

Cartoon – It will go away Magically



President-elect Joe Biden’s front-runner for secretary of Health and Human Services is New Mexico Governor Michelle Lujan Grisham, and he may announce several of his administration’s health leaders as soon as next week, according to people familiar with the matter.
The position of HHS secretary is down to two possibilities, the people said, between Lujan Grisham and former Surgeon General Vivek Murthy, a co-chair of the coronavirus advisory board Biden appointed shortly after he was elected.
Biden’s health team will assume office with the U.S. still suffering from the pandemic, as virus cases and hospitalizations soared over the past month. His health secretary is expected to have input on filling other top health posts, such as FDA commissioner and the administrator of the Centers for Medicare and Medicaid Services, the people said, so those appointments may not be announced until later.
The Health and Human Services secretary will have the tough task of rebuilding Obamacare, which Biden has promised to expand. That will be a difficult undertaking with a Republican-led Senate.
Murthy or Jeff Zients, who led the Obama administration effort to repair healthcare.gov, the faulty Obamacare website, may be named to a leadership role on the pandemic, according to the people familiar with the matter — a “Covid-19 czar.”
Mandy Cohen, the North Carolina state health secretary, is a favorite for CMS, the people said. Biden’s choices to lead the Food and Drug Administration appear narrowed down to David Kessler, a former commissioner of the agency who is another co-chair of his coronavirus advisory board, and Joshua Sharfstein, a former FDA official who is a vice dean at Johns Hopkins University’s Bloomberg School of Public Health.
Biden announced his economic team on Tuesday, a group led by Treasury Secretary-designate Janet Yellen whose top priority will be restoring jobs eliminated by the pandemic. An announcement on some of his health team could come as soon as Monday, the people said.
The people familiar with the matter asked not to be identified because talks are still ongoing and no final decision has been made. It’s not clear how many people will be announced at once, or which positions would later be filled by the health secretary once the Biden administration is in place.

Biden’s transition team did not immediately respond to a request for comment.
The U.S. recorded 158,000 new coronavirus infections on Monday and a record 205,000 cases three days earlier. Biden will take office as distribution of coronavirus vaccines ramps up, and he has warned that any delay in the transition to his administration could slow or complicate that endeavor.
Lujan Grisham is seen as having an easier path to confirmation than Murthy, who has spoken out against gun violence as a public health threat and may draw strong opposition from Senate Republicans as a result, the people familiar with the matter said.

If he isn’t nominated to lead HHS, Murthy is under consideration as Covid-19 czar or another role, including a second stint as surgeon general, the people said. Murthy talks to Biden almost every day as co-chair of his advisory board and is seen as having influential supporters.
Murthy and Zients have also represented Biden’s transition team on calls with current HHS officials, two of the people said.
Biden’s team is still discussing what the White House coronavirus task force and Operation Warp Speed — the Trump administration’s effort to fast-track vaccines — will look like under the new administration.
If Biden announces his health team next week, he may be just days ahead of the first emergency FDA approval of a coronavirus vaccine. President Donald Trump is planning a vaccine summit next week at the White House, while an FDA advisory panel is scheduled to meet on Dec. 10 to discuss the shots.
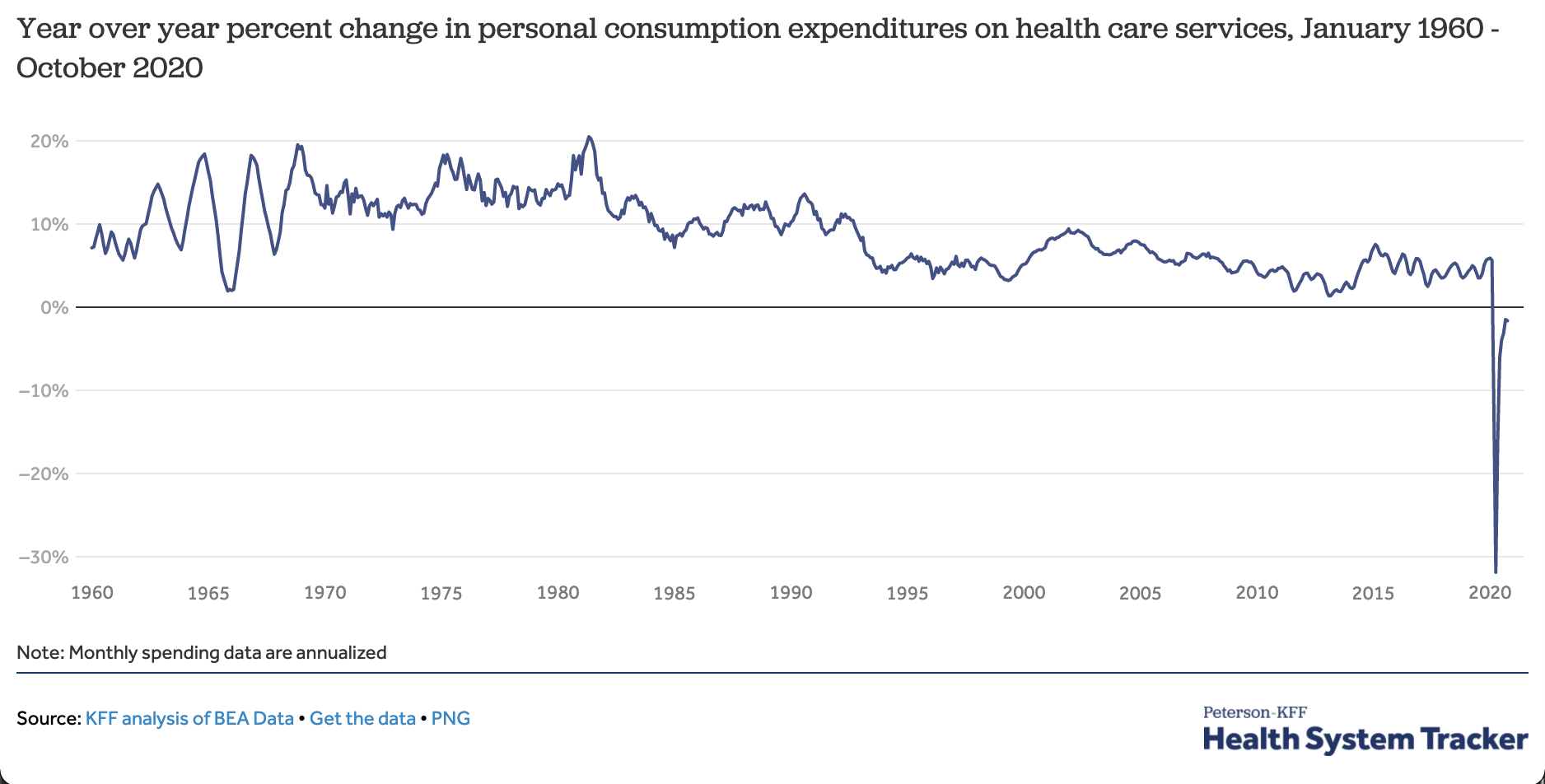
The coronavirus pandemic has caused national health care spending to go down this year — the first time that’s ever happened.
The big picture: Any big recession depresses the use of health services because people have less money to spend. But this pandemic has also directly attacked the health system, causing people to defer or skip care for fear of becoming infected.
By the numbers: Year-to-date spending on health services is down about 2% from last year. Health spending for the calendar year may end up lower than it was in 2019.
Context: This is the first time expenditures for patient care have fallen year-over-year since data became available in the 1960s.
What’s next: Spending and utilization have been recovering, but could fall again if the current spike in cases prompts either hospitals or patients to again hold off on elective care.

Many of the state’s hospitals have maintained lower numbers of beds in part to limit the length of patient stays and lower costs. But that approach is now being tested.
For all its size and economic might, California has long had few hospital beds relative to its population, a shortfall that state officials now say may prove catastrophic.
California is experiencing its largest surge in coronavirus cases with an average of nearly 15,000 new cases a day, an increase of 50 percent from the previous record over the summer.
So even though the state has some of the country’s most restrictive measures to prevent the spread of the virus, an influx of people with severe cases of Covid-19 may force overwhelmed hospitals to turn patients away by Christmas, Gov. Gavin Newsom warned this week.
A dearth of hospital beds has been a worldwide problem throughout the pandemic, but California, with a population of 40 million, has a particularly acute shortage. The wealthiest state in the wealthiest country has 1.8 hospital beds per 1,000 people, a level that exceeds only two states, Washington and Oregon, according to 2018 data compiled by the Kaiser Family Foundation. California has one-third the number of beds per capita as Poland.
Many hospitals in California have maintained lower numbers of beds in part to limit the length of patient stays and lower costs. But that approach is now being tested.
In addition to beds, a shortage of nursing staff will make handling the surge of virus cases “extraordinarily difficult for us in California,” said Carmela Coyle, the head of the California Hospital Association, which represents 400 hospitals across the state.
“This pandemic is a story of shortage, whether it is shortages of personal protective equipment, shortages of testing supplies, shortages of the trained staff needed to deal with these patients,” Ms. Coyle said. “It’s what has made this pandemic unique and different from other disasters.”

Also unlike other catastrophes, California will not be able to rely on other states for assistance. Mutual aid has been a cornerstone in its planning for disasters, requesting, for example, thousands of firefighters from neighboring states to help in dousing the mega-fires of recent years.
But with so many parts of the country struggling with the coronavirus at the same time, there are few traveling nurses available or nearby hospital beds to spare.
“You have to think of this as a natural disaster, like an earthquake — there’s a lot of need for hospitalization,” said Dr. George Rutherford, a professor of epidemiology at the University of California, San Francisco. “But the difference here is that it’s happening across the country. We can’t send people to Reno, Phoenix or Tucson. We’re stuck.”
The state government says it has 11 surge facilities, or alternative setups, including mothballed medical buildings and at least one sports arena, ready if hospitals become overloaded.
Beyond California, hospitals have been scrambling in recent weeks to handle a new rush of patients, particularly in parts of the Sun Belt and New England that had largely avoided coronavirus spikes in the spring and summer. The country is likely to hit a record 100,000 hospitalizations this week.CALIFORNIA TODAY: The news and stories that matter to Californians (and anyone else interested in the state).Sign Up
As hospitals exceed or get close to exceeding their capacity for coronavirus patients, state and local officials have been opening hospitals in parking lots or unoccupied buildings.
In Rhode Island, where infections have rapidly increased in recent weeks, a field hospital opened on Monday in the state’s second-largest city, Cranston. At a cost of $8 million, a former call center for Citizens Bank was converted into a 335-bed field hospital. In New Mexico, a vacant medical center in Albuquerque was being used for recovering coronavirus patients. “We are seeing the worst rates that we’ve seen since the pandemic hit,” Mayor Tim Keller said in a recent interview.

Nancy Foster, the American Hospital Association’s vice president for quality and patient safety policy, said hospital systems that are busy during the pandemic have not yet fully examined how they could have been better prepared. But she said the lack of hospital beds in many states reflected pre-Covid times.
“In an era when you’re focused on reducing the cost of health care, having excess capacity — that you’re heating and lighting and cleaning and all of that stuff — is just antithetical to your efforts to be as lean as possible, to be as cost-efficient as possible,” Ms. Foster said. “So we’re going to have some critical thinking around what’s that right balance between keeping costs low and being prepared in case a disaster happens.”
The number of hospital beds in California has declined over time partly because of a trend toward more outpatient care, said Kristof Stremikis, an expert on the state’s hospital system at the California Health Care Foundation. But more acute than the shortage of beds, Mr. Stremikis says, are staffing shortages, especially in regions with high concentrations of Black, Latino and Native American patients.
“The system is blinking red when it comes to the work force,” Mr. Stremikis said. “It’s nurses, doctors, allied health professionals — we don’t have enough of many different types of clinicians in California and they’re not in the right places. It’s a huge issue.”
Mr. Newsom has said California would draw from a registry of retired or nonpracticing health care workers and deploy them to hospitals.
But Ms. Coyle, the head of the California Hospital Association, says she does not think volunteers can bridge the gap.
“We are down to a very, very small fraction who are willing to serve,” she said. “Those volunteers were not trained at a level to be as helpful in a hospital setting.”

At the county level, health officers are counting down the days until their hospitals are full. On Sunday, California became the first state to record more than 100,000 cases in a week, according to a New York Times database. The state government estimates that about 12 percent of cases end up in a hospital.
Dr. Sara Cody, the chief health officer for Santa Clara County, which includes a large slice of Silicon Valley, projects that hospitals in the county will reach capacity by mid-December.
“This is the most difficult phase of the pandemic so far,” Dr. Cody said. “Everyone is tired.”
She is expecting a spike in cases from Thanksgiving gatherings, which could accelerate the timeline, she said.
Few states have been as aggressive in combating the pandemic as California, which now has a stockpile of a half-billion face masks. Los Angeles last week announced a ban on gatherings with other households. In Santa Clara County, hotels are now only reserved for essential travel and a ban on contact sports is forcing the San Francisco 49ers to play home games in Arizona.
“We have done everything that we can do as local leaders and health officials,” said Dr. Cody, who led the effort in March to put in place the country’s first shelter-in-place order. “We have worked as hard as we can work. We have tried everything that we know how to do. But without bold action at the state or federal level we are not going to be able to slow this down. We are not an island.”
Across California a weary populace wondered about the effectiveness of the state’s measures.
In Los Angeles, local officials were under fire after hundreds of tests scheduled for Tuesday at Union Station were canceled because of a film shoot, a remake of the 1990s romantic comedy “She’s All That.” People who had scheduled tests were informed of the cancellation on Monday afternoon, and it was not until after midnight that Mayor Eric Garcetti announced the tests were back on.
The filming was still taking place on Tuesday morning as Wendy Ambriz swabbed her mouth at the station’s testing kiosk.
Ms. Ambriz did not think the county’s restriction of outdoor dining, which went into effect last week, was necessary, noting that kitchen staffs are fastidious about cleanliness. But she did not blame government officials for the coronavirus spiraling out of control in Southern California.
“People don’t really follow directions,” she said.
That assessment appears to hold true for some of the state’s officials.
Sheila Kuehl, who sits on the county board of supervisors, was spotted at an Italian restaurant in Santa Monica hours after publicly calling outdoor dining “a most dangerous situation” and voting to ban it. In a statement on Monday, Ms. Kuehl’s office noted that the ban had not yet gone into effect when the dinner occurred. Her meal recalled another moment of apparent hypocrisy, a meal attended by Mr. Newsom and a gaggle of lobbyists at the luxurious French Laundry restaurant in Napa Valley just as the governor was advising residents to avoid meeting with large groups.
Outside the Broad Street Oyster Company in Malibu last week, picnic tables were cordoned off and the restaurant was not seating customers. But that did not stop people from eating there — they just ducked under the tape.
https://www.yahoo.com/news/covid-19-silently-spreading-across-193716206.html

The first confirmed coronavirus case in the U.S. was reported on Jan. 19 in a Washington man after returning from Wuhan, China, where the first outbreak of COVID-19 occurred.
Now, data from a new government study paints a different picture — the coronavirus may have been silently spreading in America as early as December 2019.
Researchers with the Centers for Disease Control and Prevention collected 7,389 blood samples from routine donations to the American Red Cross between Dec. 13, 2019 and Jan. 17, 2020.
Of the samples, 106 contained coronavirus antibodies, suggesting those individuals’ immune systems battled COVID-19 at some point.
A total of 39 donations carrying coronavirus antibodies came from residents in the western states of California, Oregon and Washington and 67 samples from the more eastern states of Connecticut, Iowa, Massachusetts, Michigan, Rhode Island and Wisconsin.
The study, published Monday in the journal Clinical Infectious Diseases, adds to growing evidence that the coronavirus had been spreading right under our noses long before testing could confirm it.
“The presence of these serum antibodies indicate that isolated SARS-CoV-2 infections may have occurred in the western portion of the United States earlier than previously recognized or that a small portion of the population may have pre-existing antibodies that bind SARS-CoV-2,” the study reads.
However, the researchers say “widespread community transmission was not likely until late February.”
Some of these early infections may have gone unnoticed because patients with mild or asymptomatic cases may not have sought medical care at the time, the researchers explain in the study. Sick patients with symptoms who did visit a doctor may not have had a respiratory sample collected, so appropriate testing may not have been conducted.
But the researchers wonder if the detection of antibodies in these patient samples really does indicate a past coronavirus infection, and not of another pathogen in the coronavirus family, such as the common cold.
A study published in August found that people who have had the common cold could have cells in their immune systems that might be able to recognize those of the novel coronavirus, McClatchy News reported.
Scientists behind the finding say this “memory” of viruses past could explain why some people are only slightly affected by COVID-19, while others get severely sick.
The researchers call this phenomenon “cross reactivity,” but they note it’s just one of several limitations to their study. The team also said they can’t tell if the COVID-19 cases were community- or travel-associated and that none of the antibody results can be considered “true positives.”
“A true positive would only be collected from an individual with a positive molecular diagnostic test,” the researchers wrote in the study.
Back in May, doctors in Paris also learned the coronavirus had been silently creeping around Europe a month before the official first-known cases were diagnosed in the region.
The first two cases — with known travel to China — in France were reported Jan. 24, but after testing frozen samples from earlier patient records, doctors realized a man with no recent travel had the coronavirus in December.





