muchresearch on variolation has been done. Inoculation through the skin seems to activate an immune response that leads to milder symptoms and less transmission, possibly because of the route of infection and the lower dose. Since it relies on activating the immune response with live smallpox variola virus, inoculation is different from the modern vaccination that eradicated smallpox using the much less harmful but related vaccinia virus.
The inoculation treatment, which originated in Asia and Africa, came to be known in Boston thanks to a man named Onesimus. By 1721, Onesimus was enslaved, owned by the most influential man in all of Boston, the Rev. Cotton Mather.
Cotton Mather heard about variolation from an enslaved West African man in his household named Onesimus. Bettman via Getty Images
Known primarily as a Congregational minister, Mather was also a scientist with a special interest in biology. He paid attention when Onesimus told him “he had undergone an operation, which had given him something of the smallpox and would forever preserve him from it; adding that it was often used” in West Africa, where he was from.
Inspired by this information from Onesimus, Mather teamed up with a Boston physician, Zabdiel Boylston, to conduct a scientific study of inoculation’s effectiveness worthy of 21st-century praise. They found that of the approximately 300 people Boylston had inoculated, 2% had died, compared with almost 15% of those who contracted smallpox from nature.
The findings seemed clear: Inoculation could help in the fight against smallpox. Science won out in this clergyman’s mind. But others were not convinced.
Stirring up controversy
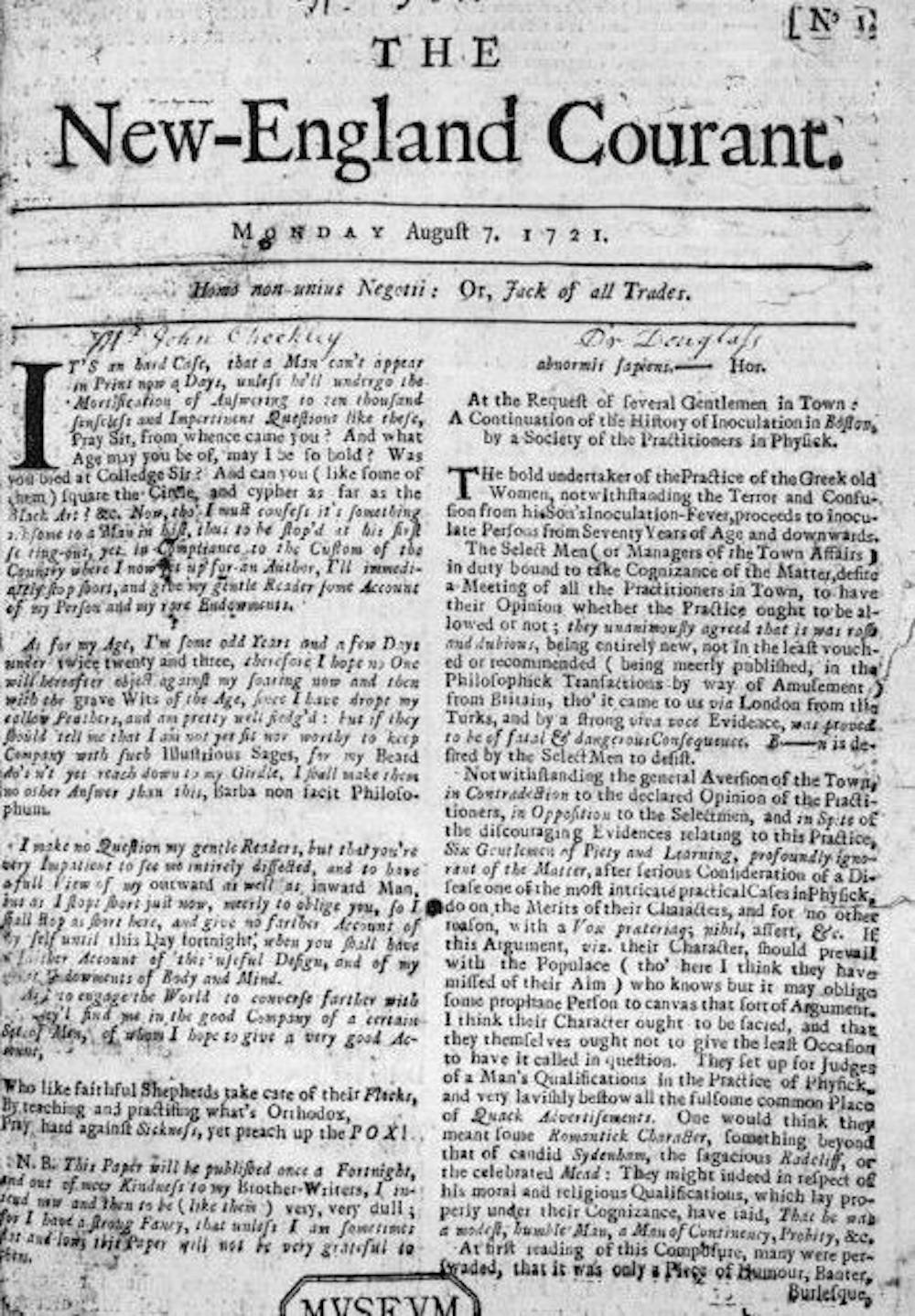
A local newspaper editor named James Franklin had his own affliction – namely an insatiable hunger for controversy. Franklin, who was no fan of Mather, set about attacking inoculation in his newspaper, The New-England Courant.
From its first edition, The New-England Courant covered inoculation. Wikimedia Commons
One article from August 1721 tried to guilt readers into resisting inoculation. If someone gets inoculated and then spreads the disease to someone else, who in turn dies of it, the article asked, “at whose hands shall their Blood be required?” The same article went on to say that “Epidemeal Distempers” such as smallpox come “as Judgments from an angry and displeased God.”
In contrast to Mather and Boylston’s research, the Courant’s articles were designed not to discover, but to sow doubt and distrust. The argument that inoculation might help to spread the disease posits something that was theoretically possible – at least if simple precautions were not taken – but it seems beside the point. If inoculation worked, wouldn’t it be worth this small risk, especially since widespread inoculations would dramatically decrease the likelihood that one person would infect another?
Franklin, the Courant’s editor, had a kid brother apprenticed to him at the time – a teenager by the name of Benjamin.
Historians don’t know which side the younger Franklin took in 1721 – or whether he took a side at all – but his subsequent approach to inoculation years later has lessons for the world’s current encounter with a deadly virus and a divided response to a vaccine.
That he was capable of overcoming this inclination shows Benjamin Franklin’s capacity for independent thought, an asset that would serve him well throughout his life as a writer, scientist and statesman. While sticking with social expectations confers certain advantages in certain settings, being able to shake off these norms when they are dangerous is also valuable. We believe the most successful people are the ones who, like Franklin, have the intellectual flexibility to choose between adherence and independence.
Perhaps the inoculation controversy of 1721 had helped him to understand an unfortunate phenomenon that continues to plague the U.S. in 2021: When people take sides, progress suffers. Tribes, whether long-standing or newly formed around an issue, can devote their energies to demonizing the other side and rallying their own. Instead of attacking the problem, they attack each other.
Franklin, in fact, became convinced that inoculation was a sound approach to preventing smallpox. Years later he intended to have his son Francis inoculated after recovering from a case of diarrhea. But before inoculation took place, the 4-year-old boy contracted smallpox and died in 1736. Citing a rumor that Francis had died because of inoculation and noting that such a rumor might deter parents from exposing their children to this procedure, Franklin made a point of setting the record straight, explaining that the child had “receiv’d the Distemper in the common Way of Infection.”
Writing his autobiography in 1771, Franklin reflected on the tragedy and used it to advocate for inoculation. He explained that he “regretted bitterly and still regret” not inoculating the boy, adding, “This I mention for the sake of parents who omit that operation, on the supposition that they should never forgive themselves if a child died under it; my example showing that the regret may be the same either way, and that, therefore, the safer should be chosen.”
A scientific perspective
A final lesson from 1721 has to do with the importance of a truly scientific perspective, one that embraces science, facts and objectivity.
Smallpox was characterized by fever and aches and pustules all over the body. Before eradication, the virus killed about 30% of those it infected, according to the U.S. Centers for Disease Control and Prevention. Sepia Times/Universal Images Group via Getty Images
Inoculation was a relatively new procedure for Bostonians in 1721, and this lifesaving method was not without deadly risks. To address this paradox, several physicians meticulously collected data and compared the number of those who died because of natural smallpox with deaths after smallpox inoculation. Boylston essentially carried out what today’s researchers would call a clinical study on the efficacy of inoculation. Knowing he needed to demonstrate the usefulness of inoculation in a diverse population, he reported in a short book how he inoculated nearly 300 individuals and carefully noted their symptoms and conditions over days and weeks.
The recent emergency-use authorization of mRNA-based and viral-vector vaccines for COVID-19 has produced a vast array of hoaxes, false claims and conspiracy theories, especially in various social media. Like 18th-century inoculations, these vaccines represent new scientific approaches to vaccination, but ones that are based on decades of scientific research and clinical studies.
We suspect that if he were alive today, Benjamin Franklin would want his example to guide modern scientists, politicians, journalists and everyone else making personal health decisions.Like Mather and Boylston, Franklin was a scientist with a respect for evidence and ultimately for truth.
When it comes to a deadly virus and a divided response to a preventive treatment, Franklin was clear what he would do. It doesn’t take a visionary like Franklin to accept the evidence of medical science today.
In this last episode of our six-part series on vaccinations, supported by the National Institute for Health Care Management Foundation, we cover vaccine development – particularly in the context of the current global pandemic. We discuss the timeline of Covid-19 vaccine development and the mRNA vaccine approach.
Katalin Kariko at her home in Jenkintown, Pa., in February. Dr. Kariko’s early research into mRNA eventually led to development of the Moderna and Pfizer-BioNTech vaccines.Credit.
She grew up in Hungary, daughter of a butcher. She decided she wanted to be a scientist, although she had never met one. She moved to the United States in her 20s, but for decades never found a permanent position, instead clinging to the fringes of academia.
Now Katalin Kariko, 66, known to colleagues as Kati, has emerged as one of the heroes of Covid-19 vaccine development. Her work, with her close collaborator, Dr. Drew Weissman of the University of Pennsylvania, laid the foundation for the stunningly successful vaccines made by Pfizer-BioNTech and Moderna.
For her entire career, Dr. Kariko has focused on messenger RNA, or mRNA — the genetic script that carries DNA instructions to each cell’s protein-making machinery. She was convinced mRNA could be used to instruct cells to make their own medicines, including vaccines.
But for many years her career at the University of Pennsylvania was fragile. She migrated from lab to lab, relying on one senior scientist after another to take her in. She never made more than $60,000 a year.
By all accounts intense and single-minded, Dr. Kariko lives for “the bench” — the spot in the lab where she works. She cares little for fame. “The bench is there, the science is good,” she shrugged in a recent interview. “Who cares?”
Dr. Anthony Fauci, director of the National Institutes of Allergy and infectious Diseases, knows Dr. Kariko’s work. “She was, in a positive sense, kind of obsessed with the concept of messenger RNA,” he said.
Dr. Kariko’s struggles to stay afloat in academia have a familiar ring to scientists. She needed grants to pursue ideas that seemed wild and fanciful. She did not get them, even as more mundane research was rewarded.
“When your idea is against the conventional wisdom that makes sense to the star chamber, it is very hard to break out,” said Dr. David Langer, a neurosurgeon who has worked with Dr. Kariko.
Dr. Kariko’s ideas about mRNA were definitely unorthodox. Increasingly, they also seem to have been prescient.
“It’s going to be transforming,” Dr. Fauci said of mRNA research. “It is already transforming for Covid-19, but also for other vaccines. H.I.V. — people in the field are already excited. Influenza, malaria.”
‘I Felt Like a God’
For Dr. Kariko, most every day was a day in the lab. “You are not going to work — you are going to have fun,” her husband, Bela Francia, manager of an apartment complex, used to tell her as she dashed back to the office on evenings and weekends. He once calculated that her endless workdays meant she was earning about a dollar an hour.
For many scientists, a new discovery is followed by a plan to make money, to form a company and get a patent. But not for Dr. Kariko. “That’s the furthest thing from Kate’s mind,” Dr. Langer said.
She grew up in the small Hungarian town of Kisujszallas. She earned a Ph.D. at the University of Szeged and worked as a postdoctoral fellow at its Biological Research Center.
In 1985, when the university’s research program ran out of money, Dr. Kariko, her husband, and 2-year-old daughter, Susan, moved to Philadelphia for a job as a postdoctoral student at Temple University. Because the Hungarian government only allowed them to take $100 out of the country, she and her husband sewed £900 (roughly $1,246 today) into Susan’s teddy bear. (Susan grew up to be a two-time Olympic gold medal winner in rowing.)
When Dr. Kariko started, it was early days in the mRNA field. Even the most basic tasks were difficult, if not impossible. How do you make RNA molecules in a lab? How do you get mRNA into cells of the body?
In 1989, she landed a job with Dr. Elliot Barnathan, then a cardiologist at the University of Pennsylvania. It was a low-level position, research assistant professor, and never meant to lead to a permanent tenured position. She was supposed to be supported by grant money, but none came in.
She and Dr. Barnathan planned to insert mRNA into cells, inducing them to make new proteins. In one of the first experiments, they hoped to use the strategy to instruct cells to make a protein called the urokinase receptor. If the experiment worked, they would detect the new protein with a radioactive molecule that would be drawn to the receptor.
“Most people laughed at us,” Dr. Barnathan said.
One fateful day, the two scientists hovered over a dot-matrix printer in a narrow room at the end of a long hall. A gamma counter, needed to track the radioactive molecule, was attached to a printer. It began to spew data.
Their detector had found new proteins produced by cells that were never supposed to make them — suggesting that mRNA could be used to direct any cell to make any protein, at will.
“I felt like a god,” Dr. Kariko recalled.
She and Dr. Barnathan were on fire with ideas. Maybe they could use mRNA to improve blood vessels for heart bypass surgery. Perhaps they could even use the procedure to extend the life span of human cells.
Dr. Barnathan, though, soon left the university, accepting a position at a biotech firm, and Dr. Kariko was left without a lab or financial support. She could stay at Penn only if she found another lab to take her on. “They expected I would quit,” she said.
Universities only support low-level Ph.D.s for a limited amount of time, Dr. Langer said: “If they don’t get a grant, they will let them go.” Dr. Kariko “was not a great grant writer,” and at that point “mRNA was more of an idea,” he said.
But Dr. Langer knew Dr. Kariko from his days as a medical resident, when he had worked in Dr. Barnathan’s lab. Dr. Langer urged the head of the neurosurgery department to give Dr. Kariko’s research a chance. “He saved me,” she said.
Dr. Langer thinks it was Dr. Kariko who saved him — from the kind of thinking that dooms so many scientists.
Working with her, he realized that one key to real scientific understanding is to design experiments that always tell you something, even if it is something you don’t want to hear. The crucial data often come from the control, he learned — the part of the experiment that involves a dummy substance for comparison.
“There’s a tendency when scientists are looking at data to try to validate their own idea,” Dr. Langer said. “The best scientists try to prove themselves wrong. Kate’s genius was a willingness to accept failure and keep trying, and her ability to answer questions people were not smart enough to ask.”
Dr. Langer hoped to use mRNA to treat patients who developed blood clots following brain surgery, often resulting in strokes. His idea was to get cells in blood vessels to make nitric oxide, a substance that dilates blood vessels, but has a half-life of milliseconds. Doctors can’t just inject patients with it.
He and Dr. Kariko tried their mRNA on isolated blood vessels used to study strokes. It failed. They trudged through snow in Buffalo, N.Y., to try it in a laboratory with rabbits prone to strokes. Failure again.
And then Dr. Langer left the university, and the department chairman said he was leaving as well. Dr. Kariko again was without a lab and without funds for research.
A meeting at a photocopying machine changed that. Dr. Weissman happened by, and she struck up a conversation. “I said, ‘I am an RNA scientist — I can make anything with mRNA,’” Dr. Kariko recalled.
Dr. Weissman told her he wanted to make a vaccine against H.I.V. “I said, ‘Yeah, yeah, I can do it,’” Dr. Kariko said.
Despite her bravado, her research on mRNA had stalled. She could make mRNA molecules that instructed cells in petri dishes to make the protein of her choice. But the mRNA did not work in living mice.
“Nobody knew why,” Dr. Weissman said. “All we knew was that the mice got sick. Their fur got ruffled, they hunched up, they stopped eating, they stopped running.”
It turned out that the immune system recognizes invading microbes by detecting their mRNA and responding with inflammation. The scientists’ mRNA injections looked to the immune system like an invasion of pathogens.
But with that answer came another puzzle. Every cell in every person’s body makes mRNA, and the immune system turns a blind eye. “Why is the mRNA I made different?” Dr. Kariko wondered.
A control in an experiment finally provided a clue. Dr. Kariko and Dr. Weissman noticed their mRNA caused an immune overreaction. But the control molecules, another form of RNA in the human body — so-called transfer RNA, or tRNA — did not.
A molecule called pseudouridine in tRNA allowed it to evade the immune response. As it turned out, naturally occurring human mRNA also contains the molecule.
Added to the mRNA made by Dr. Kariko and Dr. Weissman, the molecule did the same — and also made the mRNA much more powerful, directing the synthesis of 10 times as much protein in each cell.
The idea that adding pseudouridine to mRNA protected it from the body’s immune system was a basic scientific discovery with a wide range of thrilling applications. It meant that mRNA could be used to alter the functions of cells without prompting an immune system attack.
“We both started writing grants,” Dr. Weissman said. “We didn’t get most of them. People were not interested in mRNA. The people who reviewed the grants said mRNA will not be a good therapeutic, so don’t bother.’”
Leading scientific journals rejected their work. When the research finally was published, in Immunity, it got little attention.
Dr. Weissman and Dr. Kariko then showed they could induce an animal — a monkey — to make a protein they had selected. In this case, they injected monkeys with mRNA for erythropoietin, a protein that stimulates the body to make red blood cells. The animals’ red blood cell counts soared.
The scientists thought the same method could be used to prompt the body to make any protein drug, like insulin or other hormones or some of the new diabetes drugs. Crucially, mRNA also could be used to make vaccines unlike any seen before.
Instead of injecting a piece of a virus into the body, doctors could inject mRNA that would instruct cells to briefly make that part of the virus.
“We talked to pharmaceutical companies and venture capitalists. No one cared,” Dr. Weissman said. “We were screaming a lot, but no one would listen.”
Eventually, though, two biotech companies took notice of the work: Moderna, in the United States, and BioNTech, in Germany. Pfizer partnered with BioNTech, and the two now help fund Dr. Weissman’s lab.
‘Oh, It Works’
Soon clinical trials of an mRNA flu vaccine were underway, and there were efforts to build new vaccines against cytomegalovirus and the Zika virus, among others. Then came the coronavirus.
Researchers had known for 20 years that the crucial feature of any coronavirus is the spike protein sitting on its surface, which allows the virus to inject itself into human cells. It was a fat target for an mRNA vaccine.
Chinese scientists posted the genetic sequence of the virus ravaging Wuhan in January 2020, and researchers everywhere went to work. BioNTech designed its mRNA vaccine in hours; Moderna designed its in two days.
The idea for both vaccines was to introduce mRNA into the body that would briefly instruct human cells to produce the coronavirus’s spike protein. The immune system would see the protein, recognize it as alien, and learn to attack the coronavirus if it ever appeared in the body.
The vaccines, though, needed a lipid bubble to encase the mRNA and carry it to the cells that it would enter. The vehicle came quickly, based on 25 years of work by multiple scientists, including Pieter Cullis of the University of British Columbia.
Scientists also needed to isolate the virus’s spike protein from the bounty of genetic data provided by Chinese researchers. Dr. Barney Graham, of the National Institutes of Health, and Jason McClellan, of the University of Texas at Austin, solved that problem in short order.
Testing the quickly designed vaccines required a monumental effort by companies and the National Institutes of Health. But Dr. Kariko had no doubts.
On Nov. 8, the first results of the Pfizer-BioNTech study came in, showing that the mRNA vaccine offered powerful immunity to the new virus. Dr. Kariko turned to her husband. “Oh, it works,” she said. “I thought so.”
To celebrate, she ate an entire box of Goobers chocolate-covered peanuts. By herself.
Dr. Weissman celebrated with his family, ordering takeout dinner from an Italian restaurant, “with wine,” he said. Deep down, he was awed.
“My dream was always that we develop something in the lab that helps people,” Dr. Weissman said. “I’ve satisfied my life’s dream.”
Dr. Kariko and Dr. Weissman were vaccinated on Dec. 18 at the University of Pennsylvania. Their inoculations turned into a press event, and as the cameras flashed, she began to feel uncharacteristically overwhelmed.
A senior administrator told the doctors and nurses rolling up their sleeves for shots that the scientists whose research made the vaccine possible were present, and they all clapped. Dr. Kariko wept.
Things could have gone so differently, for the scientists and for the world, Dr. Langer said. “There are probably many people like her who failed,” he said.
A new report out later today concludes that basic scientific research plays an essential role in creating companies that later produce thousands of jobs and billions in economic value.
Why it matters: The report uses thepandemic — and especially the rapid development of new mRNA vaccines — to show how basic research funding from the government lays the necessary groundwork for economically valuable companies down the road.
By the numbers: The Science Coalition — a nonprofit group that represents 50 of the nation’s top private and public research universities — identified 53 companies that have spun off from federally funded university research.
Those companies — which range from pharmaceutical startups to agriculture firms — have contributed more than $1.3 billion to U.S. GDP between 2015 and 2019, while supporting the creation of more than 100,000 jobs.
What they’re saying:“The COVID-19 pandemic has shown that the need for the federal government to continue investing in fundamental research is far from theoretical,” says John Latini, president of the Science Coalition. “Consistent, sustained, robust federal funding is how science evolves.”
Details: Latini praised the Biden administration’s first budget proposal to Congress, released last week, which includes what would be a $9 billion funding boost for the National Institutes of Health (NIH) — the country’s single biggest science research funding agency.
The National Oceanic and Atmospheric Administration would see its budget rise to a record high of $6.9 billion, including $800 millionreserved for climate research.
The catch: The Biden budget proposal is just that, and it will ultimately be up to Congress to decide how much to allocate to research agencies.
Context: Government research funding is vital because private money tends to go to applied research. But without basic research — the lifeblood of science — the U.S. risks missing out on potentially world-changing innovations in the future.
The long-term value of that funding can be seen in the story of Katalin Kariko, an obscure biomedical researcher who labored for years on mRNA with little reward — until the pandemic, when her work helped provide the foundation for mRNA COVID-19 vaccines.
The bottom line: Because its ultimate payoff might lay years in the future, it’s easy to see basic research funding as a waste — until the day comes when we need it.









{kind=link}