The average number of new daily COVID-19 cases has increased 94 percent over the past two weeks, according to data from The New York Times, as worries over outbreaks climb nationwide.
The U.S. recorded a seven-day average of more than 23,000 daily cases on Monday, almost doubling from the average two weeks ago, as less than half of the total population is fully vaccinated.
Monday’s count of 32,105 newly confirmed cases pushed the seven-day average up from its Sunday level of more than 19,000 new cases — a 60 percent increase from two weeks prior.
All but four states — West Virginia, Maine, South Dakota and Iowa — have seen increased daily averages in the past 14 days, and the average in 16 states at least doubled in that period.
This comes as the highly transmissible delta variant was declared the dominant strain in the U.S. last week.
At the same time, vaccinations have stalled, with the daily rate reaching its lowest point during President Biden’s tenure on Sunday at slightly more than 506,000. Monday saw a small uptick in the average rate to more than 527,000 per day, according to Our World in Data.
The rise in case counts comes as the Centers for Disease Control and Prevention says just 48 percent of the total population is fully vaccinated. Officials have said fully vaccinated people are protected from the virus, while unvaccinated people are at much higher risk for serious illness and death.
This leaves a majority of Americans still vulnerable to the virus, particularly children under 12 years old, who are not authorized to get the vaccine. More than 56 percent of the eligible population aged 12 and older is fully vaccinated.
The Biden administration has strived to boost vaccination numbers over the past few months and signaled a new strategy focused on grassroots campaigning to promote the vaccine last week. The country fell short of the president’s goal to get 70 percent of adults at least one dose by the Fourth of July.
Increases in COVID-19 cases have previously signaled during the pandemic an upcoming rise in hospitalizations and deaths. The Times data shows that average deaths are still decreasing, but average daily hospitalizations are climbing, with a 16 percent increase from two weeks ago.
Still, case counts are much lower than the devastating peak that hit the U.S. in January, and experts say the country will not reach that level of infection again, as vulnerable populations have gotten vaccinated. Seventy-nine percent of those aged 65 and older are considered fully vaccinated.
Exactly 300 years ago, in 1721, Benjamin Franklin and his fellow American colonists faced a deadly smallpox outbreak. Their varying responses constitute an eerily prescient object lesson for today’s world, similarly devastated by a virus and divided over vaccination three centuries later.
As a microbiologist and a Franklin scholar, we see some parallels between then and now that could help governments, journalists and the rest of us cope with the coronavirus pandemic and future threats.
Smallpox strikes Boston
Smallpox was nothing new in 1721. Known to have affected people for at least 3,000 years, it ran rampant in Boston, eventually striking more than half the city’s population. The virus killed about 1 in 13 residents – but the death toll was probably more, since the lack of sophisticated epidemiology made it impossible to identify the cause of all deaths.
What was new, at least to Boston, was a simple procedure that could protect people from the disease. It was known as “variolation” or “inoculation,” and involved deliberately exposing someone to the smallpox “matter” from a victim’s scabs or pus, injecting the material into the skin using a needle. This approach typically caused a mild disease and induced a state of “immunity” against smallpox.
Even today, the exact mechanism is poorly understood and not muchresearch on variolation has been done. Inoculation through the skin seems to activate an immune response that leads to milder symptoms and less transmission, possibly because of the route of infection and the lower dose. Since it relies on activating the immune response with live smallpox variola virus, inoculation is different from the modern vaccination that eradicated smallpox using the much less harmful but related vaccinia virus.
The inoculation treatment, which originated in Asia and Africa, came to be known in Boston thanks to a man named Onesimus. By 1721, Onesimus was enslaved, owned by the most influential man in all of Boston, the Rev. Cotton Mather.
Cotton Mather heard about variolation from an enslaved West African man in his household named Onesimus. Bettman via Getty Images
Known primarily as a Congregational minister, Mather was also a scientist with a special interest in biology. He paid attention when Onesimus told him “he had undergone an operation, which had given him something of the smallpox and would forever preserve him from it; adding that it was often used” in West Africa, where he was from.
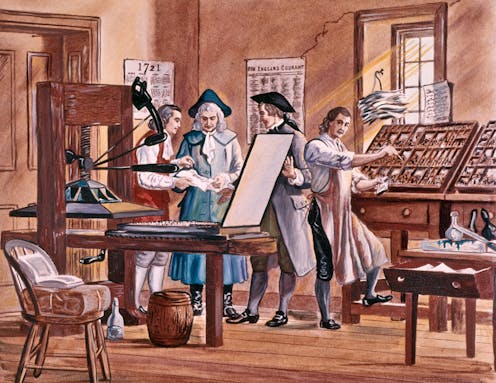
Inspired by this information from Onesimus, Mather teamed up with a Boston physician, Zabdiel Boylston, to conduct a scientific study of inoculation’s effectiveness worthy of 21st-century praise. They found that of the approximately 300 people Boylston had inoculated, 2% had died, compared with almost 15% of those who contracted smallpox from nature.
The findings seemed clear: Inoculation could help in the fight against smallpox. Science won out in this clergyman’s mind. But others were not convinced.
Stirring up controversy
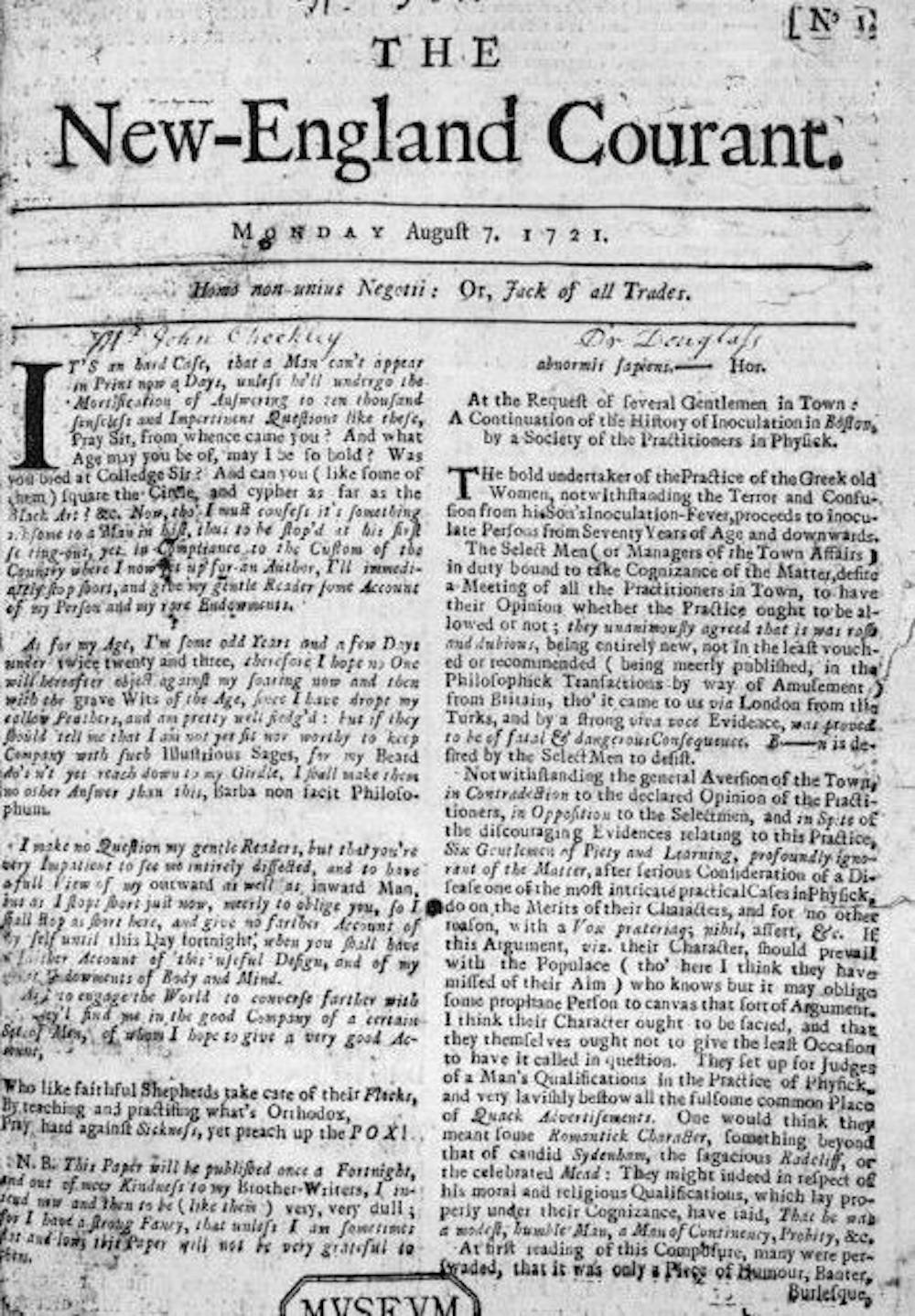
A local newspaper editor named James Franklin had his own affliction – namely an insatiable hunger for controversy. Franklin, who was no fan of Mather, set about attacking inoculation in his newspaper, The New-England Courant.
From its first edition, The New-England Courant covered inoculation. Wikimedia Commons
One article from August 1721 tried to guilt readers into resisting inoculation. If someone gets inoculated and then spreads the disease to someone else, who in turn dies of it, the article asked, “at whose hands shall their Blood be required?” The same article went on to say that “Epidemeal Distempers” such as smallpox come “as Judgments from an angry and displeased God.”
In contrast to Mather and Boylston’s research, the Courant’s articles were designed not to discover, but to sow doubt and distrust. The argument that inoculation might help to spread the disease posits something that was theoretically possible – at least if simple precautions were not taken – but it seems beside the point. If inoculation worked, wouldn’t it be worth this small risk, especially since widespread inoculations would dramatically decrease the likelihood that one person would infect another?
Franklin, the Courant’s editor, had a kid brother apprenticed to him at the time – a teenager by the name of Benjamin.
Historians don’t know which side the younger Franklin took in 1721 – or whether he took a side at all – but his subsequent approach to inoculation years later has lessons for the world’s current encounter with a deadly virus and a divided response to a vaccine.
That he was capable of overcoming this inclination shows Benjamin Franklin’s capacity for independent thought, an asset that would serve him well throughout his life as a writer, scientist and statesman. While sticking with social expectations confers certain advantages in certain settings, being able to shake off these norms when they are dangerous is also valuable. We believe the most successful people are the ones who, like Franklin, have the intellectual flexibility to choose between adherence and independence.
Perhaps the inoculation controversy of 1721 had helped him to understand an unfortunate phenomenon that continues to plague the U.S. in 2021: When people take sides, progress suffers. Tribes, whether long-standing or newly formed around an issue, can devote their energies to demonizing the other side and rallying their own. Instead of attacking the problem, they attack each other.
Franklin, in fact, became convinced that inoculation was a sound approach to preventing smallpox. Years later he intended to have his son Francis inoculated after recovering from a case of diarrhea. But before inoculation took place, the 4-year-old boy contracted smallpox and died in 1736. Citing a rumor that Francis had died because of inoculation and noting that such a rumor might deter parents from exposing their children to this procedure, Franklin made a point of setting the record straight, explaining that the child had “receiv’d the Distemper in the common Way of Infection.”
Writing his autobiography in 1771, Franklin reflected on the tragedy and used it to advocate for inoculation. He explained that he “regretted bitterly and still regret” not inoculating the boy, adding, “This I mention for the sake of parents who omit that operation, on the supposition that they should never forgive themselves if a child died under it; my example showing that the regret may be the same either way, and that, therefore, the safer should be chosen.”
A scientific perspective
A final lesson from 1721 has to do with the importance of a truly scientific perspective, one that embraces science, facts and objectivity.
Smallpox was characterized by fever and aches and pustules all over the body. Before eradication, the virus killed about 30% of those it infected, according to the U.S. Centers for Disease Control and Prevention. Sepia Times/Universal Images Group via Getty Images
Inoculation was a relatively new procedure for Bostonians in 1721, and this lifesaving method was not without deadly risks. To address this paradox, several physicians meticulously collected data and compared the number of those who died because of natural smallpox with deaths after smallpox inoculation. Boylston essentially carried out what today’s researchers would call a clinical study on the efficacy of inoculation. Knowing he needed to demonstrate the usefulness of inoculation in a diverse population, he reported in a short book how he inoculated nearly 300 individuals and carefully noted their symptoms and conditions over days and weeks.
The recent emergency-use authorization of mRNA-based and viral-vector vaccines for COVID-19 has produced a vast array of hoaxes, false claims and conspiracy theories, especially in various social media. Like 18th-century inoculations, these vaccines represent new scientific approaches to vaccination, but ones that are based on decades of scientific research and clinical studies.
We suspect that if he were alive today, Benjamin Franklin would want his example to guide modern scientists, politicians, journalists and everyone else making personal health decisions.Like Mather and Boylston, Franklin was a scientist with a respect for evidence and ultimately for truth.
When it comes to a deadly virus and a divided response to a preventive treatment, Franklin was clear what he would do. It doesn’t take a visionary like Franklin to accept the evidence of medical science today.
Health officials are grappling with how to prevent potential COVID-19 outbreaks from the delta variant that is spreading rapidly across the U.S.
Concern over the highly transmissible delta strain prompted Los Angeles County this week to recommend that all people wear masks indoors, even if they’re vaccinated. The World Health Organization (WHO) has also encouraged fully vaccinated people to continue using masks.
But the Centers for Disease Control and Prevention (CDC) has not signaled any plans to revise its mask guidance, with Biden administration officials and some experts say that fully vaccinated Americans are safe from all existing COVID-19 variants.
“If you have been vaccinated, the message we’re conveying is you’re safe,” White House press secretary Jen Psaki said Wednesday. “Vaccines are effective, and that is something we want to be very clear with the public about.”
Still, the move by officials in Los Angeles County raises the prospect that mask recommendations and even mandates could make a return to certain parts of the country.
The CDC projected the delta variant made up more than a quarter of cases in the U.S. in the most recent two-week period, ending June 19 — a jump from 10 percent the previous two weeks.
Los Angeles County issued a statement Monday saying it “strongly recommends” all people wear masks in indoor settings where they don’t know everyone’s vaccination status.
Barbara Ferrer, director of the county’s Department of Public Health, told The Hill that officials want to take time to get more people vaccinated as research is conducted on delta variant transmission from the fully vaccinated.
“While we’re doing that work with building confidence, we’re going to go ahead and offer as much protection as possible for everyone,” she said.
Leana Wen, an emergency physician and public health professor at George Washington University, praised the county’s decision as the “right move,” saying she hopes other jurisdictions follow suit to protect both vaccinated and unvaccinated residents.
“People who are fully vaccinated are still at risk, albeit a low risk, from those who are unvaccinated,” Wen said.
“Fully vaccinated people can be around others who are fully vaccinated without any limitations,” she added. “However, if they’re going to be around unvaccinated people or vaccination status is not being checked, then those could be high-risk settings” where masks should be worn.
For now, Los Angeles County is an outlier as cities and states continue to loosen mask requirements. Washington’s King County, home to Seattle, and Pennsylvania were the latest jurisdictions to end their mandates, taking that step this week.
CDC Director Rochelle Walensky told NBC’s “Today” on Wednesday that the agency’s guidance that fully vaccinated people don’t need masks in most settings has not changed. She said the WHO has given conflicting instructions, saying the international organization is focused on the global community, which has a lower vaccination rate than the U.S.
“We have always said that local policymakers need to make policies for their local environment,” Walensky said. “But those masking policies are not to protect the vaccinated, they’re to protect the unvaccinated.”
So far, the delta strain has not led to any changes in masking policies at the White House or the Capitol.
The White House does not require masks if a person is vaccinated, although the administration is not checking to see whether all maskless people have gotten their COVID-19 shots.
In recent weeks, the House has ended its universal mask requirement, and few people in the Capitol continue to wear them. The overwhelming majority of lawmakers in both parties have shed masks and freely gather in large groups on the House floor.
The Senate, which never had a mask requirement since nearly all senators voluntarily wore facial coverings when it was recommended, has also relaxed its pandemic restrictions.
But the delta variant threat is influencing other activities in the House. Speaker Nancy Pelosi (D-Calif.) announced this week that proxy voting would be extended through Aug. 17, and House Majority Leader Steny Hoyer (D-Md.) said that was due to the global spread of the delta variant.
“As we know, there are some countries in the world that are seeing a virulent resurgence of this new variant of the COVID-19. Israel is a perfect example of that,” Hoyer told reporters, referring to Israel reimposing its indoor mask mandate despite having one of the world’s highest vaccination rates. “But even in Israel, where they have the vaccine available, they’re seeing a resurgence.”
“So, the Speaker correctly, along with the medical advice that she’s gotten, determined that there was still justification for staying on guard,” Hoyer said.
Recent studies have found that COVID-19 vaccines are effective against the strain. Both doses of Pfizer-BioNTech were found to be 88 percent effective against symptomatic disease.
There is “less data” on how Johnson & Johnson performs, Walensky said Wednesday, but “right now we have no information to suggest that you need a second shot after J&J, even with the delta variant.”
Jen Kates, senior vice president and director of global health & HIV policy at the Kaiser Family Foundation, said research shows the CDC guidance “still stands,” although she acknowledged the agency needs to be prepared to adjust.
Kates expressed concern that the resurgence of the mask debate could affect the vaccination effort, noting the variant is spreading mostly among unvaccinated people.
“The worst outcome, I think, is that people choose not to get vaccinated because they think the vaccines aren’t as effective against variants,” she said.
As most Americans have gotten vaccinated, COVID-19 cases, hospitalizations and deaths have declined significantly. But the U.S. is expected to fall short of President Biden’s goal to have 70 percent of adults receiving at least one vaccine dose by the Fourth of July.
The White House still plans to move forward with Independence Day festivities. The administration sent 1,000 invitations for people to gather at 1600 Pennsylvania Ave. on Sunday, with vaccinated people allowed to go without masks. All guests were instructed to get tested one to three days before arriving.
“We certainly feel comfortable and confident moving forward with our event here at the White House and individuals having barbecues in their backgrounds this week to celebrate the Fourth of July,” Psaki said on Wednesday.
It’s “a trickle that will become a torrent,” Ashish Jha, dean at Brown University’s School of Public Health, tweeted.
More hospitals are likely to require employees receive a COVID-19 vaccine, experts said, to further protect the sick and vulnerable patients who rely on them for care.
A Houston-area hospital captured headlines after taking a firm stance on requiring vaccines that prevent severe illness of the coronavirus, which has killed more than 600,000 in the U.S. and ravaged the economy.
Houston Methodist employees who refused the vaccine were either terminated or resigned. A judge earlier this month sided with the hospital and tossed out an employee lawsuit that was seeking to block the mandated inoculation. The ruling may give other hospitals the green light to require the jab, and as more facilities put a similar policy in place, others are likely to follow, experts said.
It’s “a trickle that will become a torrent,” Ashish Jha, professor and dean at Brown University’s School of Public Health, posted Thursday on Twitter.
3 large health systems in Massachusetts to require all workers to be vaccinated.
Given the critical need to protect vulnerable patients, its critical all hospitals do this.
Some of the nation’s largest health systems have yet to mandate the shot, including Kaiser Permanente and CommonSpirit Health.
“Vaccination will only be required for Kaiser Permanente employees if a state or county where we operate mandates the vaccine for health care workers,” the company said in an email.
The American Hospital Association continues to hear that a growing number of its members are requiring the vaccine, with some exemptions. However, many member hospitals are waiting until the FDA grants full approval, a time when more safety and efficacy data will be made available.
“Getting vaccinated is especially critical for health care professionals because they work with patients with underlying health conditions whose immune systems may be compromised,”AHA, which has not taken on stance on the requirement, said in a statement.
The mandates raise ethical questions, some say, pointing to the profession’s promise to “do no harm.”
Arthur Caplan, head of medical ethics at New York University School of Medicine, said the codes of ethics that doctors and nurses says to put patients first, do no harm and protect the vulnerable.
“Of course they should be vaccinated,” he said. “If they don’t want to get vaccinated, I think they’re in the wrong profession.”
The Equal Employment Opportunity Commission said employment law does not prohibit employers from requiring the jab, essentially giving the green light to employers to put incentives and requirements in place for their workers. The EEOC is the federal agency tasked with ensuring that workplaces do not discriminate.
Some states are going against the tide and signing legislation that bars vaccine mandates, including Florida. The city of San Francisco will require hospital employees and workers in high-risk settings to get the vaccine. San Francisco, like other employers and universities, will require all city workers get inoculated.
The differing policy stances across the country creates additional hurdles for corporations with a large footprint.
As the delta variant of the coronavirus spreads, especially among the unvaccinated, the Biden administration is gearing up for a new push to vaccinate the so-called “movable middle”—and some public health experts say FDA could advance that goal by fully approving Covid-19 vaccines.
Analysis reveals toll of US Covid-19 deaths among unvaccinated patients
According to an analysis by the Associated Press, nearly all recent Covid-19 deaths have occurred in unvaccinated individuals.
The AP analysis is based on data from CDC, although CDC has not itself released estimates of the share of Covid-19 deaths among unvaccinated patients.
According to the AP analysis, just 0.8% of Covid-19 deaths in May were among the fully vaccinated. Meanwhile, the share of hospitalized patients who were fully vaccinated was just 0.1% in May, with fewer than 1,200 fully vaccinated people hospitalized out of more than 853,000 hospitalizations.
Meanwhile, according to CDC, 54% of the U.S. population, including 66% of American adults, have received at least one dose of a Covid-19 vaccine, while 46.1% of the total population and 56.8% of American adults have received all required doses.
In many places across the United States, COVID-19 feels over. Unmasked citizens run rampant. New York City is planning an August mega-concert in Central Park. I’m as hopeful as the rest of us, but I think we may be suffering from memory loss.
Let’s start from this time last year, when many Americans were exuberantly returning to newly reopened beaches, parks and restaurants after a seemingly eternal three months—three whole months!—of quarantine. Universal observance of safety guidelines was surely going to be sufficient to limit viral spread.
We know how that turned out. By mid-June 2020, there were already signs that our bleary-eyed re-emergence was premature. On June 22, 2020, the number of new daily cases of COVID-19 (33,485) surpassed the high-water mark hit on the worst day of the horrific first surge, when that figure peaked at just over 32,000.
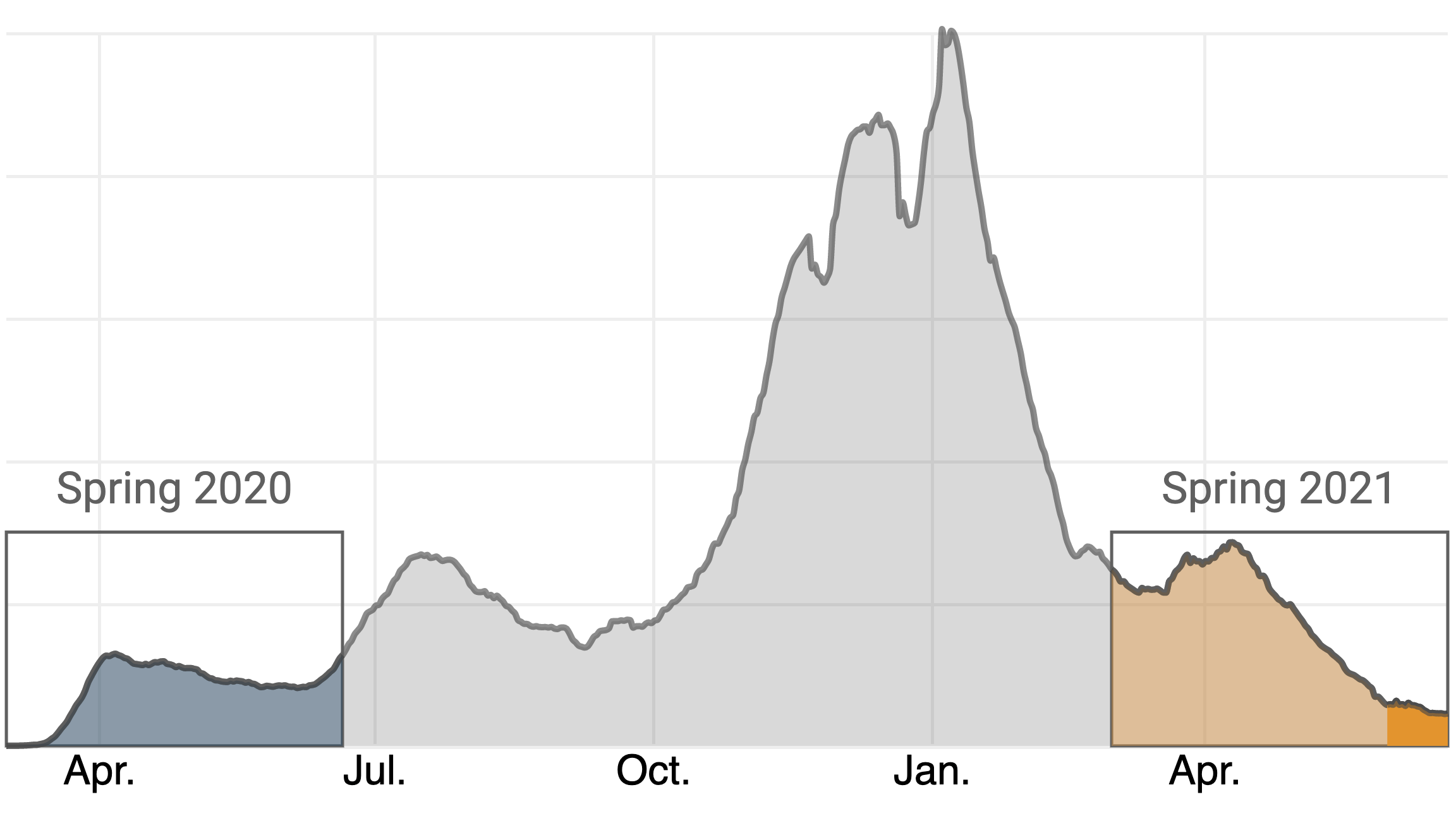
A year later, the daily case count is not as foreboding—nor is it nearly as low it may appear.
You’ll notice that this graph covers only the past 12 weeks, while virtually every chart you’ll find (including the one on TIME’s dashboard) graphs COVID-19 cases from the beginning of the outbreak. This is intentional. The toll of the pandemic in the U.S. has persisted for so long, and reached such catastrophic heights in the first weeks of 2021, that patterns such as this one are nearly impossible to see on the typical chart. Here’s what the same graph looks like against that backdrop:
My fear is that the pandemic remains much more deadly than how it looks on the page. Yes, deaths remain on a steady decline, having recently sunk below 300 people a day on average for the first time since March 24, 2020, right around the time that many offices were shuttering. But a surge in cases, particularly among the large number of unvaccinated Americans, could quickly reverse that decline.
As you can see, it has been less than a month since the 2021 case count sunk below the year-over-year figure, on May 26. The massive nationwide vaccine rollout is undoubtedly a major factor, but it’s difficult to quantify the impact of vaccination on the currently low case and death figures. There are only weak correlations between states’ vaccination rates and some key indicators, like the rate at which cases have risen or fallen in recent weeks.
What we can quantify is that, in the 27 days since the lines crossed, the vaccination rate in the U.S. has only crawled upward, from 39.7% to 45.3% of Americans who have received a complete dosage. While the official vaccination rate applies to the entire population, data from the U.S. Centers for Disease Control and Prevention (CDC) also includes percentages for several age groups. By TIME’s calculations, there are 97.4 million adults age 18 and over who have been eligible for vaccination for two months but who have not yet received even a first dose. This group trends heavily younger, with those 65 and over representing only 7.8% of the unvaccinated population. (These figures do no include those under 18, who constitute a small portion of the eligible population.)
On May 13, two weeks before daily case numbers in 2021 fell below the year-over-year figures from the same day in 2020, the CDC issued guidance liberating fully vaccinated individuals from wearing masks in many scenarios. I do not have conclusive proof that any of the country’s 97.4 million unvaccinated adults have abused this privilege. All I can state with confidence is that, based on the number of people I’ve seen not wearing a mask in places like stores, which often have signs imploring those who are not fully vaccinated to continue to mask up, it is mathematically almost certain that more than a few have done so.
Which is to say: the situation today, if one can momentarily rewind to Memorial Day of 2020, feels very familiar. There appears to be a lambent light at the end of the tunnel, yet cavalier attitudes towards the pandemic, particularly among younger people who, as a group, are under-vaccinated, resembles what we saw last summer just before the second wave.
Watching these trends, I grow more concerned every day that the country is positioned for yet another surge in cases, despite our defensive upgrades in the off-season. I hope I’m wrong, but the numbers are not nearly as comforting as they first look. The fact that the Delta variant, which is both more transmissible and appears to cause more severe disease, is on pace to become the dominant form of COVID-19 in the U.S. in the coming months is further reason for alarm. Moreover, some states have significantly higher vaccination rates than others, leaving those with less protection more vulnerable to future spikes.
Forgive me for being a buzzkill, but unless we can institute a functional vaccine passport system, which appears unlikely, I do not think it is wise to assume that every unmasked individual is fully dosed. Short of a passport system, and with dangerous variants competing for dominance and the duration of vaccine protection still unclear, we ought to continue to ration physical space in public areas—a policy that is hastily being relaxed at places like Major League Baseball parks. I love baseball and eagerly look forward to buzzing up to Philadelphia to take in a game at Citizen’s Bank Park, which is operating at full capacity. But not while the policy is that “Unvaccinated fans are strongly encouraged to wear their masks in all indoor and outdoor areas in and around the ballpark.”
I also think there might be a backdoor to a digital passport system. Based on polling data, it appears there is a substantial population of people who aren’t categorically opposed to vaccination, just unmotivated to get around to it—what we’ve termedvaccine “meh-sitance,” not hesitance. My proposal is that bars, restaurants and other popular venues merely require each person who enters to verbally affirm that they are fully vaccinated.
This might sound about as effective as asking passengers in the exit row to individually verify that they listened to the instructions. But while it’s one thing to ignore a sign at the grocery store, it’s another to lie in front of your friends. Peer pressure is a powerful motivator, and if even a fraction of the unvaccinated would take the time to resolve that dissonance, or risk missing out on trivia night, it could substantially push up the percentages. I call this the “FOMO method,” and though we are still a long, long way from eliminating the disease altogether, it could help us avert a fourth wave this summer.
The World Health Organization said Monday that the coronavirus variant first identified in India last year will be reclassified as a “variant of concern,” indicating that it has become a global health threat.
The B.1.617 variant has been found to spread more easily than the original virus, with some evidence indicating that it may evade some of the protections provided by the vaccines, according to a preliminary study. But the shots are still considered effective. The agency will provide more details on Tuesday.
The highly contagious, triple-mutant variant is also the fourth variant to be designated as a global concern, prompting enhanced tracking and analysis. The other variants are those first detected in Britain, South Africa and Brazil.
“We are classifying this as a variant of concern at a global level,” said Maria Van Kerkhove, WHO technical lead on COVID-19, per Reuters. “There is some available information to suggest increased transmissibility.”
A variant is labeled as “of concern” if it is shown to be more contagious, more deadly or more resistant to current vaccines and treatments, according to the WHO.
The global agency said the predominant lineage of B.1.617 was first identified in India in December, although an earlier version was spotted in October 2020.
The variant has already spread to other countries, and many nations – including the U.S. – have moved to end or restrict travel from India.
“Even though there is increased transmissibility demonstrated by some preliminary studies, we need much more information about this virus variant and this lineage and all of the sub-lineages,” said Maria Van Kerkhove, the WHO’s technical lead for COVID-19.
India reported a record-high of daily coronavirus cases, averaging about 391,000 new daily cases and about 3,879 deaths per day, according to Johns Hopkins University data.
LIMA, Peru — The doctor watched the patients stream into his intensive care unit with a sense of dread.
For weeks, César Salomé, a physician in Lima’s Hospital Mongrut, had followed the chilling reports. A new coronavirus variant, spawned in the Amazon rainforest, had stormed Brazil and driven its health system to the brink of collapse.Now his patients, too, were arriving far sicker, their lungs saturated with disease, and dying within days. Even the young and healthy didn’t appear protected.
The new variant, he realized, was here.
“We used to have more time,” Salomé said. “Now, we have patients who come in and in a few days they’ve lost the use of their lungs.”
The P.1 variant, which packs a suite of mutations that makes it more transmissible and potentially more dangerous, is no longer just Brazil’s problem. It’s South America’s problem — and the world’s.
In recent weeks, it has been carried across rivers and over borders, evading restrictive measures meant to curb its advance to help fuel a coronavirus surge across the continent. There is mounting anxiety in parts of South America that P.1 could quickly become the dominant variant, transporting Brazil’s humanitarian disaster — patients languishing without care, a skyrocketing death toll — into their countries.
“It’s spreading,” said Julio Castro, a Venezuelan infectious-disease expert. “It’s impossible to stop.”
In Lima, scientists have detected the variant in 40 percent of coronavirus cases. In Uruguay, it’s been found in 30 percent. In Paraguay, officials say half of cases at the border with Brazil are P.1. Other South American countries — Colombia, Argentina, Venezuela, Chile — have discovered it in their territories. Limitations in genomic sequencing have made it difficult to know the variant’s true breadth, but it has been identified in more than two dozen countries, from Japan to the United States.
Hospital systems across South America are being pushed to their limits. Uruguay, one of South America’s wealthiest nations and a success story early in the pandemic, is barreling toward a medical system failure. Health officials say Peru is on the precipice, with only 84 intensive care beds left at the end of March. The intensive care system in Paraguay, roiled by protests last month over medical shortcomings, has run out of hospital beds.
“Paraguay has little chance of stopping the spread of the P.1 variant,” said Elena Candia Florentín, president of the Paraguayan Society of Infectious Diseases.
“With the medical system collapsed, medications and supplies chronically depleted, early detection deficient, contact tracing nonexistent, waiting patients begging for treatment on social media, insufficient vaccinations for health workers, and uncertainty over when general and vulnerable populations will be vaccinated, the outlook in Paraguay is dark,” she said.
How P.1 spread across the region is a distinctly South American story. Nearly every country on the continent shares a land border with Brazil. People converge on border towns, where crossing into another country can be as simple as crossing the street. Limited surveillance and border security have made the region a paradise for smugglers. But they have also made it nearly impossible to control the variant’s spread.
“We share 1,000 kilometers of dry border with Brazil, the biggest factory of variants in the world and the epicenter of the crisis,” said Gonzalo Moratorio, a Uruguayan molecular virologist tracking the variant’s growth. “And now it’s not just one country.”
The Brazilian city of Tabatinga, deep in the Amazon rainforest, where officials suspect the virus crossed into Colombia and Peru, is emblematic of the struggle to contain the variant. The city of 70,000 was swept by P.1 earlier this year. Many in the area have family ties in several countries and are accustomed to crossing borders with ease — canoeing across the Amazon River to Peru or walking into Colombia.
“People ended up bringing the virus from one side to the other,” said Sinesio Tikuna Trovão, an Indigenous leader. “The crossing was free, with both sides living right on top of one another.”
Now that the variant has infiltrated numerous countries, stopping its spread will be difficult. Most South American countries, with the exception of Brazil, adopted stringent containment measures last year. But they have been undone by poverty, apathy, distrust and exhaustion. With national economies battered and poverty rising sharply, public health experts fear more restrictions will be difficult to maintain. In Brazil, despite record death numbers, many states are lifting restrictions.(SOUND FAMILIAR)
That has left inoculation as the only way out. But coronavirus vaccines are South America’s white whale: often discussed, but rarely seen. The continent hasn’t distributed its own vaccine or negotiated a regional agreement with pharmaceutical companies. It’s one of the world’s hardest-hit regions but has administered only 6 percent of the world’s vaccine doses, according to the site Our World in Data. (The outlier is Chile, which is vaccinating residents more quickly than anywhere in the Americas — but still suffering a surge in cases.)
“We should not only blame the policy response,” said Luis Felipe López-Calva, the United Nations Development Program’s regional director for Latin America and the Caribbean. “We have to understand the vaccine market.”
“And there is a failure in the market,” he said.
The vaccine has become so scarce, López-Calva said, that officials are imposing restrictions on information. It’s nearly impossible to know how much governments are paying for doses. Some regional blocs, such as the African Union and the European Union, have negotiated joint contracts. But in South America, it has been every country for itself — diminishing the bargaining power for each one.
“This has been harmful for these countries, and for the whole world to stop the virus,” López-Calva said. “Because it’s never been more clear that no one is protected until everyone is protected.”
Paulo Buss, a prominent Brazilian scientist, said it didn’t have to be like this. He was Brazil’s health representative to the Union of South American Nations, which negotiated several regional deals with pharmaceutical companies before the coronavirus pandemic. But that union came apart amid political differences just before the arrival of the virus.
“It was the worst possible moment,” Buss said. “We’ve lost capacity and our negotiation attempts have been fragmented. Multi-lateralism was weakened.”
Vaccine scarcity has led to line-jumping scandals all over South America, but particularly in Peru. Hundreds of politically connected people, including cabinet ministers and former president Martín Vizcarra, snagged vaccine doses early. Now people are calling for criminal charges.
As officials bicker and the vaccination campaign is delayed, the variant continues to spread. P.1 accounts for 70 percent of cases in some parts of the Lima region, according to officials. Last week, the country logged the highest daily case count since August — more than 11,000. On Saturday, the country recorded 294 deaths, the most in a day since the start of the pandemic.
Peruvians have been stunned by how quickly the surge overwhelmed the health-care system. Public health analysts and government officials had believed Peru was prepared for a second wave. But it wasn’t ready for the variant.
“We did not expect such a strong second wave,” said Percy Mayta-Tristan, director of research at the Scientific University of the South in Lima. “The first wave was so extensive. The presence of the Brazilian variant helps explain why.”








{kind=link}